deep brain stimulation (DBS) for sustained tremor control? • Christian Hartmann • Irvine Cooper • Stefan Groiss • Christian McDonough • What is the most important aspect of an awake craniotomy? • Premedication with midazolam • Sedation with precedex and propofol • Patient selection and preparation • Cortical mapping • Which of the following is not one of the Major anesthetic challenges for awake craniotomy? • Smooth transition of anesthetic depth based on different surgical stages • Maintenance of cerebral hemodynamic and cardiopulmonary function • Crisis management of awake patient • Central line access
Parkinson disease, essential tremor, dystonias • DBS has become one of the most successful treatment strategies in advanced stages of the disease • Only for patients with PD, not secondary or atypical Parkinsonian syndromes • Target the subthalamic nucleus, internal segment of globus pallidus, or ventral intermediate nucleus of thalamus • Advantages – adaptability, reversibility, less tissue damage, option to perform b/l surgery • Criteria: • Motor fluctuations • Tremor, not satisfactorily treated with medication • Levodopa-induced reduction of motor symptoms by >33% • Exclusion of dementia, relevant psychiatric or somatic comorbidity, or general contraindication
cortical areas required for speech of motor function • Very important to educate patient about duration and nature of the procedure • Asleep-awake-asleep technique with intermittent airway management • Essential element is local anesthetic technique • Anesthetic technique • Minimize patient discomfort • Ensure patient compliance • Technique that produces minimal inhibition of spontaneous seizure activity
NIBP monitoring • Arterial line may be warranted in some cases • Utmost importance is patient comfort • Positioning - as much 'sniff' as possible and clear access to patient's face • Emergent airway supplies on hand "just in case"
or dexmedetomidine infusions • Some use fentanyl v remifentanil • May use propofol + remifentanil + dexmedetomidine • Provocation of seizure activity may be required by administration methohexital, etomidate or with hyperventilation • Propofol needs to be discontinued about 15 mins before EEG recording
bolus dose of dexmedetomine? • Decreased CO, decreased HR, decreased BP • Decreased CO, increased HR, decreased BP • Decreased CO, decreased HR, increased BP • Increased CO, decreased HR, increased BP • Which of the following do NOT act at the GABA A receptor? • Propofol • Gabapentin • Benzodiazepines • Etomidate
and spinal cord • Adequate surgical conditions • Bed at 15-30 degrees to facilitate venous drainage • Avoid sedatives and/or opiates if elevated ICP is a concern • Maintain normal electrolytes • Fluid of choice is 0.9% Normal Saline • Most often IV anesthetic preferred over volatile anesthetic
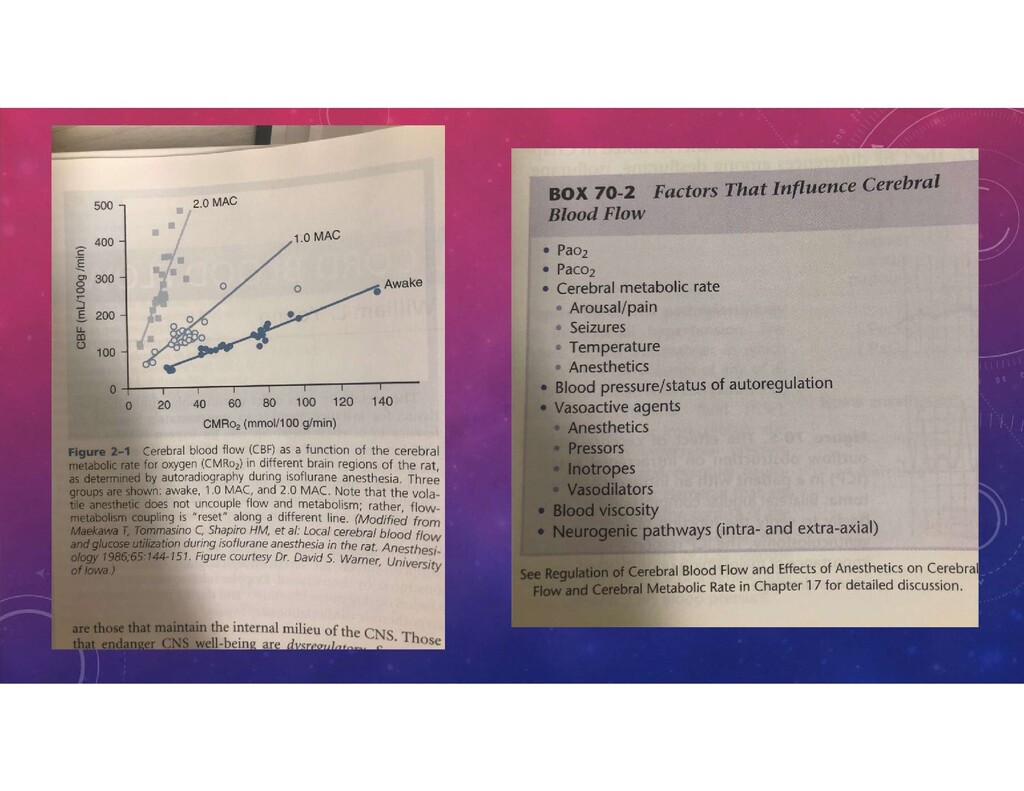
• Utilizes over 20% of total oxygen metabolism • Neurovascular coupling – CBF, blood volume, glucose consumption and oxygen metabolism all increased within localized regions of activity • Neurons consume 75-80% of energy produced in the brain • Cerebral vessels respond by mechanisms involving nitric oxide, prostaglandins, vasoactive peptides, potassium channels, and endothelin
controls expiration during the normal physiologic state? • Pons, lower pontine apneustic center • Medulla, ventral respiratory group • Pons, upper pontine pneumotaxic center • Medulla, dorsal respiratory group • Which of the following are true? • The brain metabolizes fatty acids for energy in states of severe starvation • The brain obtains most of its energy from ketone bodies in states of severe starvation • Under normal circumstances, the brain utilizes glucose and ketone bodies for energy.
of pathology and/or anesthetics • CBF changes are directly proportional to PaCO2 • Volatile Anesthetics lead to uncoupling of CBF/CMRO2 • IV Anesthetics decrease CBF and decrease CMRO2 • Benzos decrease CMRO2, little effect on CBF • Succinylcholine – controversial but believed to increase CBF which can increase ICP • Opioids have minimal effects on CMRO2 and no effect on CBF unless rapid infusion
on CBF and CMRO2 on a normal brain? • Increased CBF and increased CMRO2 • Increased CBF and decreased CMRO2 • Decreased CBF and decreased CMRO2 • Decreased CBF and increased CMRO2 • What is the order of volatile anesthetic dose dependent increase in CBF due to vasodilation? • Sevoflurane > Desflurane > Isoflurane > Halothane • Isoflurane > Sevoflurane > Desflurane > Halothane • Halothane > Desflurane > Isoflurane > Sevoflurane • Halothane > Sevoflurane > Isoflurane > Desflurane
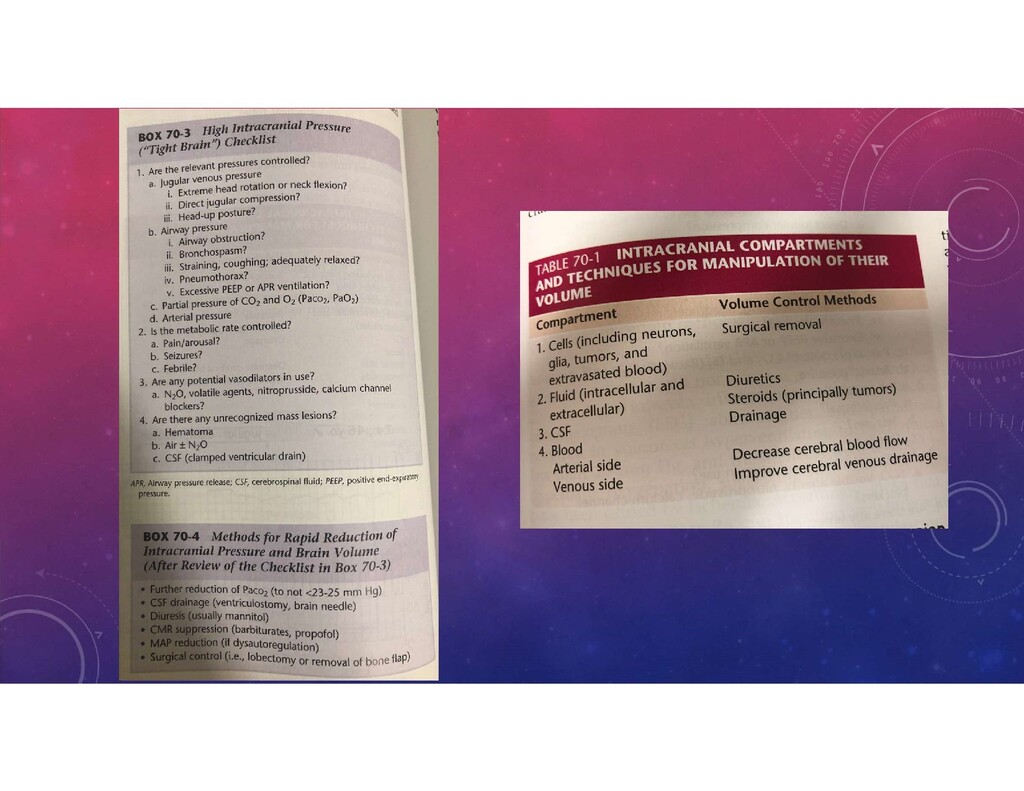
of the bed, oxygenation and ventilation to maintain PaO2 >100, PaCO2 30-35 • CSF drainage • Mannitol boluses at 0.25-1g/kg • 3% saline as similar effects as mannitol • Hyperventilation – but CBF drops 3-4% for every 1 mmHg decrease in PCO2
being most sensitive to effects of volatile anesthetics? • Motor evoked potentials • Brainstem evoked potentials • Visual evoked potentials • Somatosensory evoked potentials
and Dysautoregulation." Anesthesiology Clinics. 2016 Sept; 34(3): 465-477. • Burnand, Cally and Joseph Sebastian. "Anaesthesia for Awake Craniotomy." Continuing Education in Anaesthesia, Critical Care & Pain. 2014. Vol 14 (1): 6-11. • Cottrell, James E. MD and William L. Young MD. Cottrell and Young's Neuroanesthesia. 5th ed. 2010. • Hartmann, Christina J., Sabine Fliegen, Stefan J. Groiss, Lars Wojtecki and Alfons Schnitzler. "An Update on Best Practice of Deep Brain Stimulation in Parkinson's Disease." Ther Adv Neurol Disord. 2019, Vol 12: 1-20. • Miller, Ronald E. MD, MS. Miller's Anesthesia. 8th ed. 2015. P 2158-2196. • OpenAnethesia. • Sewell Darreul and Martin Smith. "Awake Craniotomy: Anesthetic Considerations Based on Outcome Evidence." Current Opin Anesthesiol. 2019, 32: 546-552.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}