to promote conversations between clinicians and patients by helping patients choose care that is: -Supported by evidence -Not duplicates of other tests or procedures already received -Free from harm -Truly necessary Beginning in 2012, national organizations representing medical specialists asked their members to identify tests or procedures commonly used in their field whose necessity should be questioned and discussed. There are over 70,000 ICD-10 procedure codes and over 69,000 ICD-10 diagnosis codes.
as part of pre- operative or pre-procedural evaluations for asymptomatic patients with low perioperative risk of death or myocardial infarction. Even for CAD patients, ECG is mainly for baseline comparison in OR but won’t predict complications. American Society of Anesthesiologists Don’t obtain baseline diagnostic cardiac testing (trans-thoracic/esophageal echocardiography – TTE/TEE) or cardiac stress testing in asymptomatic stable patients with known cardiac disease (e.g: CAD, valvular disease) undergoing low or moderate risk non-cardiac surgery. The Society of Thoracic Surgeons Patients who have no cardiac history and good functional status do not require preoperative stress testing prior to non-cardiac thoracic surgery. American Society of Echocardiography Avoid echocardiograms for preoperative/perioperative assessment of patients with no history or symptoms of heart disease.
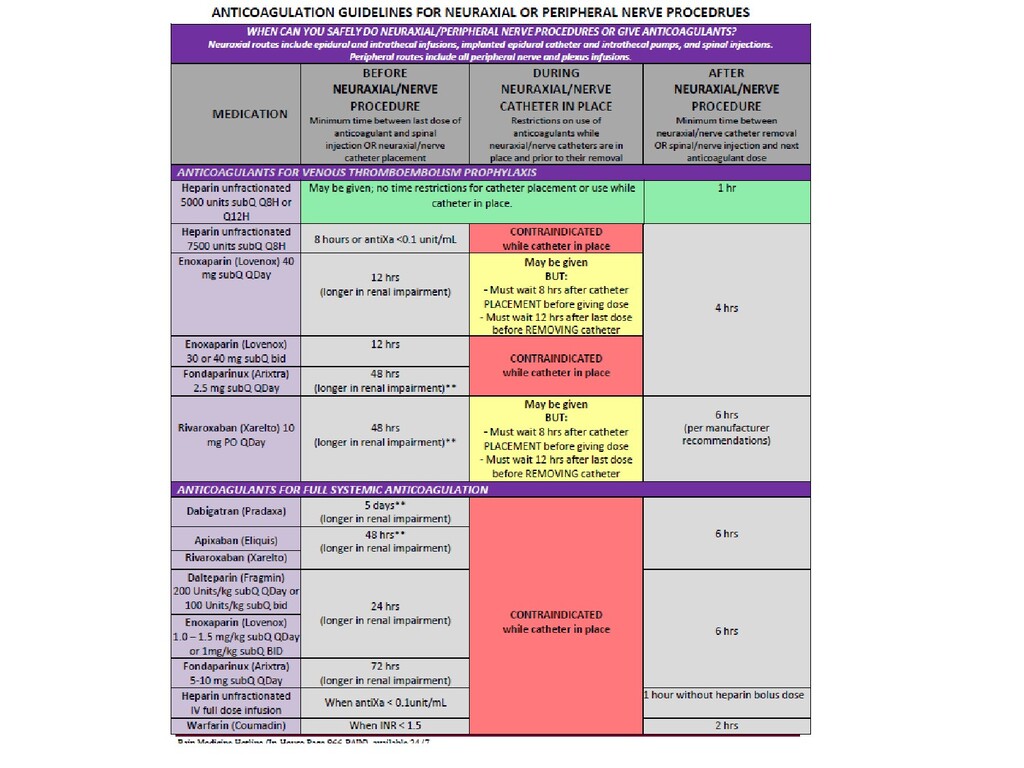
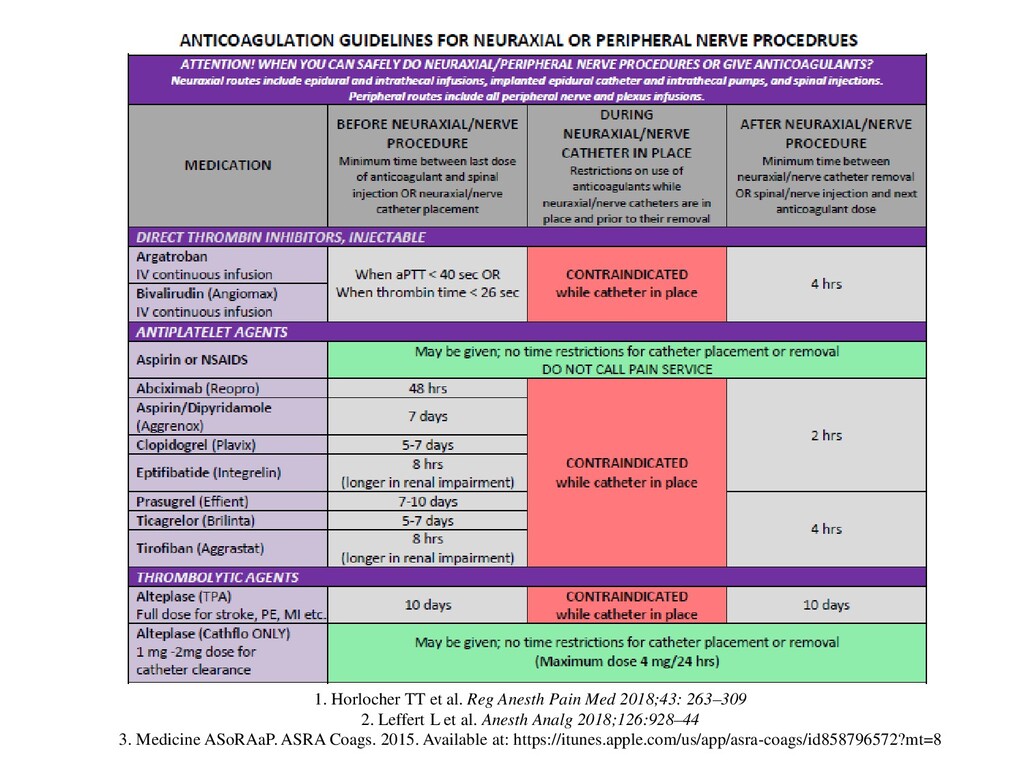
263–309 2. Leffert L et al. Anesth Analg 2018;126:928–44 3. Medicine ASoRAaP. ASRA Coags. 2015. Available at: https://itunes.apple.com/us/app/asra-coags/id858796572?mt=8
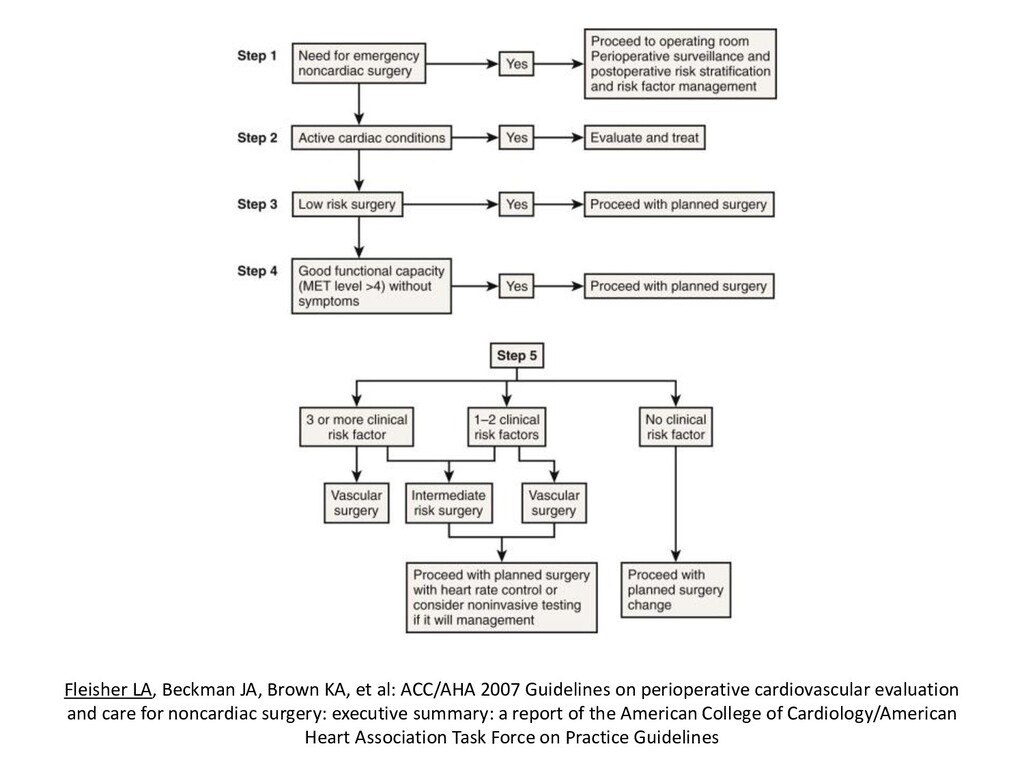
Guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines
type of anesthesia -Vague recommendations like “control BP,” “keep euvolemic” -Vague information (“pt has COPD, could benefit from pulmonary evaluation eventually,” “patient probably doesn’t have significant coronary disease”)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}