FNA: the safest and most accurate of diagnostic tools in thyroid tools in thyroid • • • • In experienced hands, and in situations where In experienced hands, and in situations where the pathologist performs the needling, cytology the pathologist performs the needling, cytology can be a very sensitive tool. can be a very sensitive tool. • • Sensitivity 94% Sensitivity 94% • • Specificity 75% Specificity 75% • • Positive predictive value 98% Positive predictive value 98%
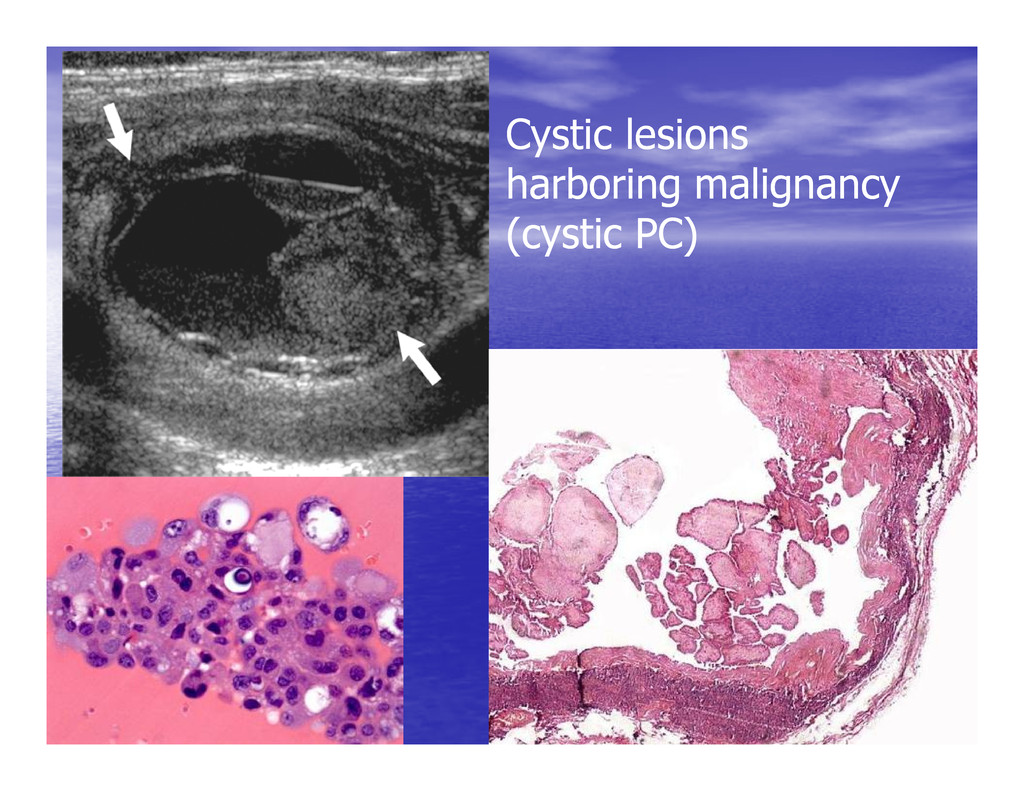
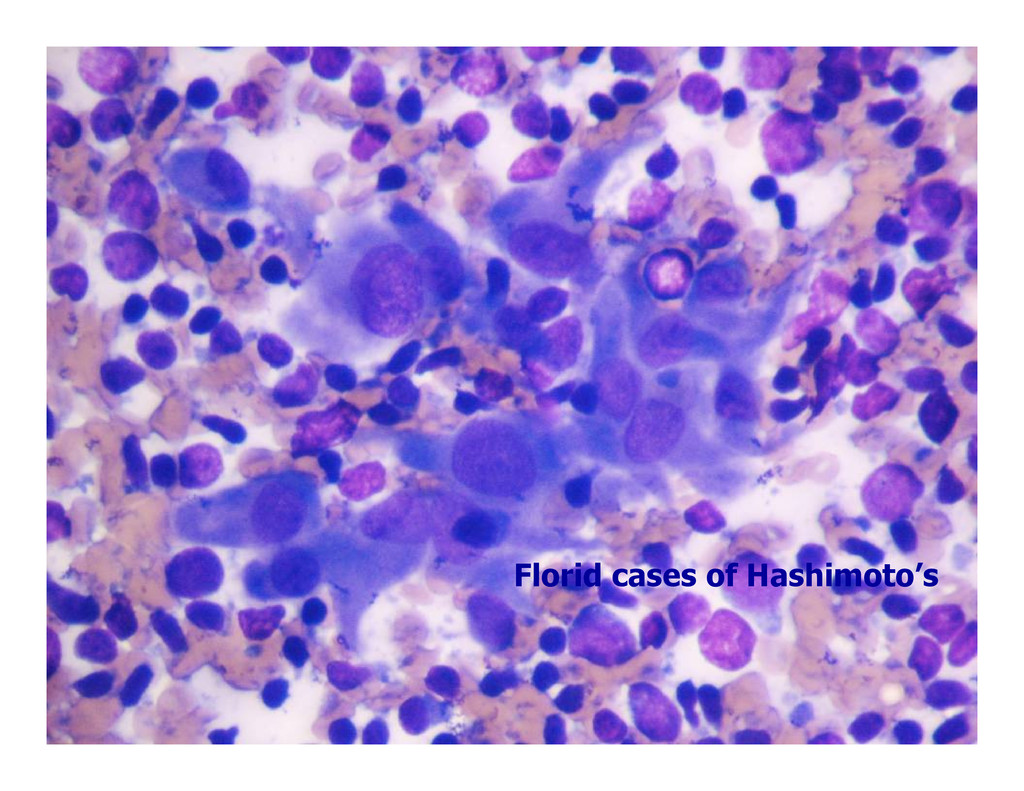
where the Cases with dual pathology where the dominant non dominant non- -neoplastic lesion neoplastic lesion dominant non dominant non- -neoplastic lesion neoplastic lesion overlies or obscures a small overlies or obscures a small carcinoma carcinoma
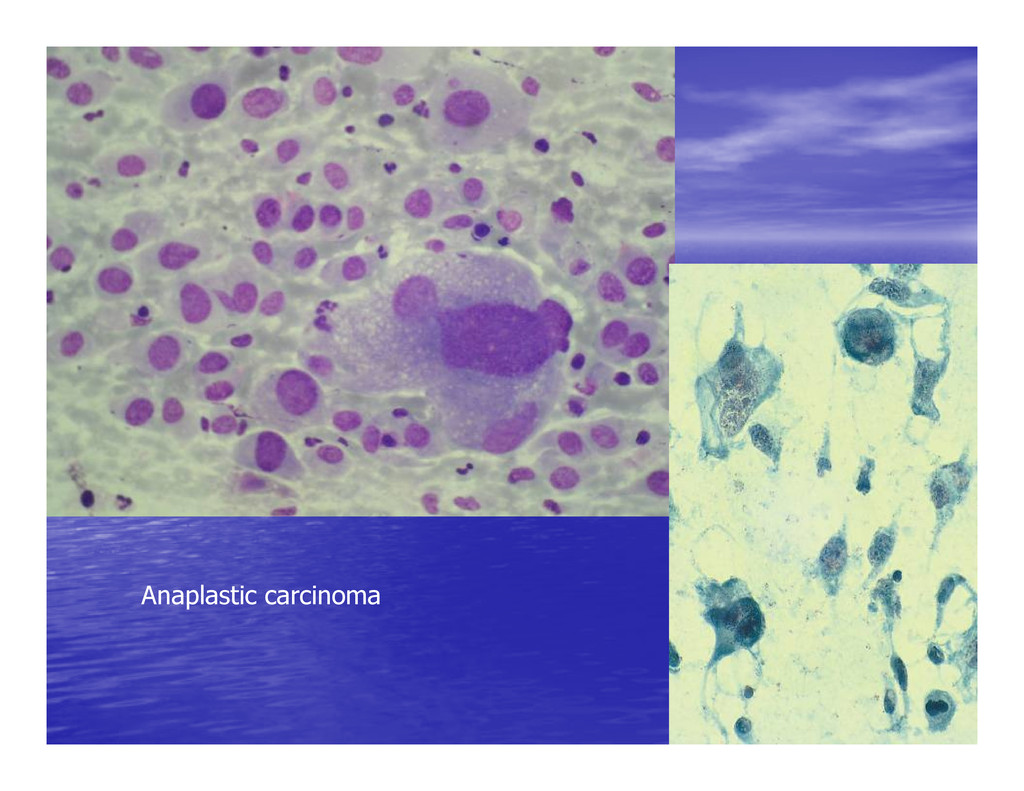
• • Evaluation of solitary thyroid nodules Evaluation of solitary thyroid nodules (with a view to (with a view to distinguish benign from malignant) distinguish benign from malignant) • • Evaluation of diffuse thyroid lesions Evaluation of diffuse thyroid lesions (with a view to (with a view to distinguish inflammatory/autoimmune lesions from distinguish inflammatory/autoimmune lesions from distinguish inflammatory/autoimmune lesions from distinguish inflammatory/autoimmune lesions from nodular goiter) nodular goiter) • • Confirmation and categorization of clinically obvious Confirmation and categorization of clinically obvious thyroid malignancy thyroid malignancy (especially anaplastic carcinomas (especially anaplastic carcinomas that may require preoperative palliative treatment, and that may require preoperative palliative treatment, and lymphoma and metastatic malignancy where surgery is lymphoma and metastatic malignancy where surgery is usually not indicated) usually not indicated)
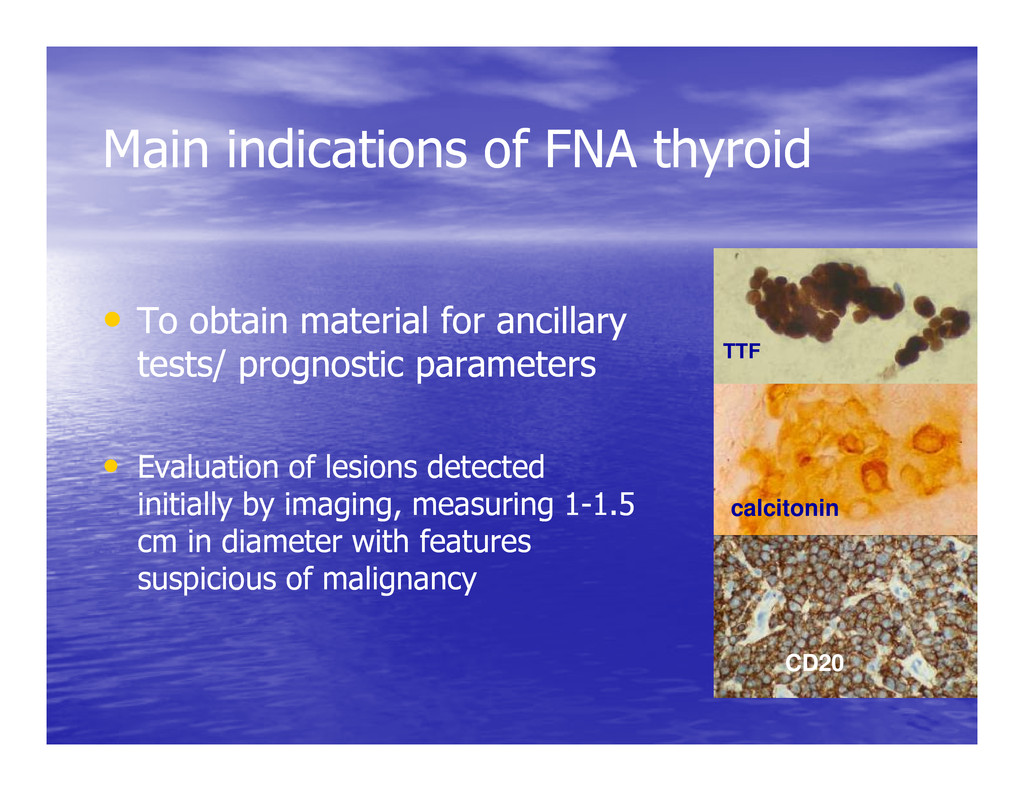
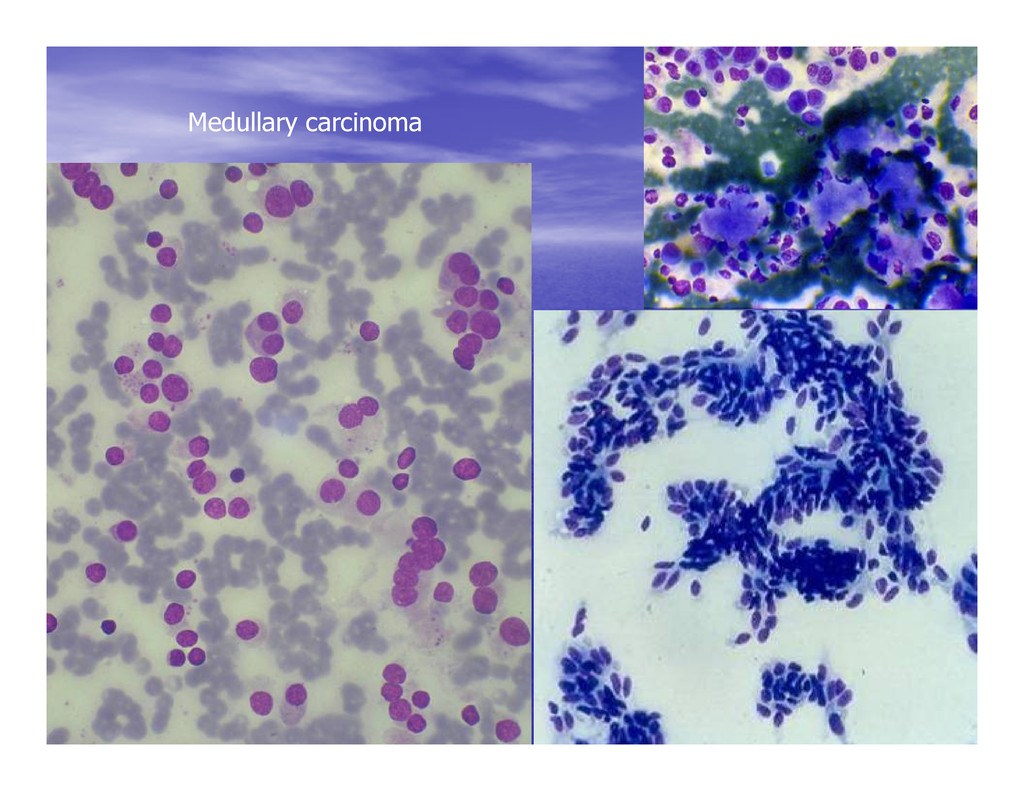
• • To obtain material for ancillary To obtain material for ancillary tests/ prognostic parameters tests/ prognostic parameters TTF • • Evaluation of lesions detected Evaluation of lesions detected initially by imaging, measuring 1 initially by imaging, measuring 1- -1.5 1.5 cm in diameter with features cm in diameter with features suspicious of malignancy suspicious of malignancy calcitonin CD20
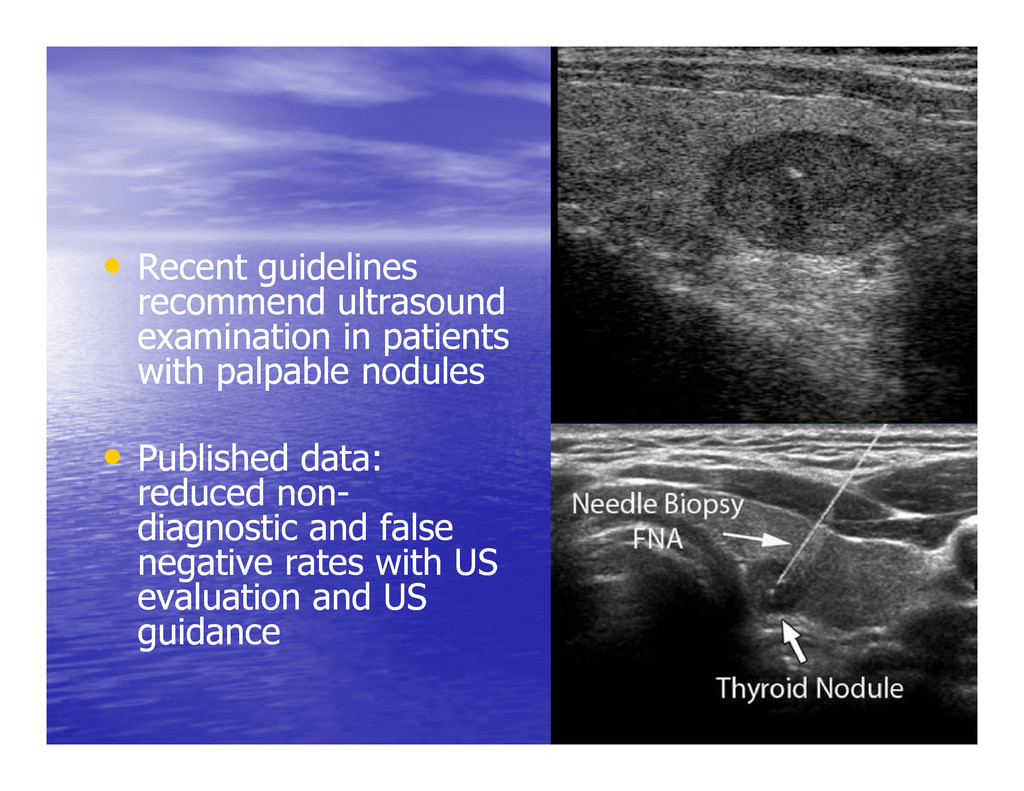
examination in patients examination in patients with palpable nodules with palpable nodules • • Published data: Published data: reduced non reduced non- - diagnostic and false diagnostic and false negative rates with US negative rates with US evaluation and US evaluation and US guidance guidance
and have been used to plan have been used to plan definitive surgery and other definitive surgery and other treatment protocols treatment protocols treatment protocols treatment protocols • •Cytological diagnosis is Cytological diagnosis is generally accurate in the generally accurate in the following: following:
operations are still performed unnecessarily for benign disease. • Many of these operations follow FNA cytology interpreted as follicular lesions in which follicular carcinoma could not be excluded.
preoperative obsessed with preoperative distinction of follicular distinction of follicular carcinoma (FC) from carcinoma (FC) from carcinoma (FC) from carcinoma (FC) from follicular adenoma (FA) follicular adenoma (FA) • • This has lead to the use of ancillary This has lead to the use of ancillary techniques (galectin 3, CD44v6, techniques (galectin 3, CD44v6, morphometry, AGNORs, ploidy analysis) morphometry, AGNORs, ploidy analysis)
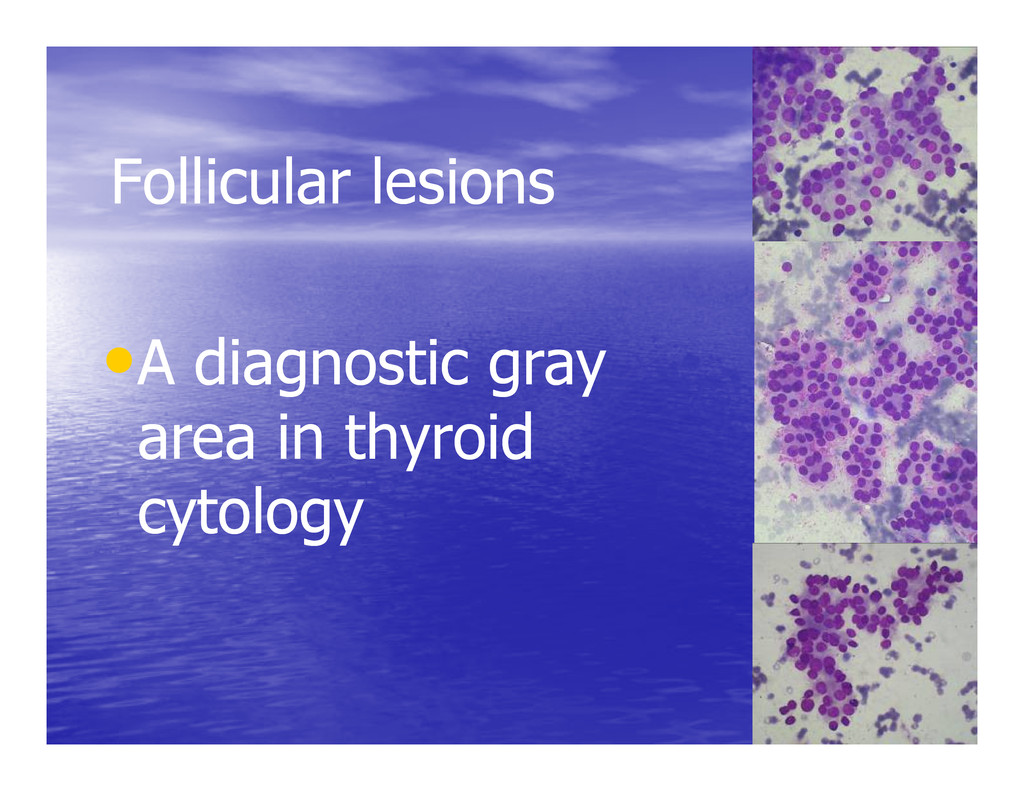
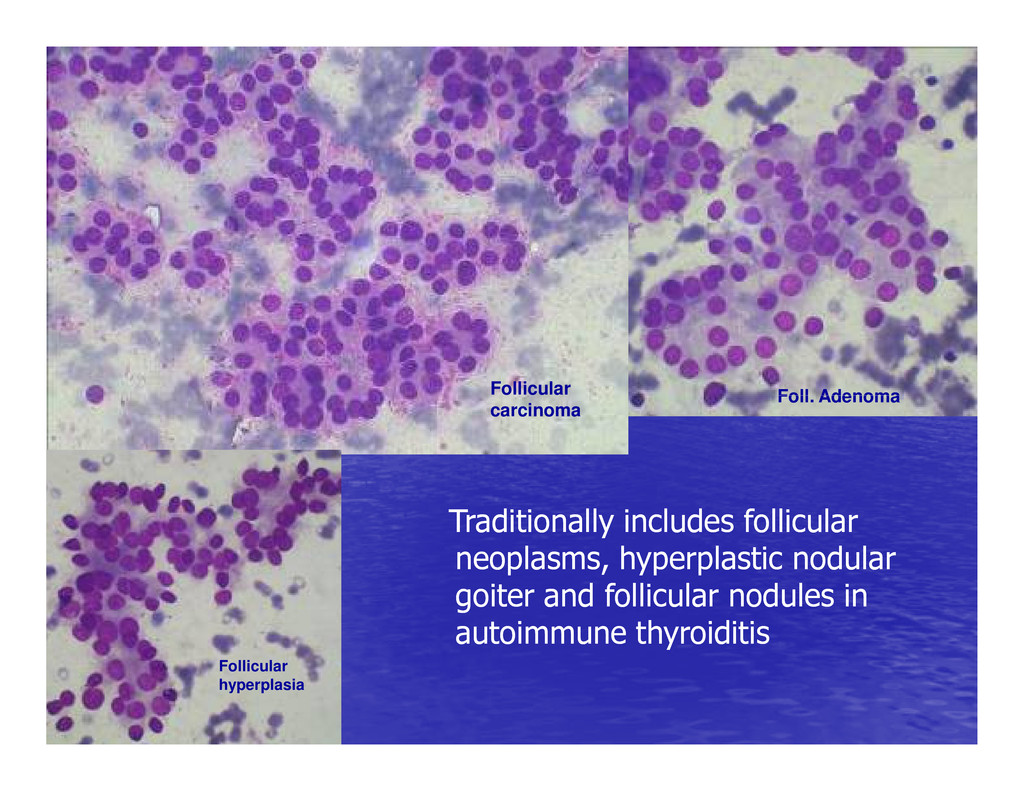
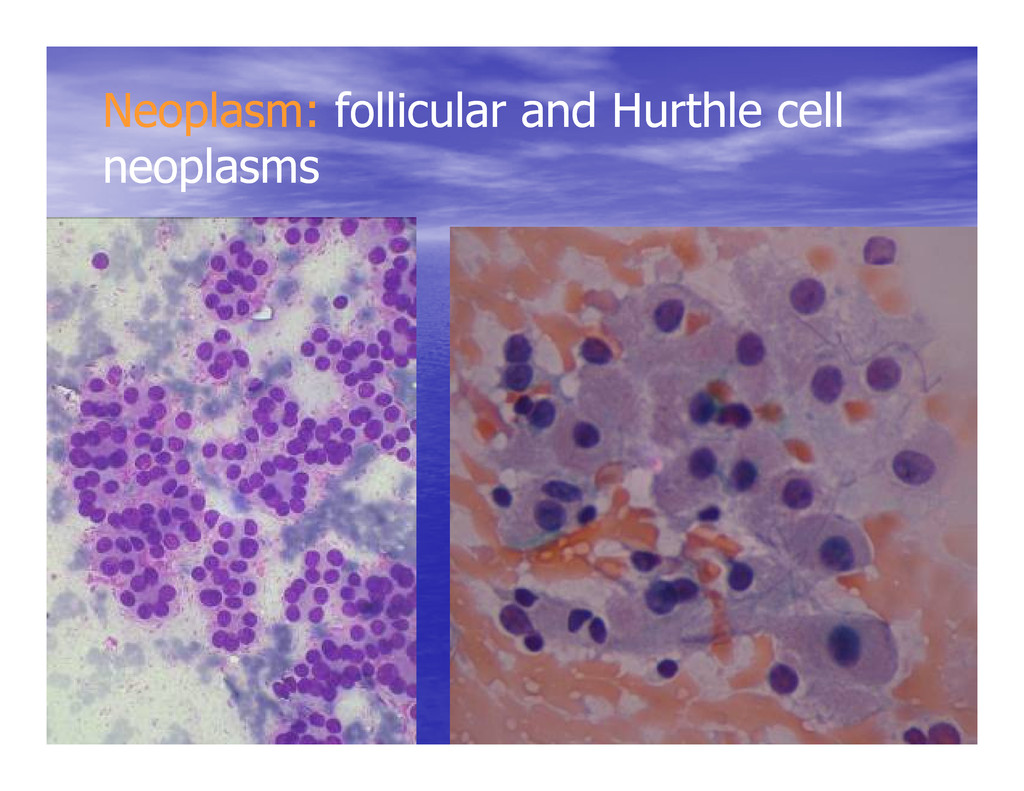
includes follicular Traditionally includes follicular neoplasms, hyperplastic nodular neoplasms, hyperplastic nodular goiter and follicular nodules in goiter and follicular nodules in autoimmune thyroiditis autoimmune thyroiditis
hyperplastic nodules from follicular neoplasms: a problem that extends to tissue neoplasms: a problem that extends to tissue pathology as well. pathology as well. Follicular lesions Follicular lesions • • Partially encapsulated hyperplastic nodules of Partially encapsulated hyperplastic nodules of goiter: not infrequently misdiagnosed goiter: not infrequently misdiagnosed histologically as follicular carcinoma. histologically as follicular carcinoma. • • Pseudo Pseudo- -encapsulated nodules of goiter are encapsulated nodules of goiter are sometimes misdiagnosed as follicular adenoma. sometimes misdiagnosed as follicular adenoma.
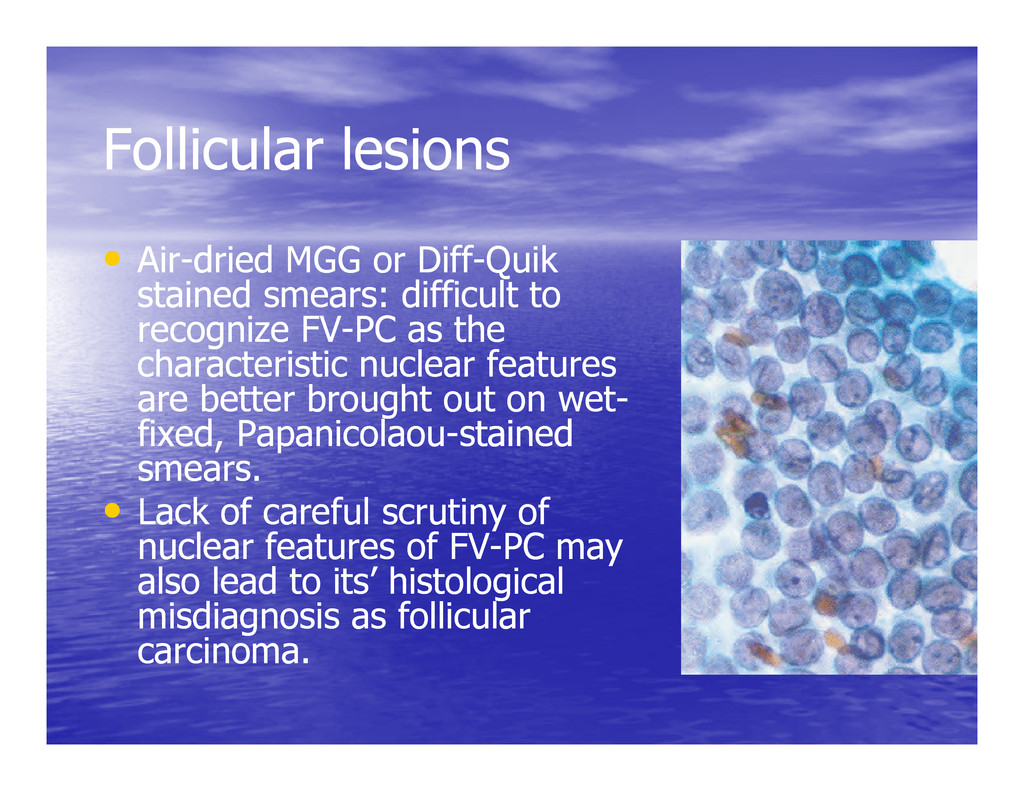
or Diff dried MGG or Diff- -Quik Quik stained smears: difficult to stained smears: difficult to recognize FV recognize FV- -PC as the PC as the characteristic nuclear features characteristic nuclear features are better brought out on wet are better brought out on wet- - are better brought out on wet are better brought out on wet- - fixed, Papanicolaou fixed, Papanicolaou- -stained stained smears. smears. • • Lack of careful scrutiny of Lack of careful scrutiny of nuclear features of FV nuclear features of FV- -PC may PC may also lead to its’ histological also lead to its’ histological misdiagnosis as follicular misdiagnosis as follicular carcinoma. carcinoma.
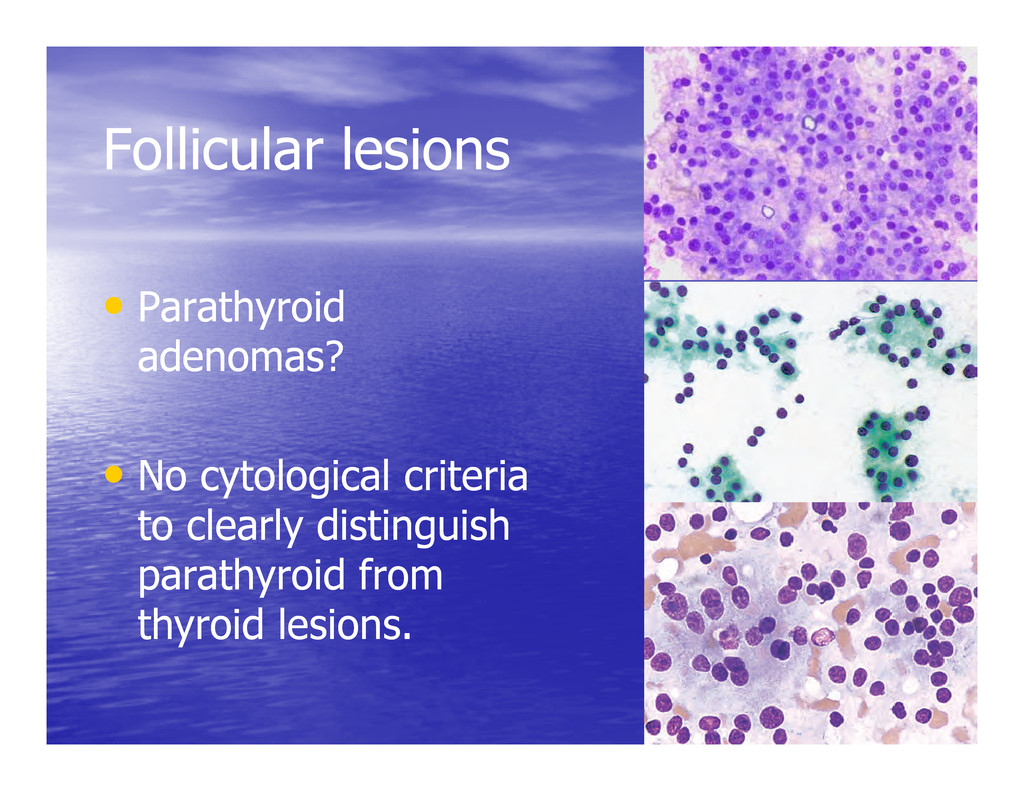
• • No cytological criteria No cytological criteria to clearly distinguish to clearly distinguish parathyroid from parathyroid from thyroid lesions. thyroid lesions.
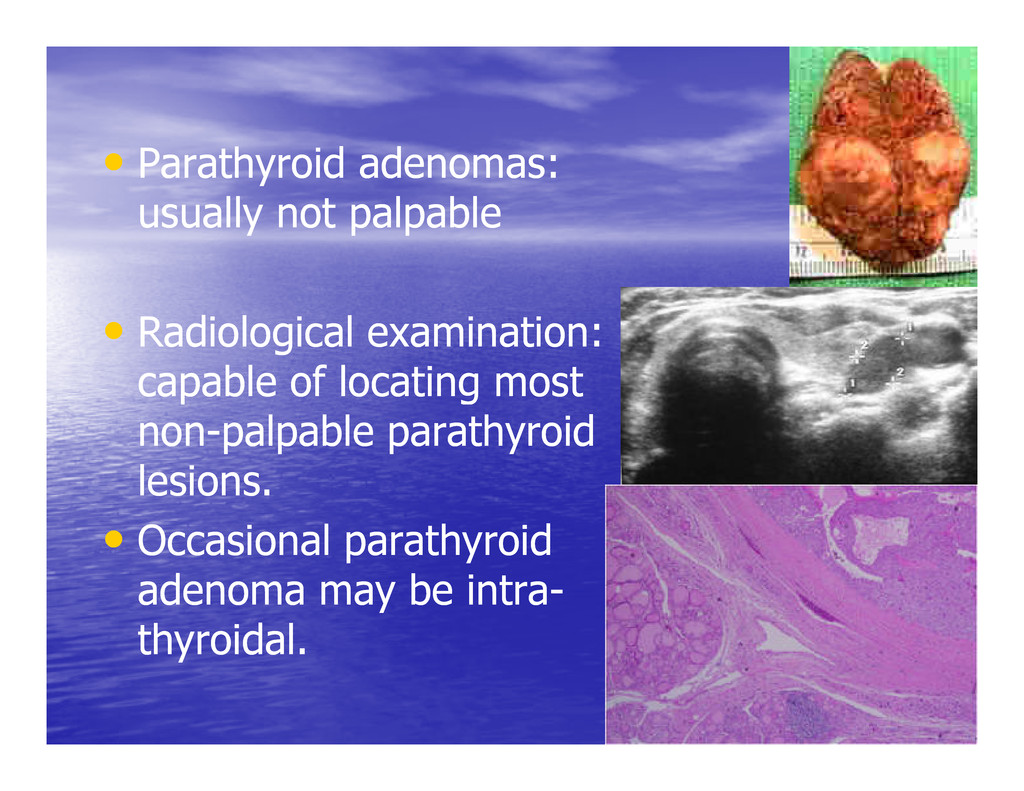
not palpable • • Radiological examination: Radiological examination: capable of locating most capable of locating most capable of locating most capable of locating most non non- -palpable parathyroid palpable parathyroid lesions. lesions. • • Occasional parathyroid Occasional parathyroid adenoma may be intra adenoma may be intra- - thyroidal. thyroidal.
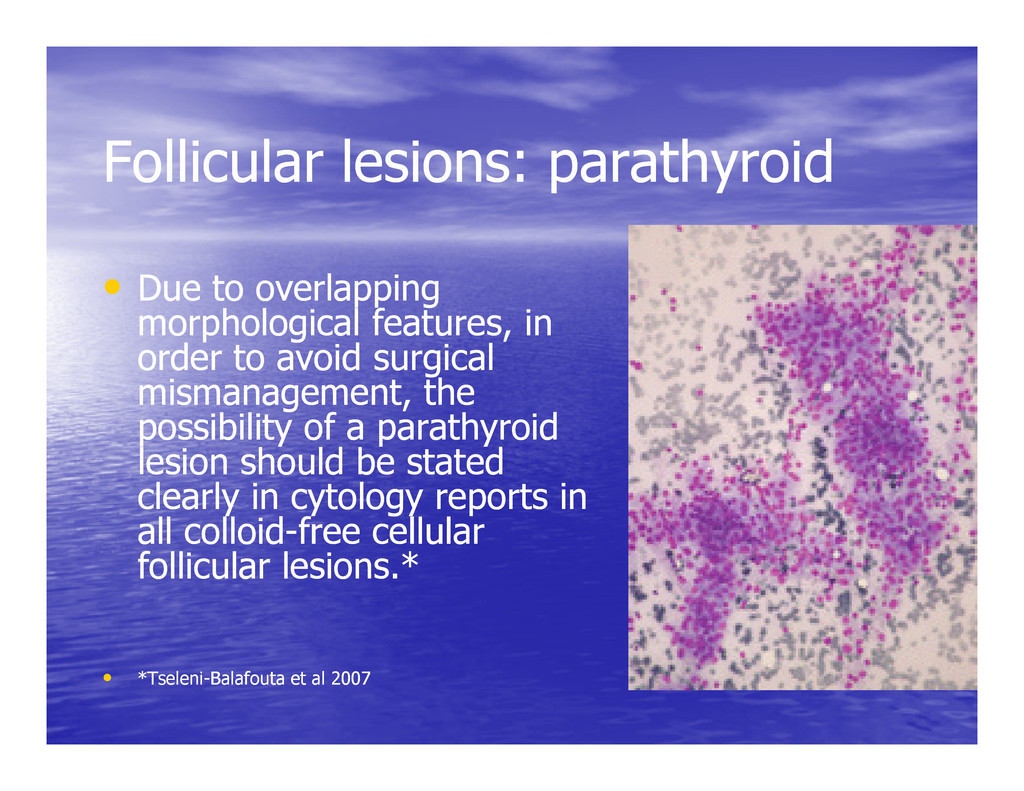
overlapping Due to overlapping morphological features, in morphological features, in order to avoid surgical order to avoid surgical mismanagement, the mismanagement, the mismanagement, the mismanagement, the possibility of a parathyroid possibility of a parathyroid lesion should be stated lesion should be stated clearly in cytology reports in clearly in cytology reports in all colloid all colloid- -free cellular free cellular follicular lesions.* follicular lesions.* • • *Tseleni *Tseleni- -Balafouta et al 2007 Balafouta et al 2007
FNA in thyroid? thyroid? To rule out malignancy so that To rule out malignancy so that unnecessary surgery can be unnecessary surgery can be avoided avoided
to select cellular follicular lesions for follow lesions for follow- -up or surgical excision up or surgical excision • • Leave a diagnosis of malignancy to Leave a diagnosis of malignancy to histological assessment of capsular and histological assessment of capsular and vascular invasion. vascular invasion.
any cytological atypia or suspicion of malignancy, it can be stated in the report malignancy, it can be stated in the report • • Helps in deciding whether to do Helps in deciding whether to do immediate surgery or follow immediate surgery or follow- -up the patient up the patient
thyroid FNA specimens should follow a standard format that is clinically follow a standard format that is clinically relevant in order to direct management. relevant in order to direct management. • • Clinical practice guidelines or recommendations Clinical practice guidelines or recommendations for thyroid FNA: developed by the Papanicolaou for thyroid FNA: developed by the Papanicolaou Society, the American Thyroid Association, the Society, the American Thyroid Association, the American Association of clinical endocrinologists, American Association of clinical endocrinologists, the Italian Association for Medical Endocrinology the Italian Association for Medical Endocrinology etc. etc.
with it the risk of malignancy risk of malignancy • •Each category is further qualified Each category is further qualified as to the possible pathological as to the possible pathological entity. entity.
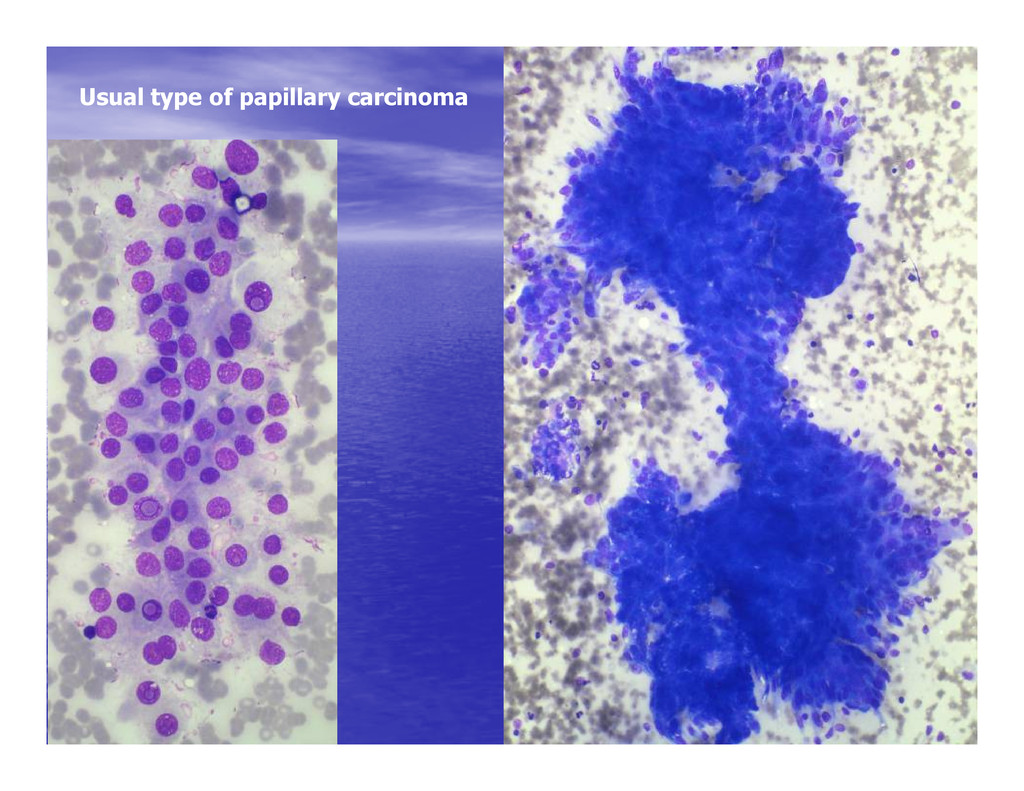
ca, Suspicious for papillary ca, Suspicious for papillary ca, Suspicious for papillary ca, medullary ca, anaplastic ca, medullary ca, anaplastic ca, metastatic malignancies metastatic malignancies
reporting thyroid FNA* reporting thyroid FNA* • • Simple and easily reproducible Simple and easily reproducible • • Following six categories useful in triaging patients for Following six categories useful in triaging patients for either clinical follow either clinical follow- -up or surgery: up or surgery: • • Unsatisfactory Unsatisfactory • • Unsatisfactory Unsatisfactory • • Benign Benign • • Atypical cellular lesion Atypical cellular lesion • • Follicular neoplasm Follicular neoplasm • • Suspicious for malignancy Suspicious for malignancy • • Positive for malignancy Positive for malignancy – – further qualify further qualify * Yang et al, Cancer 2007
is being made due If an indeterminate diagnosis is being made due to features suspicious but not diagnostic of a to features suspicious but not diagnostic of a neoplasm, it should be so qualified, since repeat neoplasm, it should be so qualified, since repeat FNA may enable definitive diagnosis. FNA may enable definitive diagnosis. FNA may enable definitive diagnosis. FNA may enable definitive diagnosis. • • If an indeterminate diagnosis is being made for If an indeterminate diagnosis is being made for a follicular neoplasm, qualifying it as such will a follicular neoplasm, qualifying it as such will clarify that distinction of benign from malignant clarify that distinction of benign from malignant cannot be achieved by repeat FNA, and either cannot be achieved by repeat FNA, and either ancillary techniques or histological study are ancillary techniques or histological study are required. required.
issue, in the former, a diagnosis of former, a diagnosis of “indeterminate “indeterminate (suspicious)” (suspicious)” can be given and in the latter can be given and in the latter can be given and in the latter can be given and in the latter a diagnosis of “indeterminate a diagnosis of “indeterminate (follicular neoplasm)” (follicular neoplasm)”
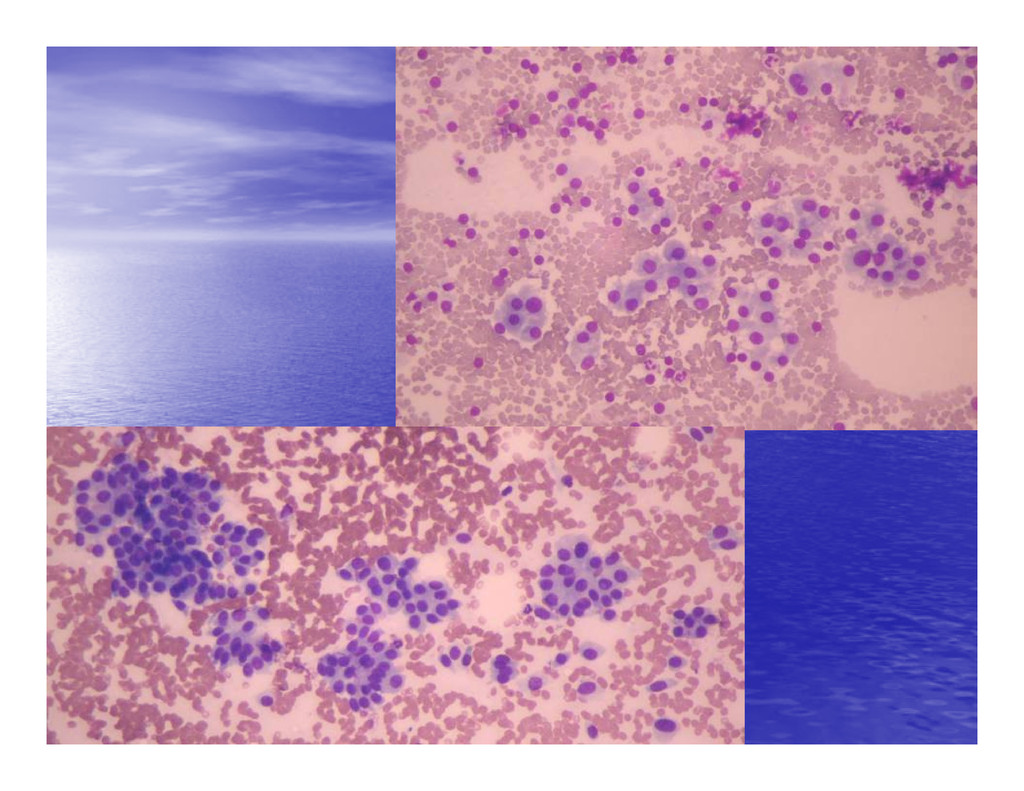
• • Swelling neck: 4 years Swelling neck: 4 years Case 1 Case 1 • • Swelling neck: 4 years Swelling neck: 4 years • • On examination: 8 cm sized nodule in the On examination: 8 cm sized nodule in the right lobe right lobe
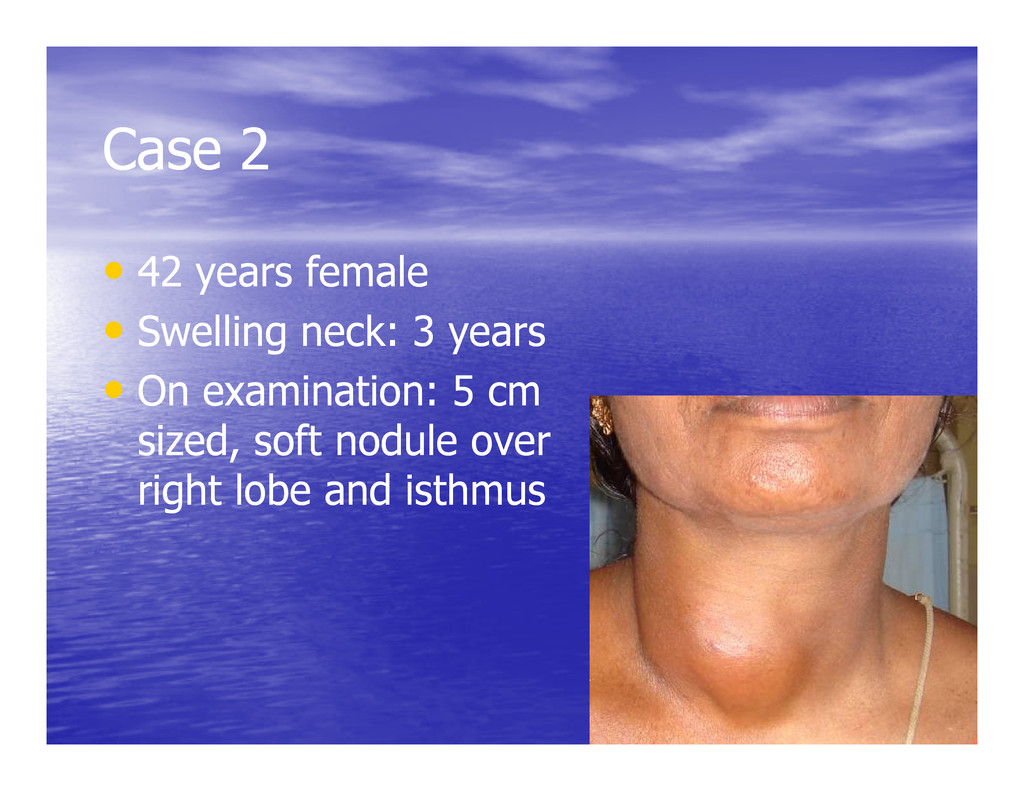
years female • • Swelling neck: 3 years Swelling neck: 3 years • • On examination: 5 cm On examination: 5 cm • • On examination: 5 cm On examination: 5 cm sized, soft nodule over sized, soft nodule over right lobe and isthmus right lobe and isthmus
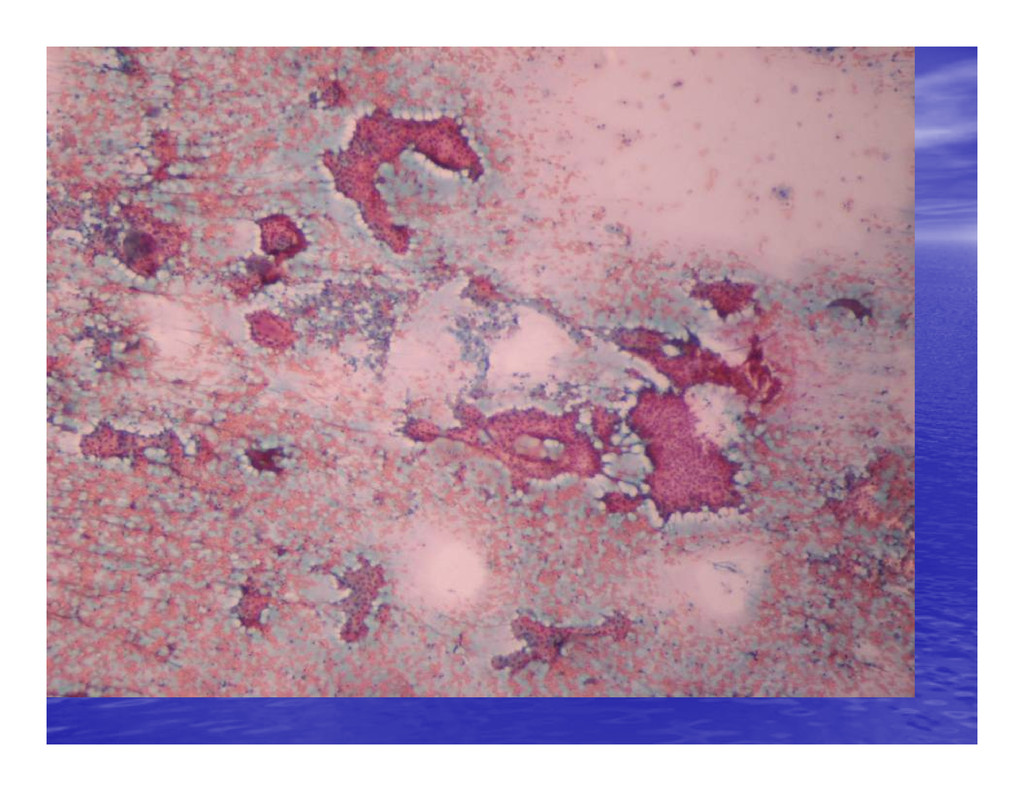
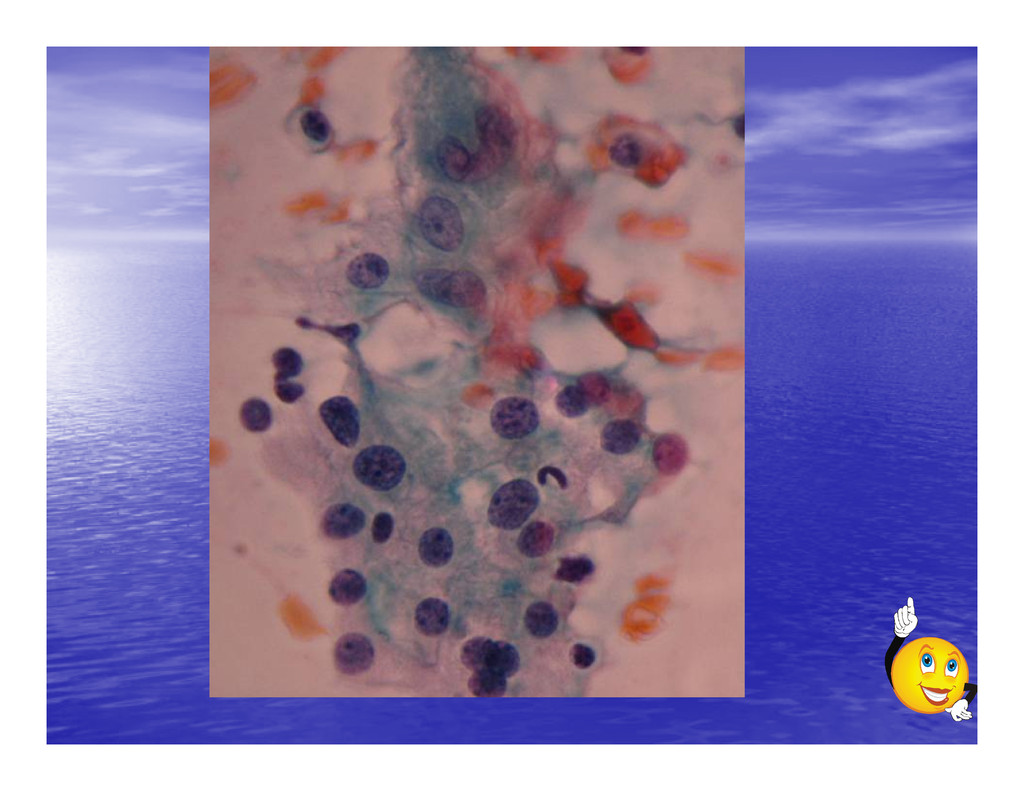
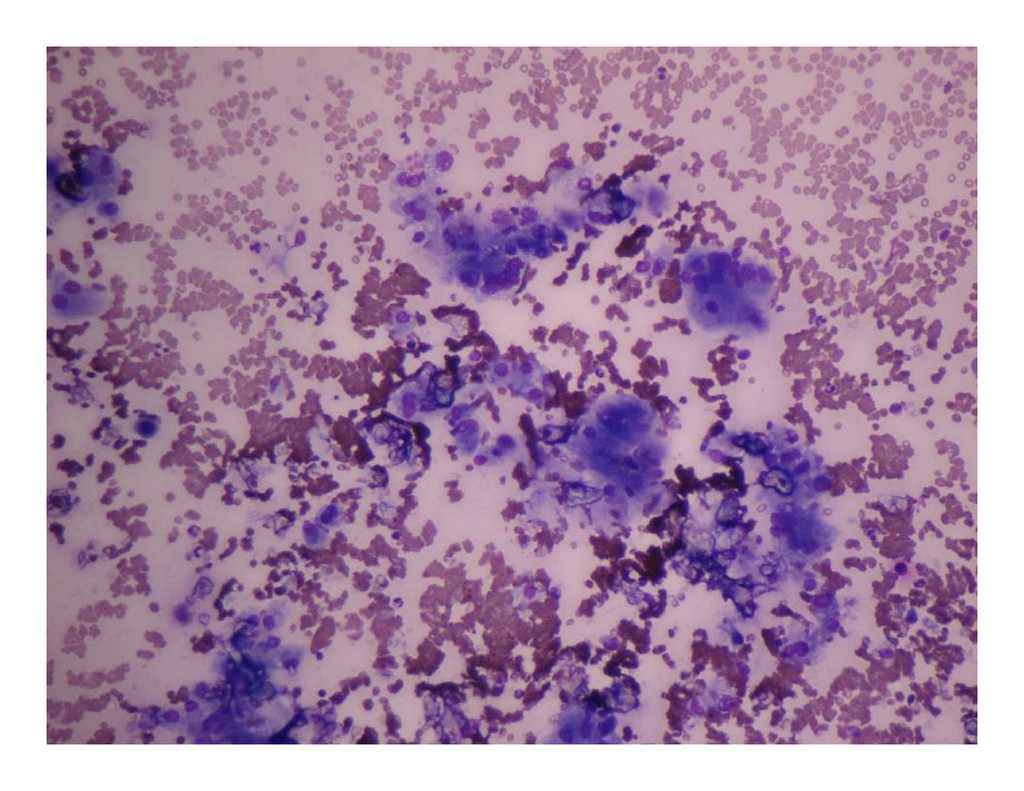
years female • • Neck swelling Neck swelling – – 15 days 15 days • • Neck swelling Neck swelling – – 15 days 15 days • • 3 cm right lobe nodule 3 cm right lobe nodule
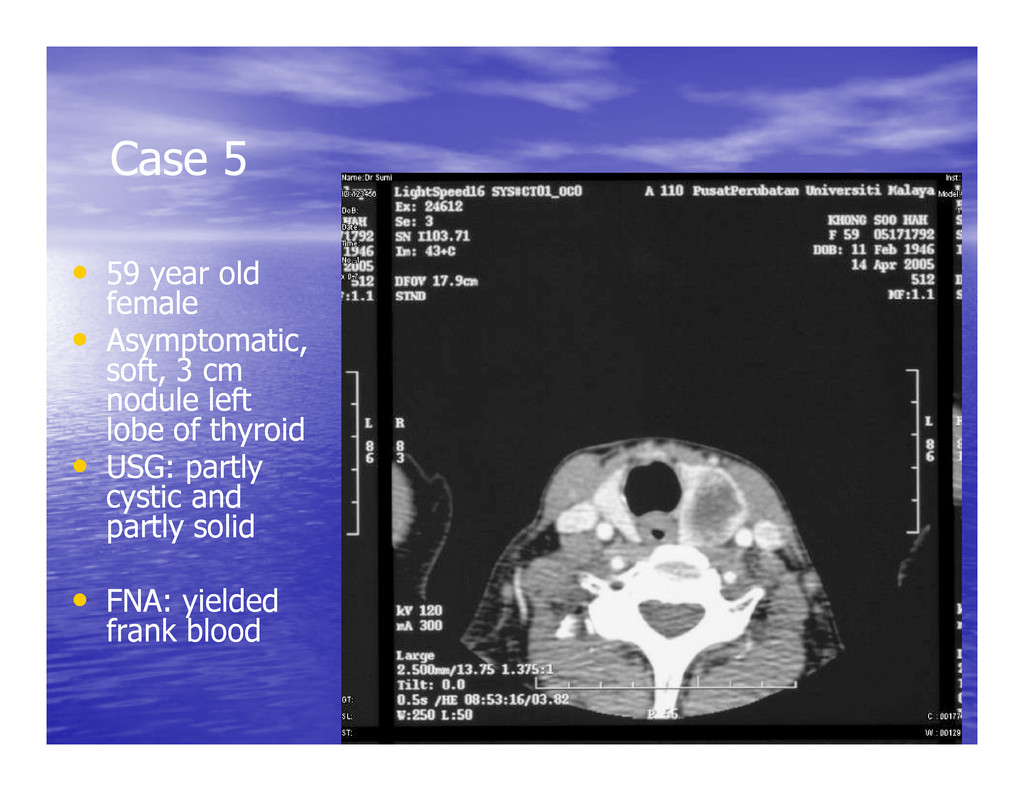
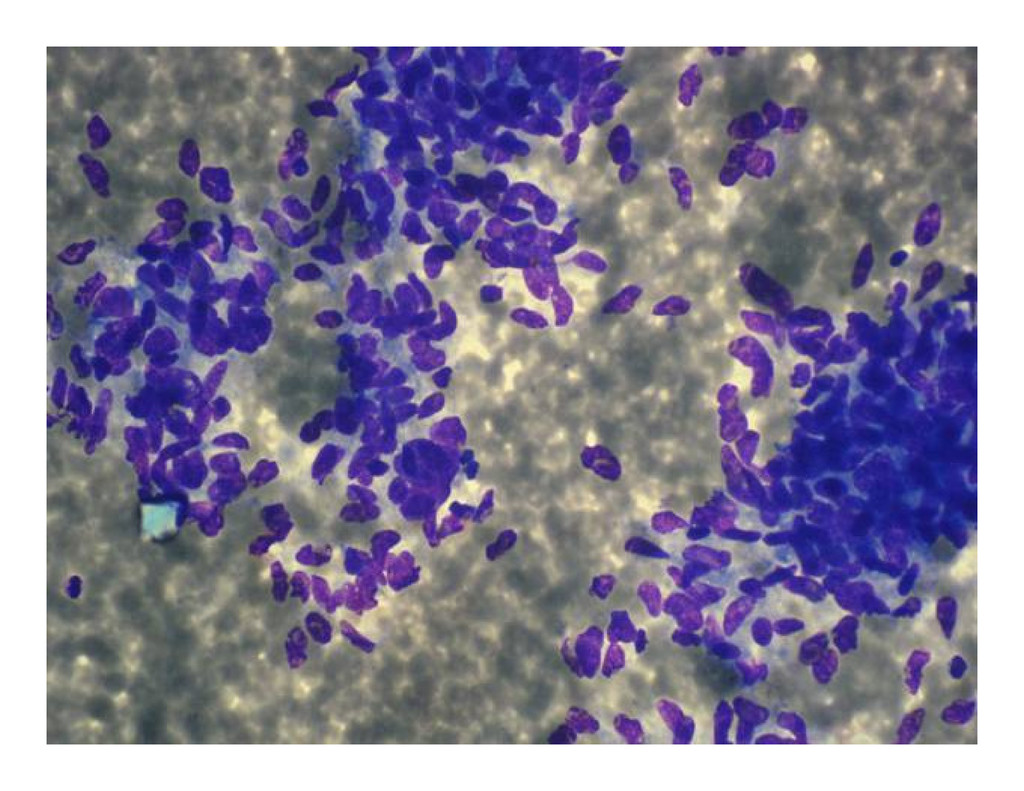
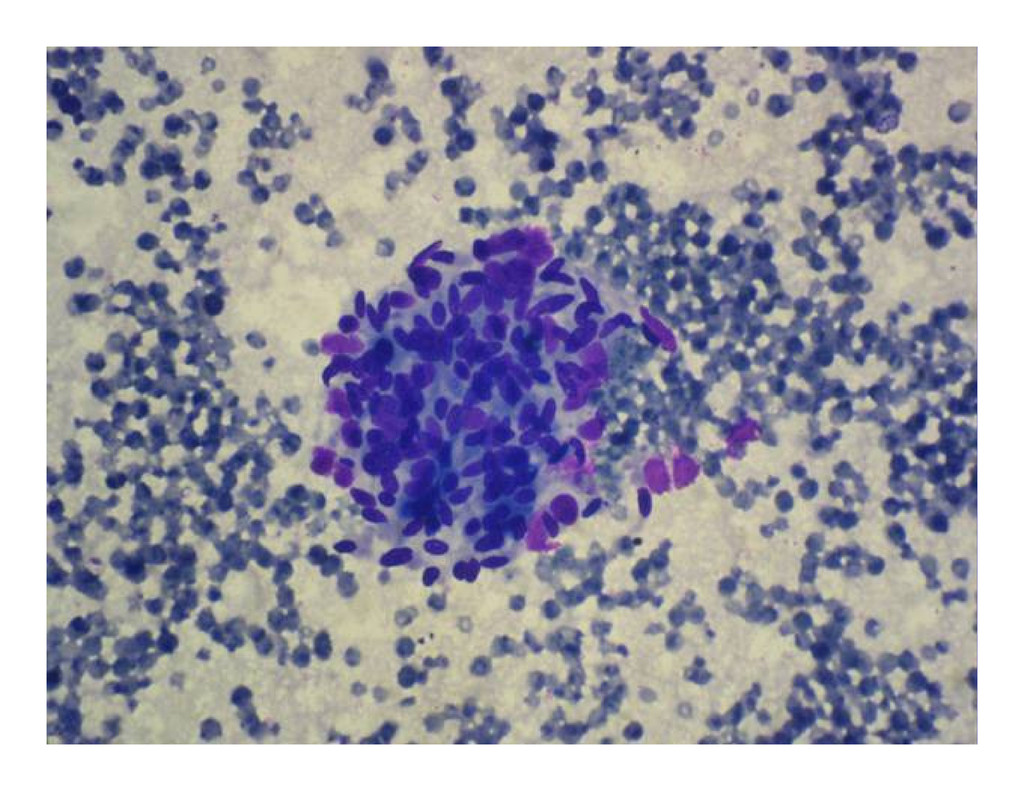
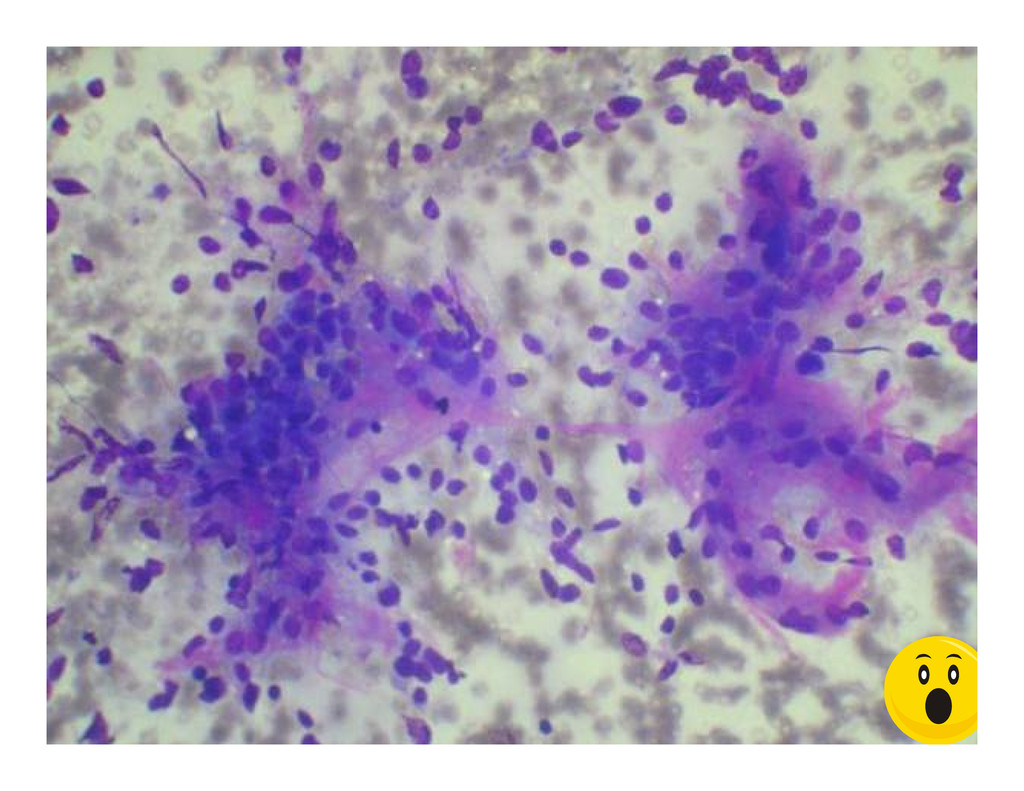
• • Asymptomatic, Asymptomatic, soft, 3 cm soft, 3 cm nodule left nodule left Case 5 nodule left nodule left lobe of thyroid lobe of thyroid • • USG: partly USG: partly cystic and cystic and partly solid partly solid • • FNA: yielded FNA: yielded frank blood frank blood
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}