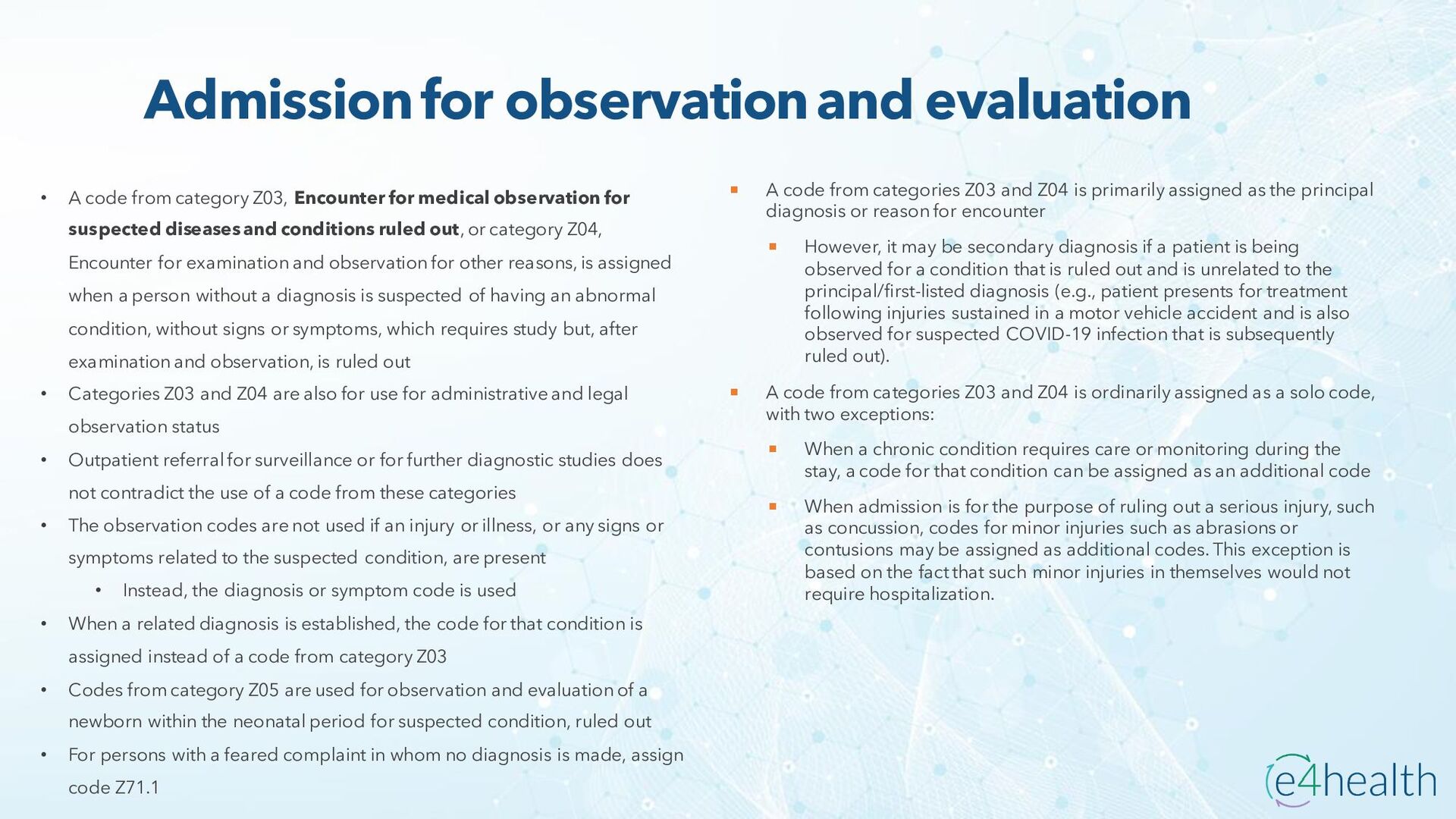
Z03, Encounter for medical observation for suspected diseases and conditions ruled out, or category Z04, Encounter for examination and observation for other reasons, is assigned when a person without a diagnosis is suspected of having an abnormal condition, without signs or symptoms, which requires study but, after examination and observation, is ruled out • Categories Z03 and Z04 are also for use for administrative and legal observation status • Outpatient referral for surveillance or for further diagnostic studies does not contradict the use of a code from these categories • The observation codes are not used if an injury or illness, or any signs or symptoms related to the suspected condition, are present • Instead, the diagnosis or symptom code is used • When a related diagnosis is established, the code for that condition is assigned instead of a code from category Z03 • Codes from category Z05 are used for observation and evaluation of a newborn within the neonatal period for suspected condition, ruled out • For persons with a feared complaint in whom no diagnosis is made, assign code Z71.1 A code from categories Z03 and Z04 is primarily assigned as the principal diagnosis or reason for encounter However, it may be secondary diagnosis if a patient is being observed for a condition that is ruled out and is unrelated to the principal/first-listed diagnosis (e.g., patient presents for treatment following injuries sustained in a motor vehicle accident and is also observed for suspected COVID-19 infection that is subsequently ruled out). A code from categories Z03 and Z04 is ordinarily assigned as a solo code, with two exceptions: When a chronic condition requires care or monitoring during the stay, a code for that condition can be assigned as an additional code When admission is for the purpose of ruling out a serious injury, such as concussion, codes for minor injuries such as abrasions or contusions may be assigned as additional codes. This exception is based on the fact that such minor injuries in themselves would not require hospitalization.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}