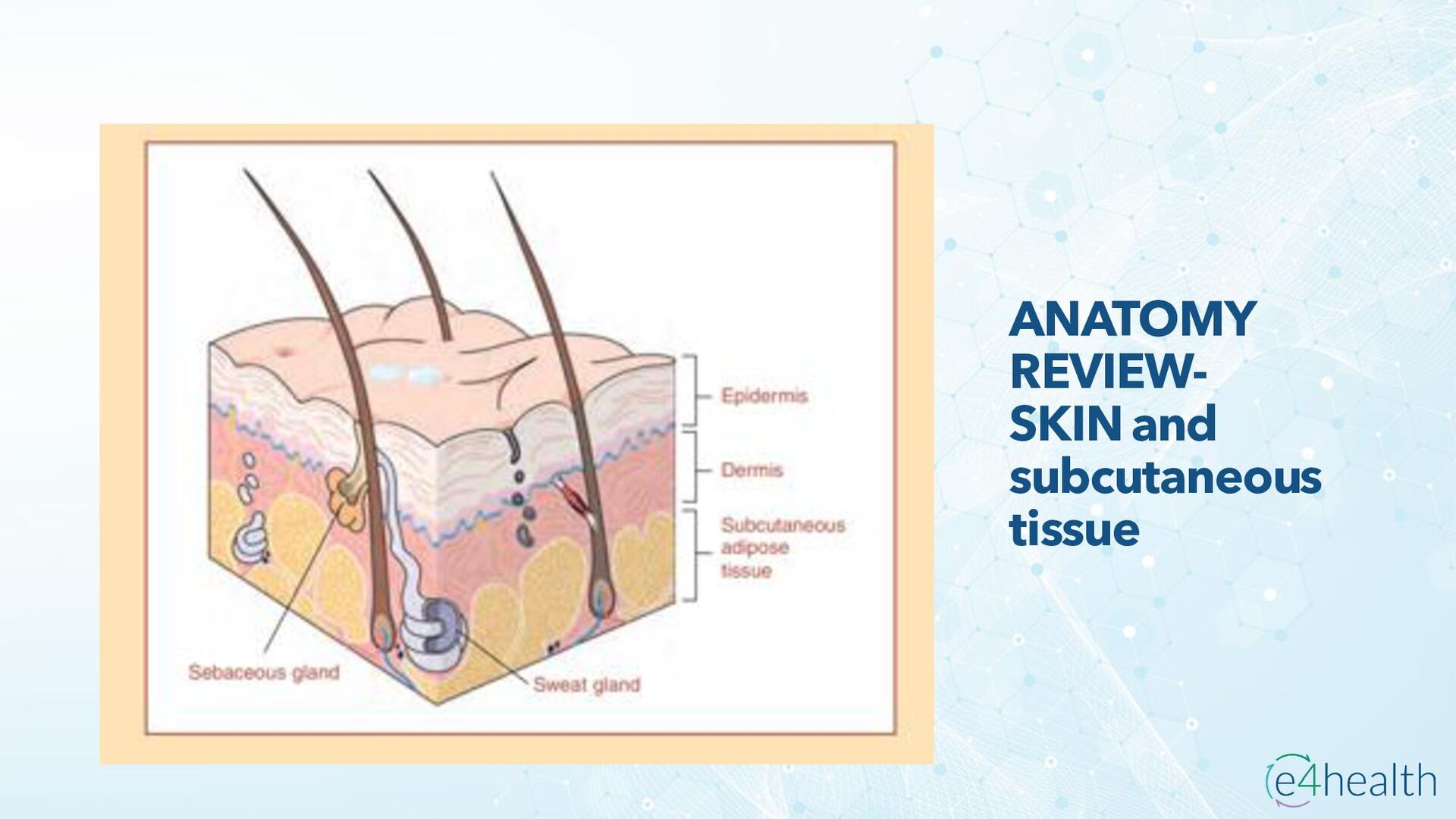
required to appropriately classify cutaneous abscess, furuncle, carbuncle, cellulitis and acute lymphangitis. • Cellulitis: A non-necrotizing infection of the skin involving the deeper layer of the dermis and the subcutaneous fat but does not involve the fascia or muscle. It typically occurs as a result of the entry of bacteria through a breach in the skin barrier due to trauma (abrasion, laceration, insect bit, puncture wound), inflammation (eczema, radiation), pre-existing skin infections, and edema (lymphatic obstruction, venous insufficiency). However, a break in the skin may be so small as to be undetectable. The characteristic signs and symptoms of cellulitis include: • Localized pain, Swelling, Tenderness, Erythema, Warmth, Purulent drainage, Lymphangitis or regional adenopathy The most common bacteria associated with cellulitis are beta-hemolytic streptococci (groups A, B, C, G, and F) and S. aureus (including methicillin-resistant type) Treatment for cellulitis includes elevation of the affected body part, treatment of underlying conditions leading to cellulitis, and antibiotics. Inpatient admission for intravenous antibiotics therapy may be required.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}