software engineering and multi- discipline complex IT implementations (Gov., defense, health, finance, insurance) • 12+ years of healthcare IT and medical devices experience (blog at http://healthcareguy.com) • 15+ years of technology management experience (government, non-profit, commercial) • 10+ years as architect, engineer, and implementation manager on various EMR and EHR initiatives (commercial and non- profit) Author of Chapter 13, “You’re the CIO of your Own Office”
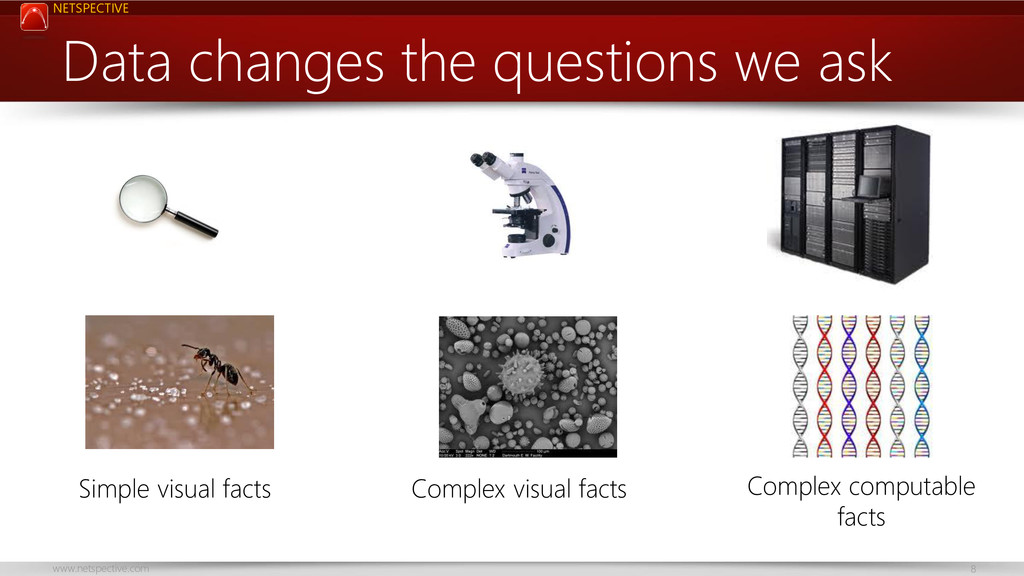
deluge of healthcare data is being created as we digitize biology, chemistry, and physics. • Data changes the questions we ask and it can actually democratize and improve the science of medicine, if we let it. • While cures are the only real miracles of medicine, data can help solve intractable problems and lead to more cures. • Healthcare-focused software engineering is going to do more harm than good (industry-neutral is better). Key takeaways • EHRs are not the center of the healthcare data ecosystem. • Applications come and go, data lives forever. He who owns, integrates, and uses data wins in the end. • Never leave your data in the hands of an application/system vendor. • There’s nothing special about health IT data that justifies complex, expensive, or special technology. • Spend freely on multiple systems and integration-friendly solutions.
of response to new patient/HCP needs Reduce permission- oriented culture React faster to regulatory and market changes Reduce number of Shadow IT systems Reduce compliance-focus in favor of customer focus
a widely accepted myth that medicine requires complex, highly specialized information-technology (IT) systems. This myth continues to justify soaring IT costs, burdensome physician workloads, and stagnation in innovation — while doctors become increasingly bound to documentation and communication products that are functionally decades behind those they use in their “civilian” life. New England Journal of Medicine “Escaping the EHR Trap - The Future of Health IT”, June 2012
Allocating scarce resources in real-time to reduce heart failure readmissions: a prospective, controlled study http://qualitysafety.bmj.com/content/early/2013/07/31/bmjqs-2013-001901.full “This study provides preliminary evidence that technology platforms that allow for automated EMR data extraction, case identification and risk stratification may help potentiate the effect of known readmission reduction strategies, in particular those that emphasize intensive and early post-discharge outpatient contact.”
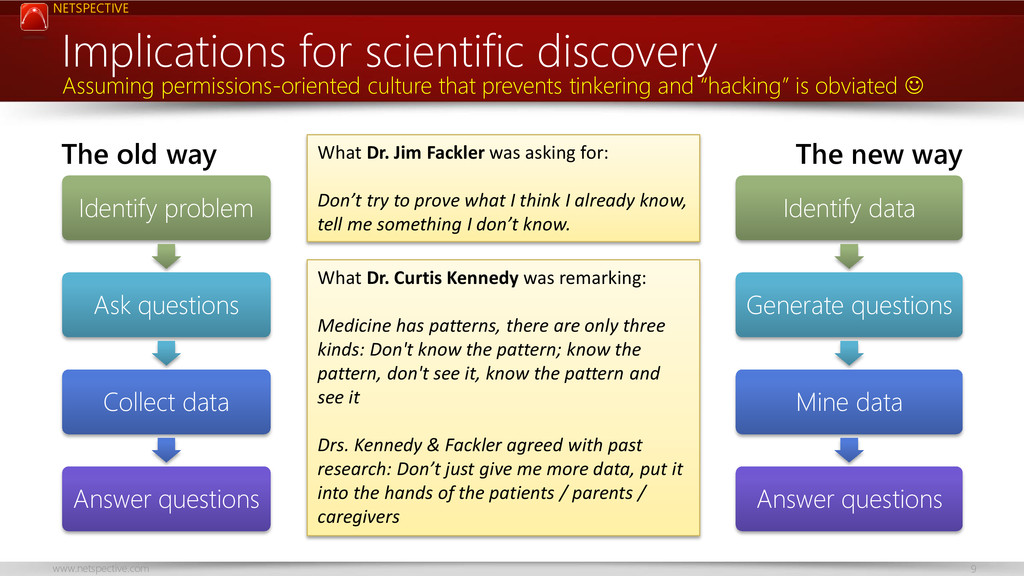
Don’t try to prove what I think I already know, tell me something I don’t know. The old way Identify problem Ask questions Collect data Answer questions The new way Identify data Generate questions Mine data Answer questions Implications for scientific discovery Assuming permissions-oriented culture that prevents tinkering and “hacking” is obviated What Dr. Curtis Kennedy was remarking: Medicine has patterns, there are only three kinds: Don't know the pattern; know the pattern, don't see it, know the pattern and see it Drs. Kennedy & Fackler agreed with past research: Don’t just give me more data, put it into the hands of the patients / parents / caregivers
instead of Data-focused IT is causing business problems. Healthcare Provider Systems Clinical Apps Patient Apps Billing Apps Lab Apps Other Apps Partner Systems Silos of information exist across groups (duplication, little sharing) Poor data integration across application bases
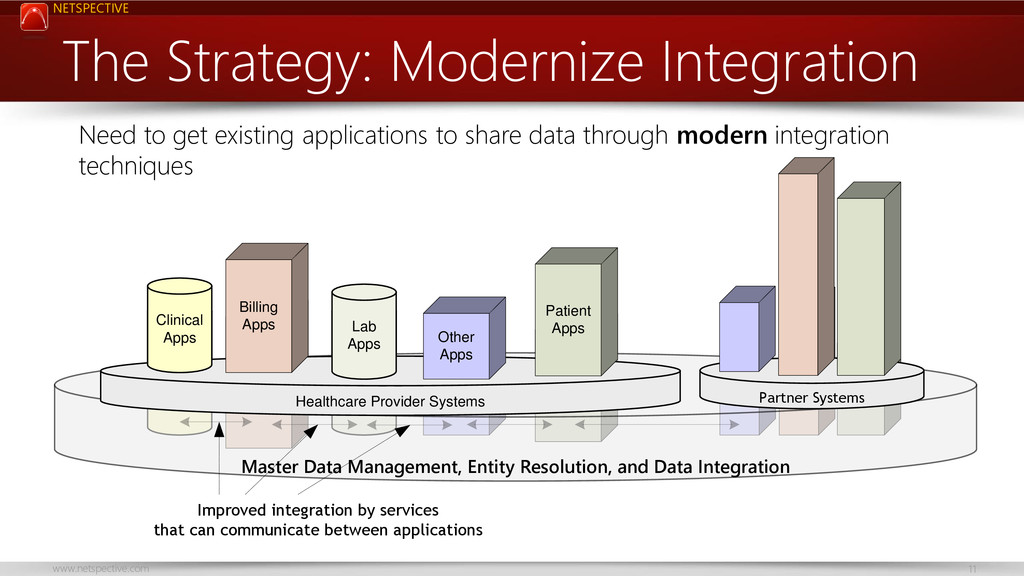
Provider Systems Clinical Apps Patient Apps Billing Apps Lab Apps Other Apps Master Data Management, Entity Resolution, and Data Integration Partner Systems Improved integration by services that can communicate between applications The Strategy: Modernize Integration Need to get existing applications to share data through modern integration techniques
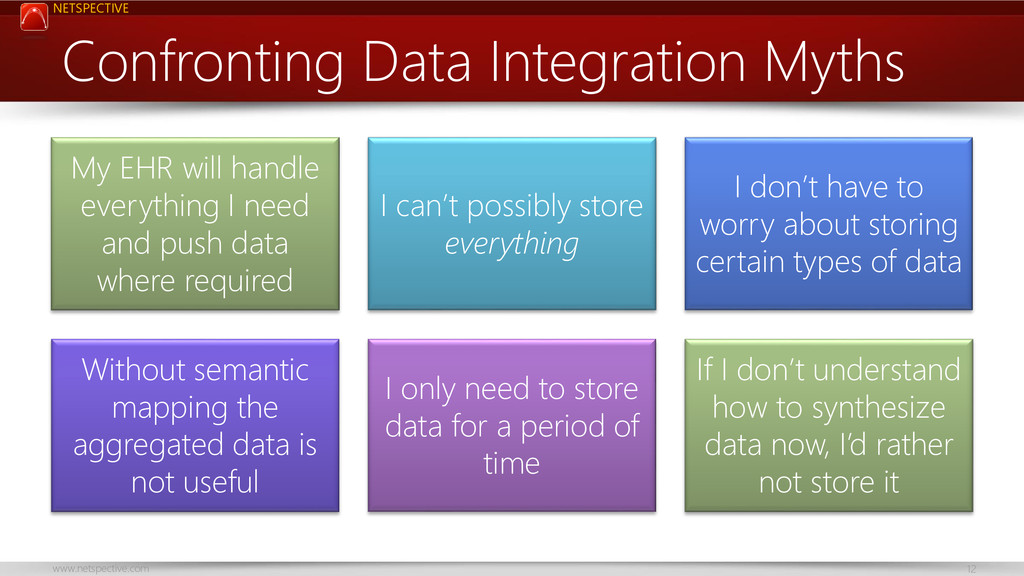
handle everything I need and push data where required I can’t possibly store everything I don’t have to worry about storing certain types of data Without semantic mapping the aggregated data is not useful I only need to store data for a period of time If I don’t understand how to synthesize data now, I’d rather not store it
Permissions-oriented culture prevents tinkering and “hacking” • We don't support shared identities, single sign on (SSO), and industry- neutral authentication and authorization • We’re looking for "structured data integration" instead of "practical app integration" in our early project phases • We create large monolithic data warehouses instead of small service oriented databases • We “push" data everywhere instead of "pulling" it when necessary • We assume EHRs the center of the universe • We accept and reward vendors that don’t care about integration • We have “Inside out” architecture, not “Outside in” • We're too focused on heavyweight industry-specific formats instead of lightweight or micro formats • Data emitted is not tagged using semantic markup, so it's not securable or searchable by default
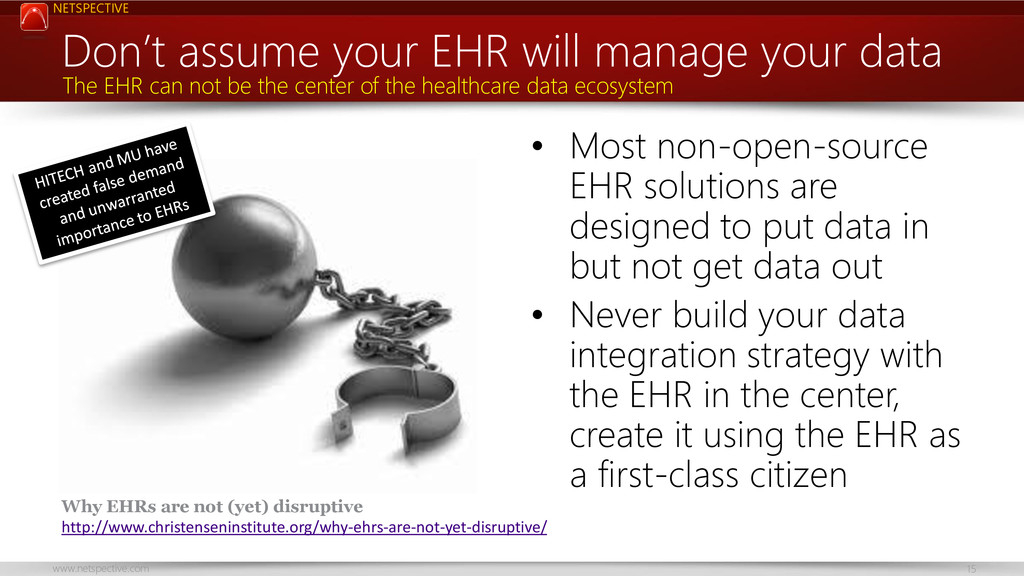
to put data in but not get data out • Never build your data integration strategy with the EHR in the center, create it using the EHR as a first-class citizen Don’t assume your EHR will manage your data The EHR can not be the center of the healthcare data ecosystem Why EHRs are not (yet) disruptive http://www.christenseninstitute.org/why-ehrs-are-not-yet-disruptive/
they’re problem solvers • Today’s permissions- oriented culture now prevents “playing” with data and discovering solutions Encourage clinical “tinkering” and “hacking” It’s ok to not know the answer in advance
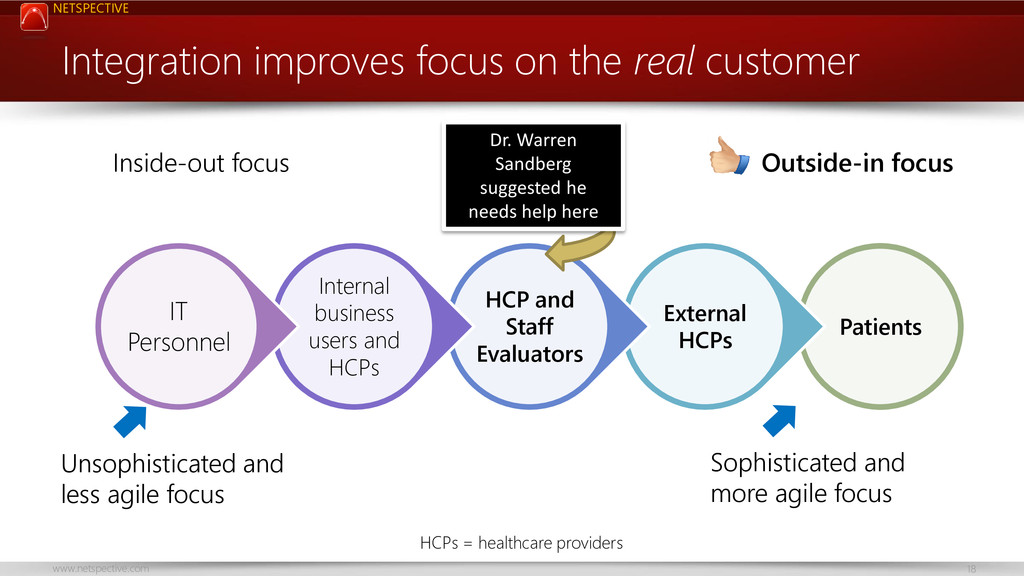
Internal business users and HCPs IT Personnel Integration improves focus on the real customer Unsophisticated and less agile focus Sophisticated and more agile focus Inside-out focus Outside-in focus HCPs = healthcare providers Dr. Warren Sandberg suggested he needs help here
health IT systems create their own custom identity, credentialing, and access management (ICAM) in an opaque part of a proprietary database. • We’re waiting for solutions from health IT vendors but free or commercial industry- neutral solutions are much better and future proof. Identity exchange is possible • Follow National Strategy for Trusted Identities in Cyberspace (NSTIC) • Use open identity exchange protocols such as SAML, OpenID, and Oauth • Use open roles and permissions-management protocols, such as XACML • Consider open source tools such as OpenAM, Apache Directory, OpenLDAP , Shibboleth, or commercial vendors. • Externalize attribute-based access control (ABAC) and role-based access control (RBAC) from clinical systems into enterprise systems like Active Directory or LDAP . Implement industry-neutral ICAM Implement shared identities, single sign on (SSO), neutral authentication and authorization
we shouldn’t integrate until structured data at detailed machine- computable levels is available. The thinking is that because mistakes can be made with semi-structured or hard to map data, we should rely on paper, make users live with missing data, or just make educated guesses instead. App-centric sharing is possible Instead of waiting for HL7 or other structured data about patients, we can use simple techniques like HTML widgets to share "snippets" of our apps. • Allow applications immediate access to portions of data they don't already manage. • Widgets are portions of apps that can be embedded or "mashed up" in other apps without tight coupling. • Blue Button has demonstrated the power of app integration versus structured data integration. It provides immediate benefit to users while the data geeks figure out what they need for analytics, computations, etc. • Consider Direct for app-centric connectivity. App-focused integration is better than nothing Structured data dogma gets in the way of faster decision support real solutions
you send me?” (push) The "push" model, where the system that contains the data is responsible for sending the data to all those that are interested (or to some central provider, such as a health information exchange or HL7 router) shouldn’t be the only model used for data integration. Better way to architect: “What data can I publish safely?” (pull) • Implement FHIR or syndicated Atom-like feeds (which could contain HL7 or other formats). • Data holders should allow secure authenticated subscriptions to their data and not worry about direct coupling with other apps. • Consider the Open Data Protocol (oData). • Enable auditing of protected health information by logging data transfers through use of syslog and other reliable methods. • Enable proper access control rules expressed in standards like XACML. • Consider Direct for connectivity if you can’t get away from ‘push’. Pushing data is more expensive than pulling it We focus more on "pushing" versus "pulling" data than is warranted early in projects
warehouse The centralized clinical data warehouse (CDW) model, where a massive multi-year project creates a monolithic relational database that all analytics will run off was fine when retrospective reporting is what defined analytics. This old architecture won’t work in modern predictive analytics and mobile-centric requirements. Better way to architect: Service-oriented databases on RDBMS/NoSQL • Drive transactional ACID-based data requirements to RDBMS and consider column- stores, document-stores, and network-stores for other kinds of data • Break relationships between data and store lookup, transactional, predictive, scoring, risk strat, trial associated, retrospective, identity, mortality ratios, and other types of data based on their usage criteria not developer convenience • Use translucent encryption and auto-de- identification of data to make it more useful without further processing • Design for decentralized sync’ing of data (e.g. mobile, etc.) not centralized ETL Move to service-oriented (de-identifiable) data Don’t assume all your data has to go into a giant data warehouse
secure data structures An example of structuring data for analysis Preparing data is important http://www.ibm.com/developerworks/data/library/techarticle/dm-ind-ehr/
The general assumption is that formats like HL7, CCD, and X.12 are the only ways to do data integration in healthcare but of course that’s not quite true. Consider industry-neutral protocols • Consider identity exchange protocols like SAML for integration of user profile data and even for exchange of patient demographics and related profile information. • Consider iCalendar/ICS publishing and subscribing for schedule data. • Consider microformats like FOAF and similar formats from schema.org. • Consider semantic data formats like RDF, RDFa, and related family. Industry-specific formats aren’t always necessary Reliance on heavyweight industry-specific formats instead of lightweight micro formats is bad
existing contracts, the vendors of systems that house the data also ‘own’ the data and it can’t be easily liberated because the vendors of the systems actively prevent it from being shared or are just too busy to liberate the data. Semantic markup and tagging is easy • One easy way to create semantically meaningful and easier to share and secure patient data is to have all HTML tags be generated with companion RDFa or HTML5 Data Attributes using industry-neutral schemas and microformats similar to the ones defined at Schema.org. • Google's recent implementation of its Knowledge Graph is a great example of the utility of this semantic mapping approach. Tag all app data using semantic markup When data is not tagged using semantic markup, it's not securable or shareable by default
applications only present through text or windowed interfaces that can be “scraped”. • Web-based applications present HTML, JavaScript, images, and other assets but aren’t search engine friendly. Search engines are great integrators • Most users need access to information trapped in existing applications but sometimes they don’t need must more than access that a search engine could easily provide. • Assume that all pages in an application, especial web applications, will be “ingested” by a securable, protectable, search engine that can act as the first method of integration. Produce data in search-friendly manner Produce HTML, JavaScript and other data in a security- and integration-friendly approach
government spends more per user on antiquated software than we do in healthcare. • There is a general fear that open source means unsupported software or lower quality solutions or unwanted security breaches. Open source can save health IT • Other industries save billions by using open source. • Commercial vendors give better pricing, service, and support when they know they are competing with open source. • Open source is sometimes more secure, higher quality, and better supported than commercial equivalents. • Don’t dismiss open source, consider it the default choice and select commercial alternatives when they are known to be better. Rely first on open source, then proprietary “Free” is not as important as open source, you should pay for software but require openness
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Thank You Visit http://www.netspective.com http://www.healthcareguy.com E-mail [email protected] Follow @ShahidNShah Call](https://files.speakerdeck.com/presentations/f65a13e0e8e001304a13021448eaa125/slide_27.jpg){kind=link}