causes of syncope. Discuss the appropriate assessment of syncope. Define who is at risk. Discuss what tests might be appropriate. Very briefly look at 'treatment of syncope'. Evaluate what we've learned.
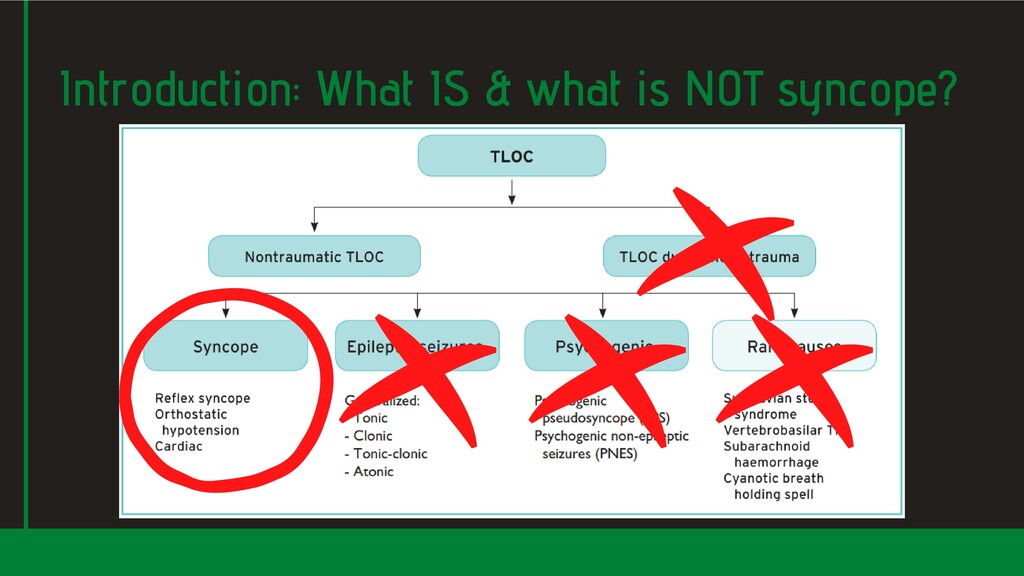
consciousness due to transient global cerebral hypo-perfusion, characterised by rapid onset, short duration and spontaneous and complete recovery." Syncope shares many clinical features with other disorders - it therefore results in many differential diagnoses. This wider group of disorders is labelled transient loss of consciousness (TLoC).
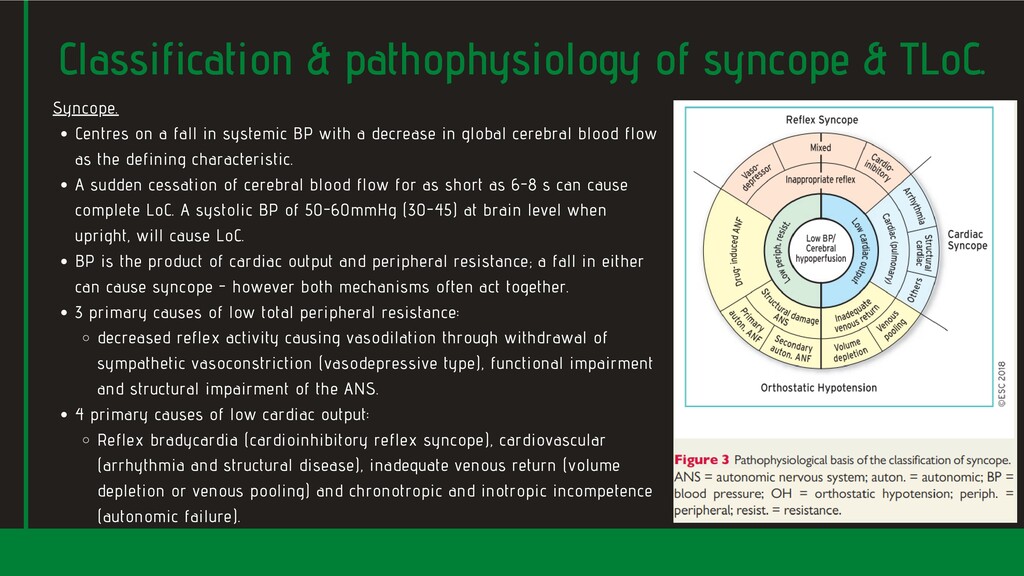
in global cerebral blood flow as the defining characteristic. A sudden cessation of cerebral blood flow for as short as 6-8 s can cause complete LoC. A systolic BP of 50-60mmHg (30-45) at brain level when upright, will cause LoC. BP is the product of cardiac output and peripheral resistance; a fall in either can cause syncope - however both mechanisms often act together. 3 primary causes of low total peripheral resistance: decreased reflex activity causing vasodilation through withdrawal of sympathetic vasoconstriction (vasodepressive type), functional impairment and structural impairment of the ANS. 4 primary causes of low cardiac output: Reflex bradycardia (cardioinhibitory reflex syncope), cardiovascular (arrhythmia and structural disease), inadequate venous return (volume depletion or venous pooling) and chronotropic and inotropic incompetence (autonomic failure). Syncope. Classification & pathophysiology of syncope & TLoC.
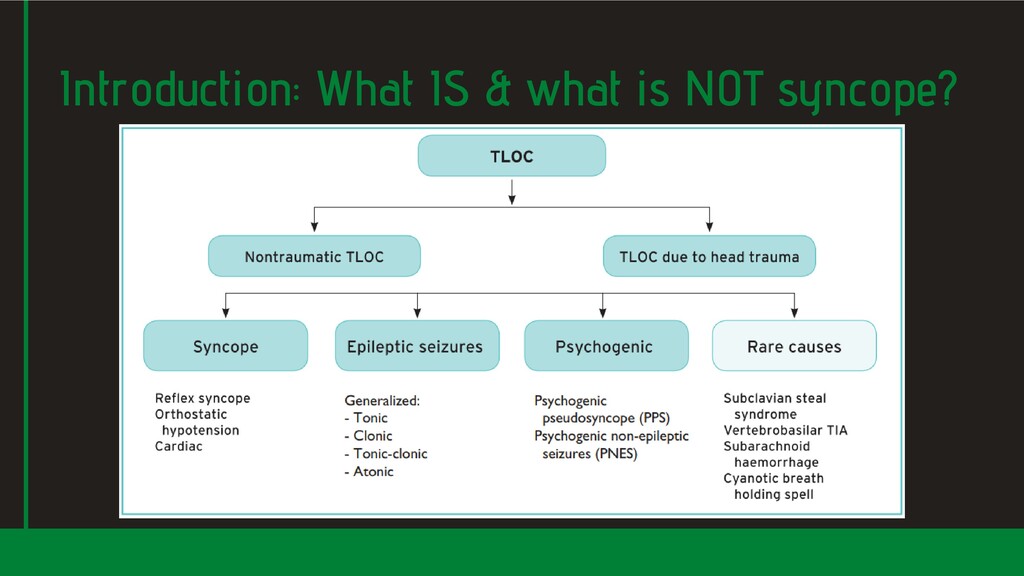
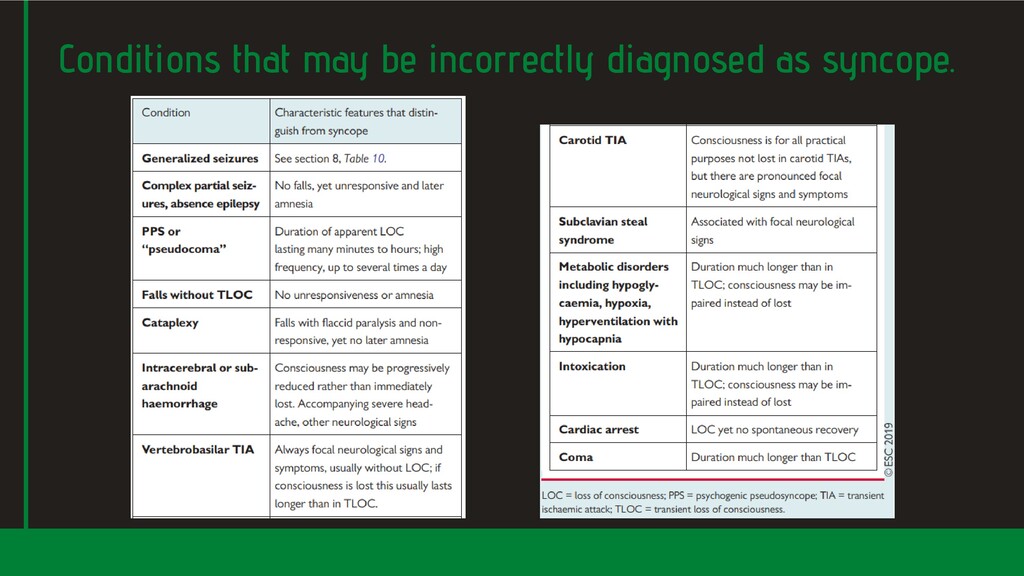
epilepsy in which normal motor control is lost, are included - tonic, clonic, tonic-clonic and atonic. Epilepsy where people remain upright (sitting or standing) eg complex parital seizures or absence epilepsy, are not counted as TLoC, but sometimes are incorrectly diagnosed as syncope. Psychogenic TLoC consists of 2 forms: One resembles epileptic seizures (psychogenic non-epileptic seizures (PNES). The other resembles syncope (psychogenic psuedosyncope (PPS). The rare forms of TLoC seldomly cause confusion with the main TLoC forms: Both vertebrobasilar TIAs and subclavian steel syndrome are associated with focal neurological signs. A SAH may present with a short TLoC but the associated extreme headache suggests the cause. In cyantoic breath-holding spells, expiratory apnoea with hyopoxia is the primary mechanism. Non-syncopal forms of (real or apparent) TLoC.
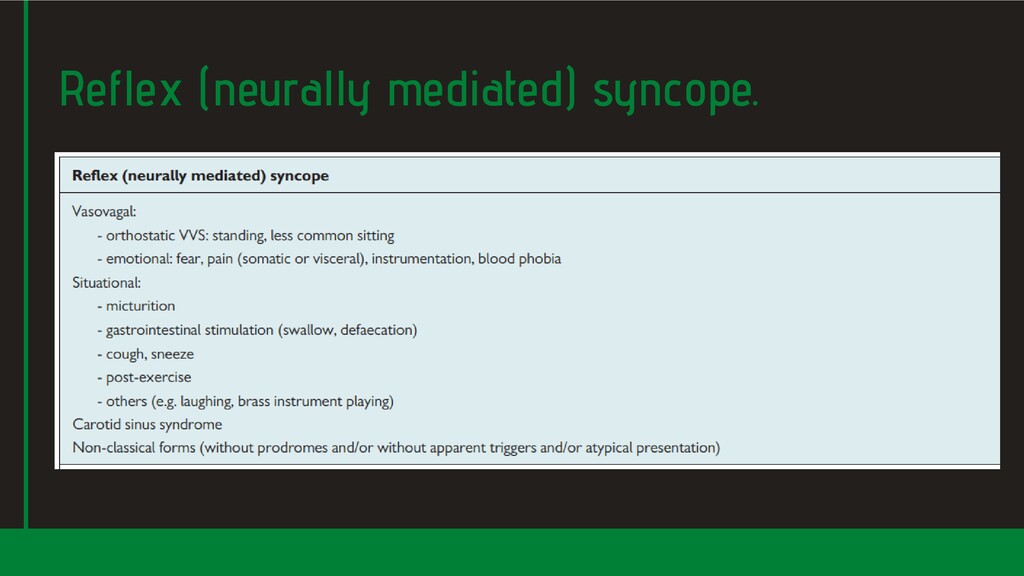
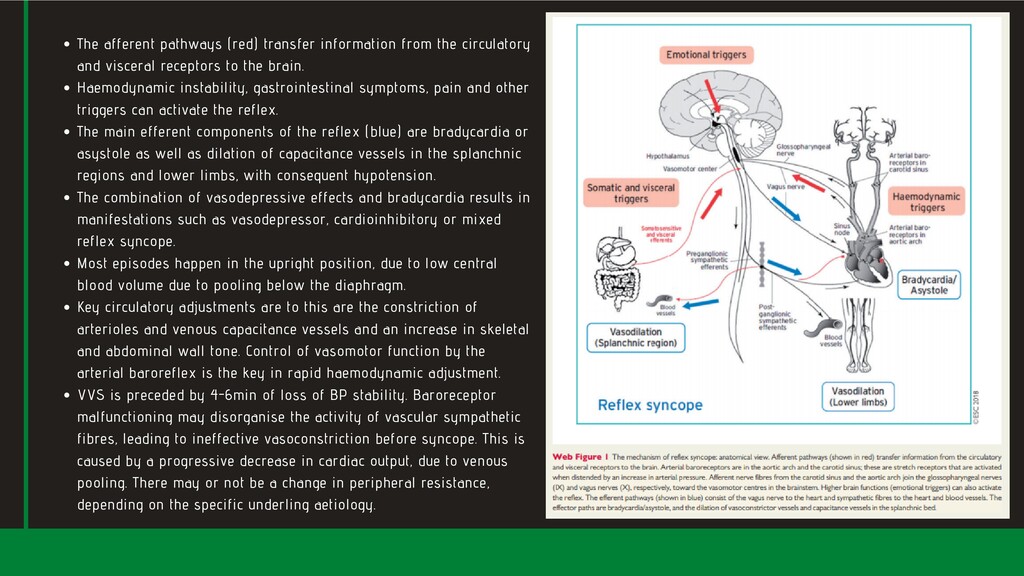
visceral receptors to the brain. Haemodynamic instability, gastrointestinal symptoms, pain and other triggers can activate the reflex. The main efferent components of the reflex (blue) are bradycardia or asystole as well as dilation of capacitance vessels in the splanchnic regions and lower limbs, with consequent hypotension. The combination of vasodepressive effects and bradycardia results in manifestations such as vasodepressor, cardioinhibitory or mixed reflex syncope. Most episodes happen in the upright position, due to low central blood volume due to pooling below the diaphragm. Key circulatory adjustments are to this are the constriction of arterioles and venous capacitance vessels and an increase in skeletal and abdominal wall tone. Control of vasomotor function by the arterial baroreflex is the key in rapid haemodynamic adjustment. VVS is preceded by 4-6min of loss of BP stability. Baroreceptor malfunctioning may disorganise the activity of vascular sympathetic fibres, leading to ineffective vasoconstriction before syncope. This is caused by a progressive decrease in cardiac output, due to venous pooling. There may or not be a change in peripheral resistance, depending on the specific underling aetiology.
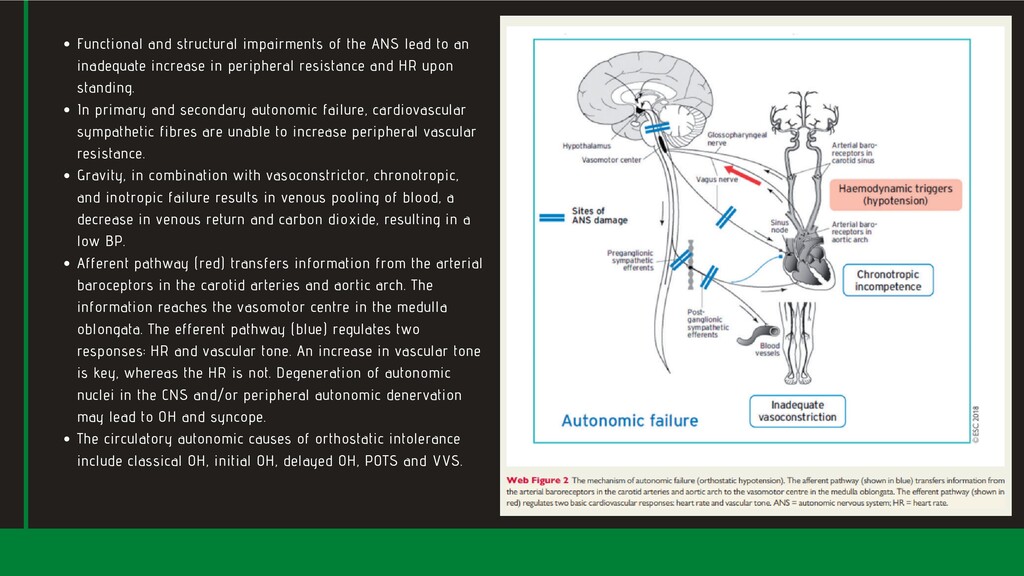
inadequate increase in peripheral resistance and HR upon standing. In primary and secondary autonomic failure, cardiovascular sympathetic fibres are unable to increase peripheral vascular resistance. Gravity, in combination with vasoconstrictor, chronotropic, and inotropic failure results in venous pooling of blood, a decrease in venous return and carbon dioxide, resulting in a low BP. Afferent pathway (red) transfers information from the arterial baroceptors in the carotid arteries and aortic arch. The information reaches the vasomotor centre in the medulla oblongata. The efferent pathway (blue) regulates two responses: HR and vascular tone. An increase in vascular tone is key, whereas the HR is not. Degeneration of autonomic nuclei in the CNS and/or peripheral autonomic denervation may lead to OH and syncope. The circulatory autonomic causes of orthostatic intolerance include classical OH, initial OH, delayed OH, POTS and VVS.
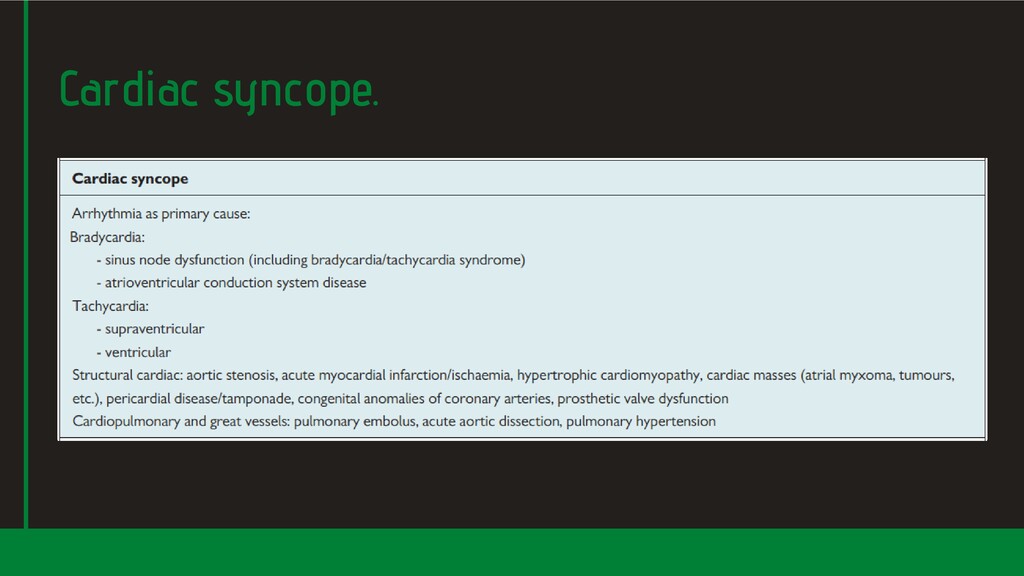
syncope. Pulmonary embolism is frequently overlooked, as is thoracic aortic dissection. Cause syncope through a critical decrease in cardiac output, but there are multiple contributary factors; type of arrhythmia, ventricular rate, LV function, posture and adequacy of vascular compensation. Cause syncope when circulatory demands outweigh the impaired ability of the heart to increase cardiac output. Of significant concern when associated with fixed or dynamic obstruction of LV outflow. Often not soley the result of restricted cardiac output; may in part be related to VV reflex, OH, or arrhythmia. Mechanism of cardiac syncope may be multifactorial. Arrhythmia; Structural heart and great vessels;
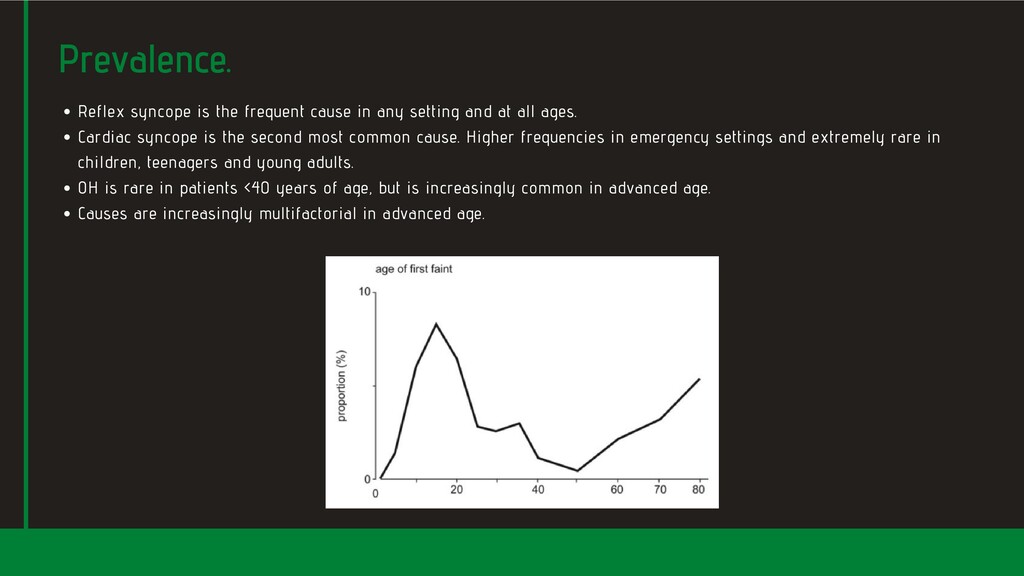
at all ages. Cardiac syncope is the second most common cause. Higher frequencies in emergency settings and extremely rare in children, teenagers and young adults. OH is rare in patients <40 years of age, but is increasingly common in advanced age. Causes are increasingly multifactorial in advanced age. Prevalence.
derived from history taking from patients and witnesses. Initial evaluation should answer: Was there a TLoC? In case of TLoC is it syncopal or non-syncopal? In case of syncope is there a clear aetiological diagnosis? Is there evidence to suggest a high risk of cardiovascular events or death? TLoC has the following 4 specific charcteristics: short duration, abnormal motor control, loss of responsiveness, and amnesia for the period of LoC. TLoC is likely to be syncope when: There are signs and symptoms specific for reflex syncope, OH, or cardiac syncope. Signs and symptoms of other forms of TLoC (head trauma, seizures, psychogenic TLoC) are absent. Through a detailed clinical history clinicians can differentiate syncope from other TLoC in 60% of cases. Initial evaluation.
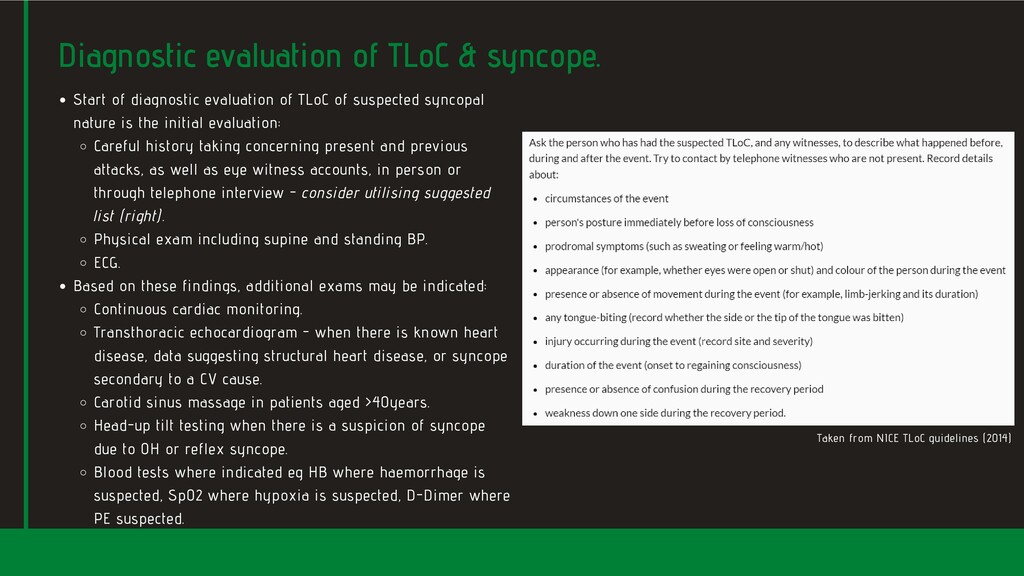
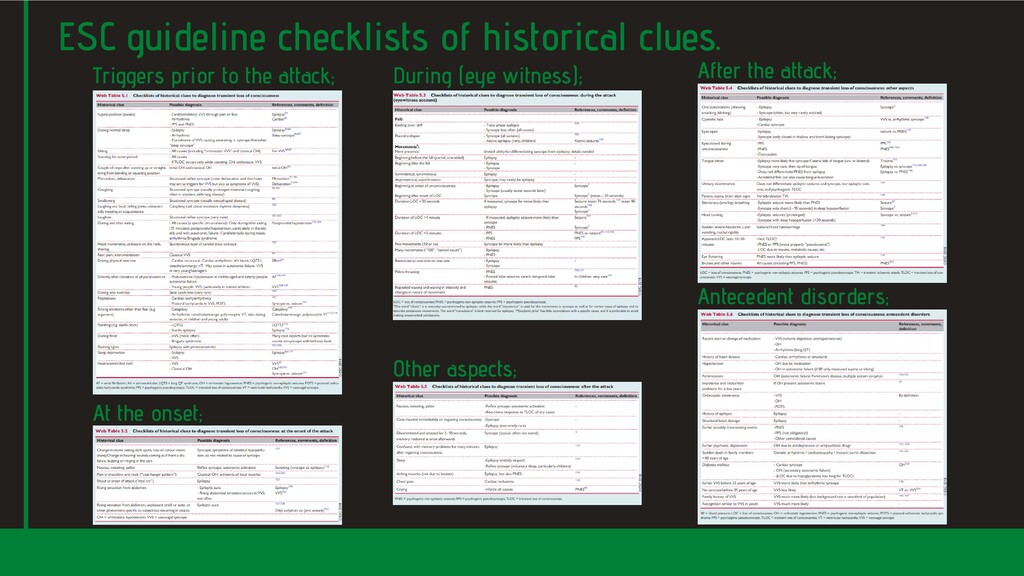
is the initial evaluation: Careful history taking concerning present and previous attacks, as well as eye witness accounts, in person or through telephone interview - consider utilising suggested list (right). Physical exam including supine and standing BP. ECG. Based on these findings, additional exams may be indicated: Continuous cardiac monitoring. Transthoracic echocardiogram - when there is known heart disease, data suggesting structural heart disease, or syncope secondary to a CV cause. Carotid sinus massage in patients aged >40years. Head-up tilt testing when there is a suspicion of syncope due to OH or reflex syncope. Blood tests where indicated eg HB where haemorrhage is suspected, Sp02 where hypoxia is suspected, D-Dimer where PE suspected. Diagnostic evaluation of TLoC & syncope. Taken from NICE TLoC guidelines (2014)
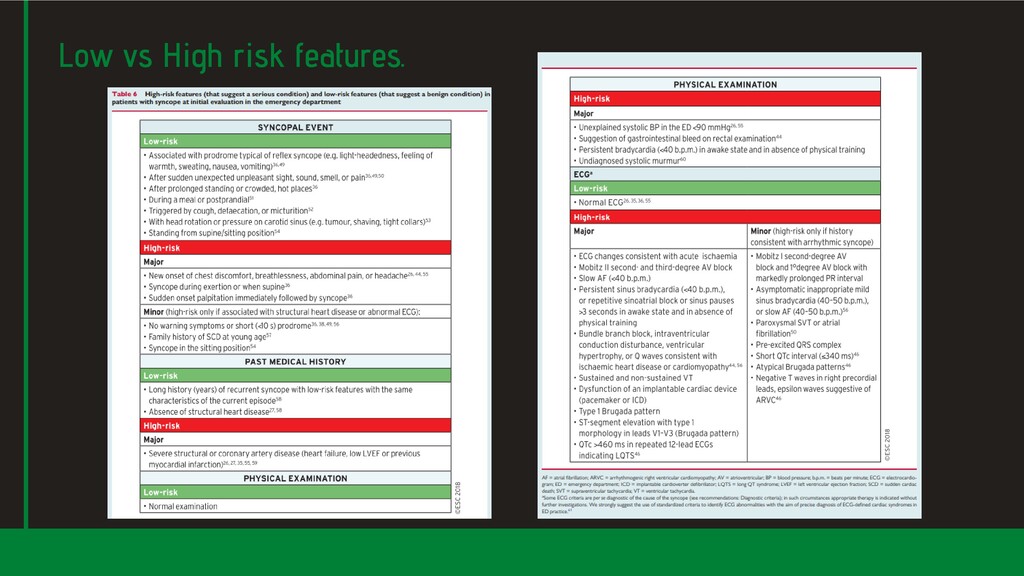
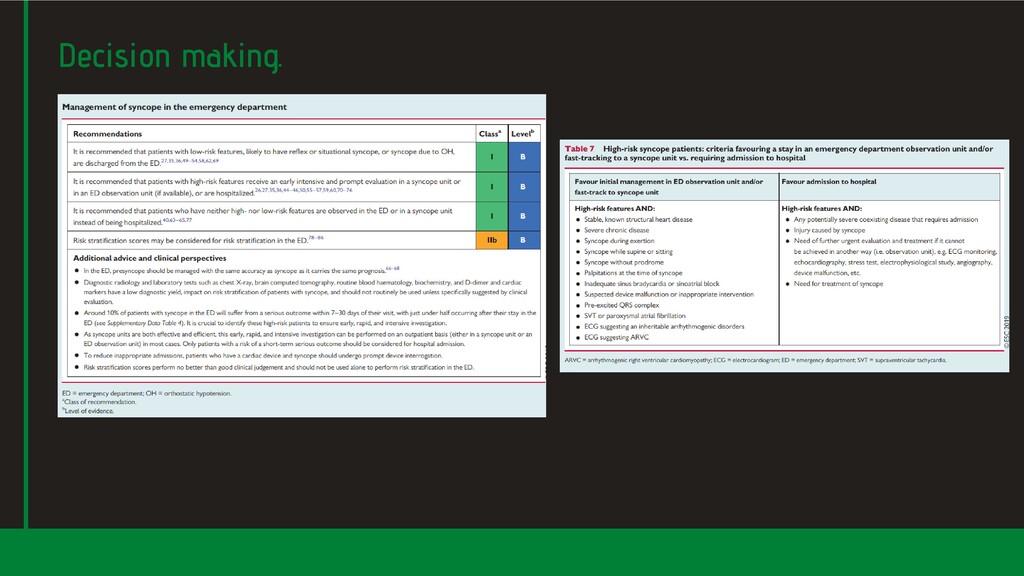
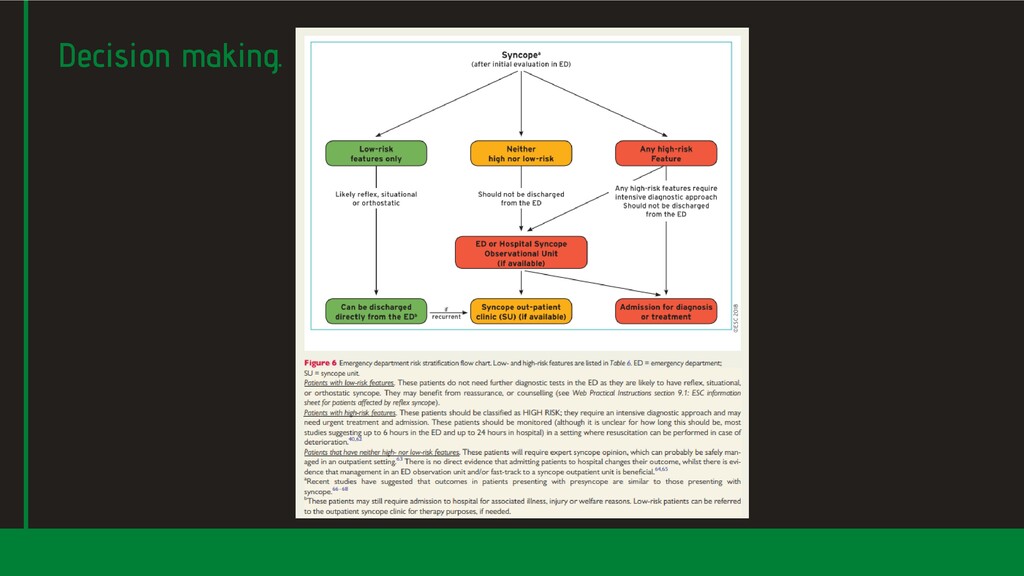
can be identified? Primary aim is to establish underlying cause. Subsequent management will focus on treating this, as this is what determines outcomes, Many (40-45%) life-threatening underlying conditions will be "obvious" in the ED. High/low risk features to follow below. What is the risk of a serious outcome? Low risk = discharge with "adequate"patient education. High risk = urgent investigation; this may require admission. High risk = more likely to have cardiac syncope eg structural heart disease, primary electrical disease (major risk factors for SCD and overall mortality in patients with syncope). Low risk patients more likely to have reflex syncope and have excellent prognosis. OH is associated with 2-fold risk of death (owing to severity of comorbidities) vs general population. Should the patient be admitted to hospital? ~50% syncopes presenting to the ED are admitted. At 7-30 days 0.8% die and 6.9% have non-fatal severe outcomes in the ED, while 3.6% have a post-ED serious outcome. Unnecessary admission of low-risk patients can be harmful and not all high-risk patients need admission. rather than syncope itself. Management in the ED based on risk stratification.
decision rules". Canadian Syncope Risk Score - "Predicts 30-day serious adverse events in EGSYS Score - "Predicts likelihood that syncope is from cardiac cause". OESIL Score - "Estimates 12-month all-cause mortality in patients presenting w/ syncope". San Francisco Syncope Rule - "Predicts risk for serious outcomes at 7 days in patients w/ syncope or near-syncope". ESC described poor sensitivity and specificity reported from external validation studies. These tools/rules perform no better than clinician judgement alone at predicting serious outcomes. patients presenting w/ syncope". (the list goes on). Risk stratification tools.
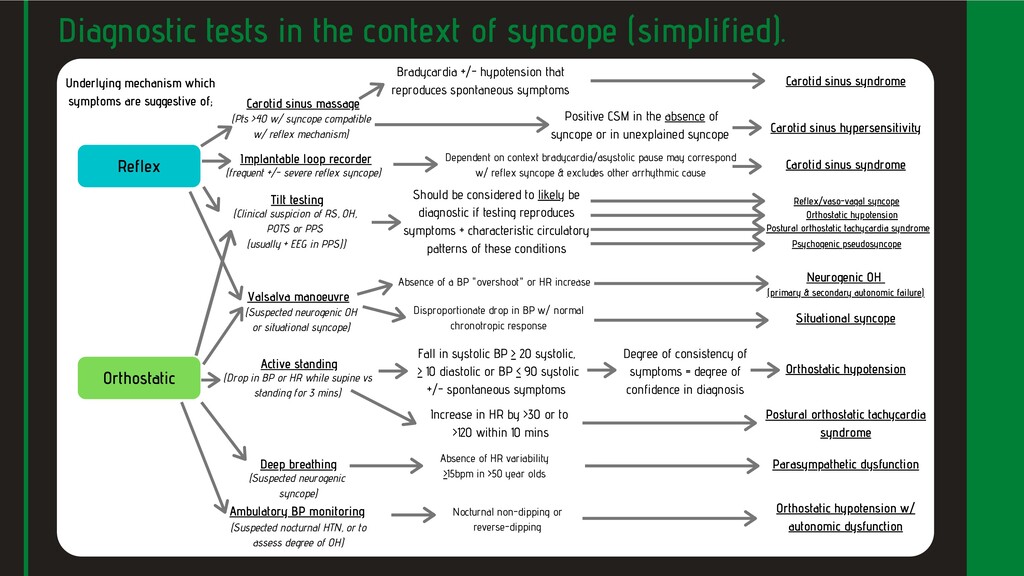
spontaneous symptoms Carotid sinus syndrome Active standing Positive CSM in the absence of syncope or in unexplained syncope Carotid sinus hypersensitivity (Pts >40 w/ syncope compatible w/ reflex mechanism) (Drop in BP or HR while supine vs standing for 3 mins) Orthostatic hypotension Increase in HR by >30 or to >120 within 10 mins Postural orthostatic tachycardia syndrome Degree of consistency of symptoms = degree of confidence in diagnosis (Clinical suspicion of RS, OH, POTS or PPS (usually + EEG in PPS)) Should be considered to likely be diagnostic if testing reproduces symptoms + characteristic circulatory patterns of these conditions Psychogenic pseudosyncope Postural orthostatic tachycardia syndrome Orthostatic hypotension Reflex/vaso-vagal syncope Valsalva manoeuvre Deep breathing Ambulatory BP monitoring Absence of a BP "overshoot" or HR increase Disproportionate drop in BP w/ normal chronotropic response Neurogenic OH (primary & secondary autonomic failure) Situational syncope Parasympathetic dysfunction Orthostatic hypotension w/ autonomic dysfunction Dependent on context bradycardia/asystolic pause may correspond w/ reflex syncope & excludes other arrhythmic cause Diagnostic tests in the context of syncope (simplified). Reflex Underlying mechanism which symptoms are suggestive of; Orthostatic Fall in systolic BP > 20 systolic, > 10 diastolic or BP < 90 systolic +/- spontaneous symptoms Absence of HR variability >15bpm in >50 year olds Nocturnal non-dipping or reverse-dipping (Suspected neurogenic OH or situational syncope) (Suspected neurogenic syncope) (Suspected nocturnal HTN, or to assess degree of OH) Implantable loop recorder (frequent +/- severe reflex syncope) Carotid sinus syndrome
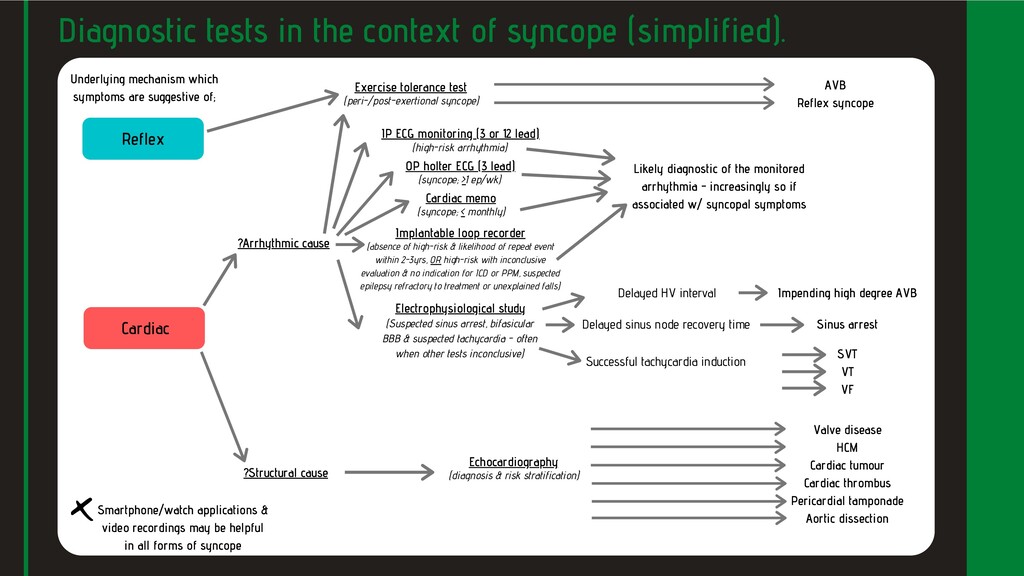
OP holter ECG (3 lead) (syncope; >1 ep/wk) (absence of high-risk & likelihood of repeat event within 2-3yrs, OR high-risk with inconclusive evaluation & no indication for ICD or PPM, suspected epilepsy refractory to treatment or unexplained falls) Cardiac memo (syncope; < monthly) ?Arrhythmic cause ?Structural cause Electrophysiological study (Suspected sinus arrest, bifasicular BBB & suspected tachycardia - often when other tests inconclusive) Delayed HV interval Impending high degree AVB Successful tachycardia induction SVT VT VF Sinus arrest Echocardiography (diagnosis & risk stratification) Valve disease HCM Cardiac tumour Cardiac thrombus Pericardial tamponade Aortic dissection Underlying mechanism which symptoms are suggestive of; Cardiac IP ECG monitoring (3 or 12 lead) Smartphone/watch applications & video recordings may be helpful in all forms of syncope Implantable loop recorder Delayed sinus node recovery time Likely diagnostic of the monitored arrhythmia - increasingly so if associated w/ syncopal symptoms Reflex Exercise tolerance test (peri-/post-exertional syncope) AVB Reflex syncope
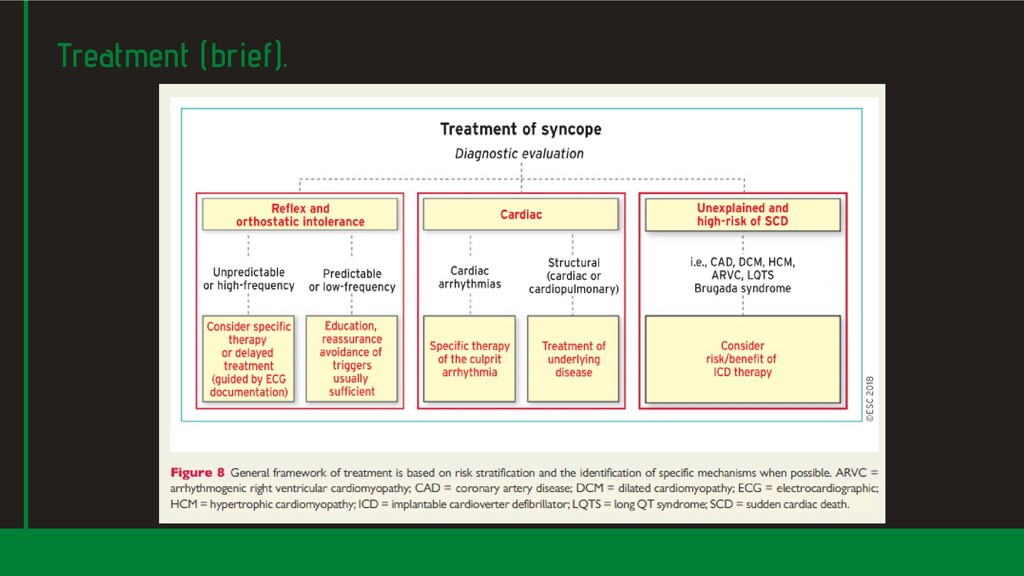
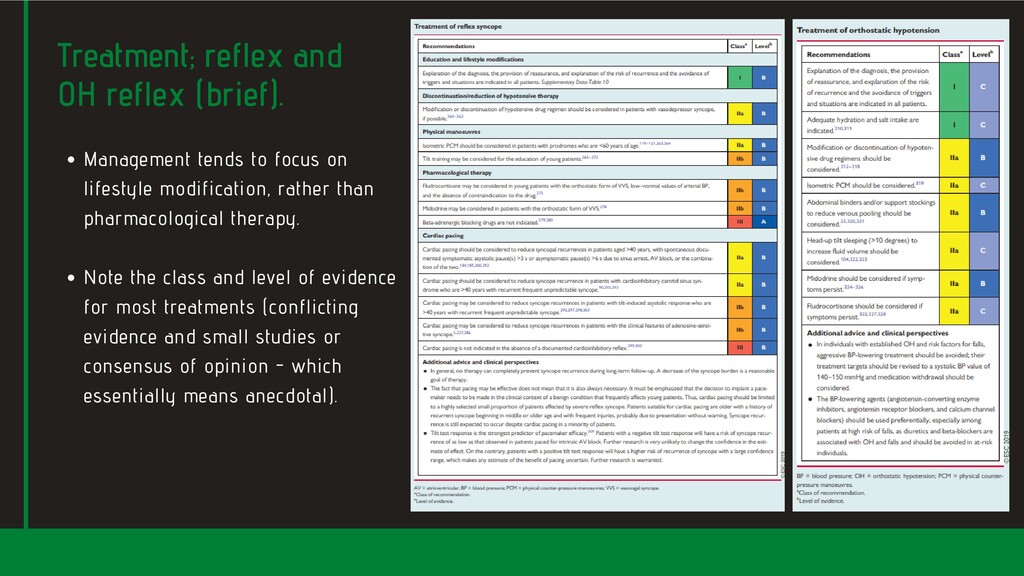
on Note the class and level of evidence for most treatments (conflicting evidence and small studies or consensus of opinion - which essentially means anecdotal). lifestyle modification, rather than pharmacological therapy.
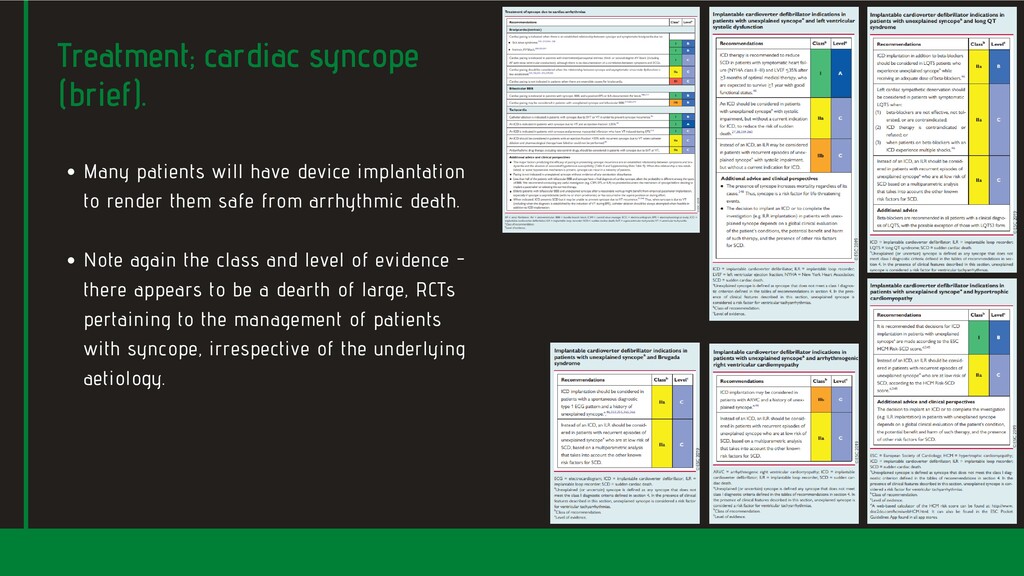
to render them safe from arrhythmic death. Note again the class and level of evidence - there appears to be a dearth of large, RCTs pertaining to the management of patients with syncope, irrespective of the underlying aetiology.
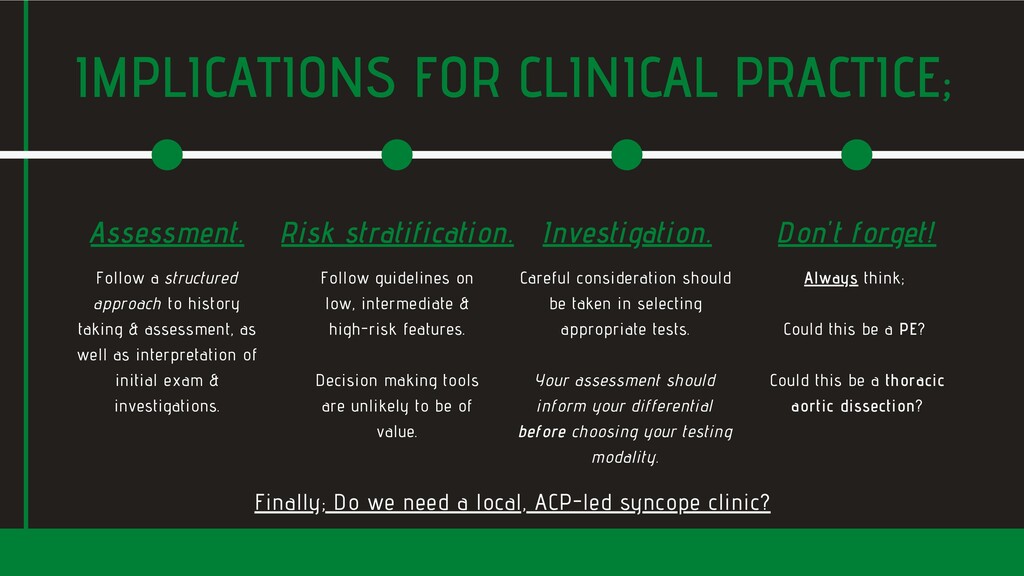
taking & assessment, as well as interpretation of initial exam & investigations. Assessment. Follow guidelines on low, intermediate & high-risk features. Decision making tools are unlikely to be of value. Risk stratification. Careful consideration should be taken in selecting appropriate tests. Your assessment should inform your differential before choosing your testing modality. Investigation. Always think; Could this be a PE? Could this be a thoracic aortic dissection? Don't forget! Finally; Do we need a local, ACP-led syncope clinic?
P.M., Fanciulli, A., Fedorowski, A., Furlan, R., Kenny, R.A., Martín, A. and Probst, V., 2018. 2018 ESC Guidelines for the diagnosis and management of syncope. European heart journal, 39(21), pp.1883-1948.Vancouver. Rogers, G. and O'Flynn, N., 2011. NICE guideline: transient loss of consciousness (blackouts) in adults and young people. Br J Gen Pract, 61(582), pp.40-42.Vancouver REFERENCES:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}