greater than the set pacemaker rate along with a pacemaker in an asynchronous mode, an R on T phenomenon may occur leading to ventricular tachycardia or ventricular fibrillation. Asynchronous pacemaker modes (i.e. DOO VOO AOO) are those in which the pacemaker neither senses nor inhibits. Regardless of the underlying rhythm or intrinsic heart rate, a pacemaker in an asynchronous mode will pace at whatever rate it is set. This mode is most commonly used perioperatively in pacemaker-dependent patients in order to decrease problems associated with electromagnetic interference (EMI) from the electrocautery unit (ECU). For example, a patient with complete heart block has a DDD pacemaker in place. The pacemaker detects the AMI from the ECU and interprets it as R waves. Since the pacemaker thinks the patient’s ventricle is therefore beating, the pacemaker inhibits itself. In a patient with CHB, no pacing can mean bradycardia or even asystole and hemodynamic instability. To prevent this complication, the pacemake may be changed to DOO perioperatively. Then the pace will consistently pace at a set rate (commonly 80 to 100) and will not sense the EMI.
HTN suffered an episode of chest pain and syncope at home, just 12 hours after returning from the hospital. She was recently discharged home 5 days after a hysterectomy for uterine fibroids. Postoperatively, she developed a UTI. She received IV cefepime in the hospital for 3 days. On the day of discharge, she was provided with a prescription for ciprofloxacin. On arrival to the hospital, she is in obvious distress – sweating, SOB, confused, and speaking in short sentences. Her extremities are cold and pale and neck veins are distended. Vital signs are: T38.2 C, HR 126, BP 76/42, RR 28, SpO2 82% on RA. She is intubated and a PA catheter is placed: ETCO2: 32 mmHg (PaCO2 59 on ABG) CVP: 18 mmHg PCWP: 14 mmHg CI: 1.9 L/min/m^2 SVR: 2200 dynes*sec/cm^5 What type of shock does the patient most likely have? A. anaphylactic B. distributive C. hypovolemic D. obstructive
output, most likely due to pericardial tamponade, PE or a tension PTX. The patient will present with low CI, high CVP, high SVR. Distributive shock will have a reduced SVR, increased CI Anaphylactic shock is a form of distributive shock Cardiogenic shock will have a reduced CI, increased SVR and increased PCWP, similar to obstructive Hypovolvemic shock will have reduced CVP, increased SVR, normal CI
in regard to anti-emetic effects, it appears to have inhibitory action at the nucleus tractus soletarii. PONV is mediated by muscarinic (M1), dopaminergic (D2), histamine (H1), serotonin and neurokinin (NK1) receptors
the ED after escaping a fire in a tire factory. He initially complains of nausea and soon is unresponsive. His heart rate is 50 bpm and his BP is 90/40. Which of the following is the most appropriate first line therapy? A) Amyl nitrite B) Hydroxocobalamin C) Sodium nitrite D) Sodium thiosulfate
for cyanide poisoning. Cyanide toxicity is most commonly seen in industrial fires. Symptoms are often vague and include GI, CV and neurologic symptoms. Prolonged exposure to sodium nitroprusside can cause this as well. ABG shows normal oxygenation with metabolic acidosis Hydroxocobalamin is now the treatment of choice though sodium nitrite or amyl nitrite are approved (though older with more side effects) treatments. Sodium thiosulfate is effective though has extremely slow onset of action.
of pH-stat management during deep hypothermic circulatory arrest? A) improved oxygen tissue delivery B) improved reduction in cerebral metabolic rate of oxygen demand C) increased speed of homogenous cerebral cooling D) reduced delivery of emboli to the brain
and a DECREASE in PaCO2 . pH stat corrects alkaline drift by maintaining a constant pH (adds CO2 to the body) Advantages Increased speed of cerebral cooling through cerebral vasodilation, Improved oxygen delivery by reducing leftward shift of oxyhemoglobin dissociation curve Disadvantages include an increased delivery of embolic load to the brain as a result of cerebral vasodilation as well as loss of cerebral autoregulation.
nitrous oxide in a term neonate with a right-to-left intracardiac shunt. The ETCO2 remains stable at 35 during the induction. Which of the following statements is the most accurate to describe the impact of the right-to-left shunt on the wash-in (FA/FI) of this inhaled induction? A. With a right-to-left shunt, using halothane would provide a more rapid wash-in. B. With a right-to-left shunt, the maximum depth achieved during an inhaled induction is increased. C. With a right-to-left shunt, the sevoflurane partial pressure in the pulmonary veins is reduced. D. With a right-to-left shunt, a change in cardiac output would have no effect on the FA/FI.
shunt is that blood from the right side of the heart (yet to pass through the lungs and pick up inhalational agent) dilutes blood on the left side (full of inhalational agent). Therefore right to left shunt slows inhalational induction This effect is greatest for insoluble agents (Desflurane) because there is no ”reservoir” of dissolved gas and dilution is unopposed.
in the setting of septic shock, which of the following statements is most accurate? A) Normal saline resuscitation is associated with hyponatremic hypochloremic metabolic acidosis B) Patients resuscitated with albumin had an increased incidence of mortality caused by renal failure C) Patients treated with albumin have increased coagulopathy compared to the saline group D) There is no significant mortality difference between patients resuscitated with albumin or normal saline
that resuscitation with albumin vs saline show no difference in hospital or 90 day mortality Large amounts of normal saline can result in a hyperchloremic hypernatremic metabolic acidosis Albumin is generally not associated with renal failure but hetastarch can be Hetastarch can reduce factor VII levels which can prolong PTT and increase coagulopathy
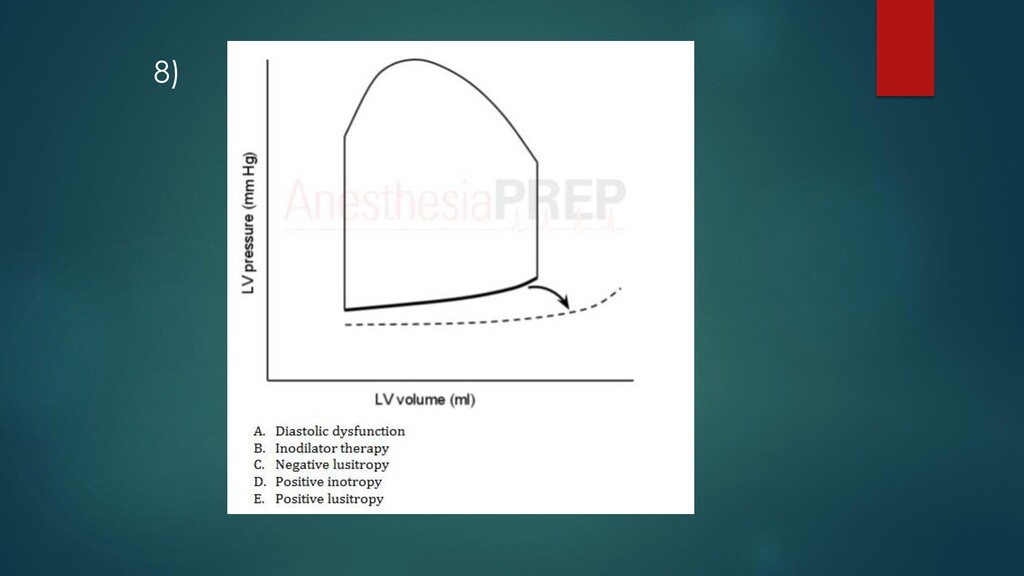
illustrated on the pressure-volume loop as a reduction in the slope and a rightward shift of the diastolic filling phase This results in a reduction in end diastolic filling pressure (LVEDP) which leads to increased coronary perfusion pressure (since coronary perfusion pressure is dependent on LVEDP.
not cross the blood brain barrier. It is able to counteract the negative effects of mu receptors in the GI tract but allows function of opioid medications in the central nervous system.
elective hernia repair but his only IV is infiltrated. An intramuscular (IM) injection is considered. Which of the following medications should NOT be administered intramuscularly to improve his blood pressure? A) Ephedrine B) Epinephrine C) Norepinephrine D) Phenylephrine
when IV or IO access is not readily available Atropine Glycopyrrolate Ephedrine Phenylephrine Epinephrine Vasopressin (though minimal cardiovascular effect is seen by this route) Norepinephrine should NOT be given IM Potent α constriction Much greater than β activity IM injection or extravasation into tissues can cause ischemia that leads to necrosis Phentolamine should be injected if infiltration with norepinephrine is suspected
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}