Yip2, PhilippaMiddleton3, Allan M Cyna1, Alison V Carlyle4 1Department of Women’sAnaesthesia, Women’sand Children’sHospital, Adelaide, Australia. 2Department of Paediatric Anaesthesia, StarshipChildren’sHospital,Auckland,NewZealand.3ARCH:AustralianResearchCentrefor Healthof WomenandBabies,Discipline of Obstetrics and Gynaecology, The University of Adelaide, Adelaide, Australia. 4Department of Anaesthesia, Princess Margaret Hospital, Subiaco, Australia Contact address: Allan M Cyna, Department of Women’s Anaesthesia, Women’s and Children’s Hospital, 72 King William Road, Adelaide, South Australia, 5006, Australia. allan.cyna@ health.sa.gov.au. Editorial group: CochraneAnaesthesiaGroup. Publication statusand date: Edited (no changeto conclusions), published in Issue11, 2010. Review content assessed asup-to-date: 13 December 2008. Citation: Yip P , Middleton P , CynaAM, CarlyleAV. Non-pharmacological interventionsfor ass isting theinduction of anaesthesiain children. CochraneDatabas eof S ys te maticReviews2009, Issue3. Art. No.: CD006447. DOI: 10.1002/14651858.CD006447.pub2. Copyright © 2010 TheCochraneCollaboration. Published by John Wiley & Sons, Ltd. A B S T R A C T Background Induction of general anaesthesia can be distressing for children. Non-pharmacological methodsfor reducing anxiety and improving co-operation may avoid theadverseeffectsof preoperativesedation. Objectives To assesstheeffectsof non-pharmacological interventionsin assisting induction of anaesthesiain children by reducing their anxiety, distressor increasing their co-operation. Search methods Wesearched CENTRAL (TheCochraneLibrary2009, Issue1). Wesearched thefollowingdatabasesfrom inception to 14th December 2008: MEDLINE, PsycINFO, CINAHL, DISSERTATION ABSTRACTS, Web of Scienceand EMBASE. Selection criteria Weincluded randomized controlled trialsof anon-pharmacological intervention implemented on theday of surgery or anaesthesia. Data collection and analysis Two authorsindependently extracted dataand assessed risk of biasin trials. Main results We included 17 trials, all from developed countries, involving 1796 children, their parents or both. Eight trials assessed parental presence. Noneshowed significant differencesin anxiety or co-operation of children during induction, except for onewhereparental presencewassignificantly lesseffectivethan midazolam in reducing children’sanxiety at induction. Six trialsassessed interventionsfor children. Preparation with acomputer packageimproved co-operation compared with parental presence(onetrial). Children playing hand-held video gamesbeforeinduction weresignificantly lessanxiousthan controlsor premedicated children (onetrial). Compared with controls, clown doctorsreduced anxiety in children (modified YalePreoperativeAnxiety Scale(mYPAS): mean difference(MD)
{kind=link}
{kind=link}
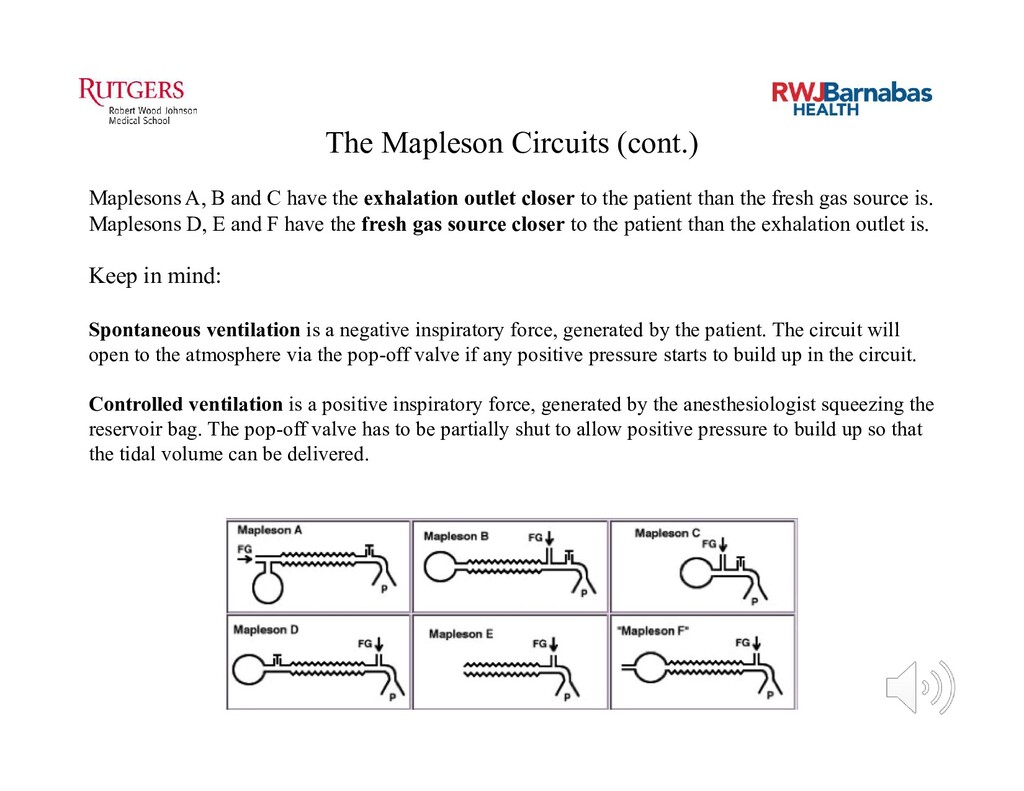
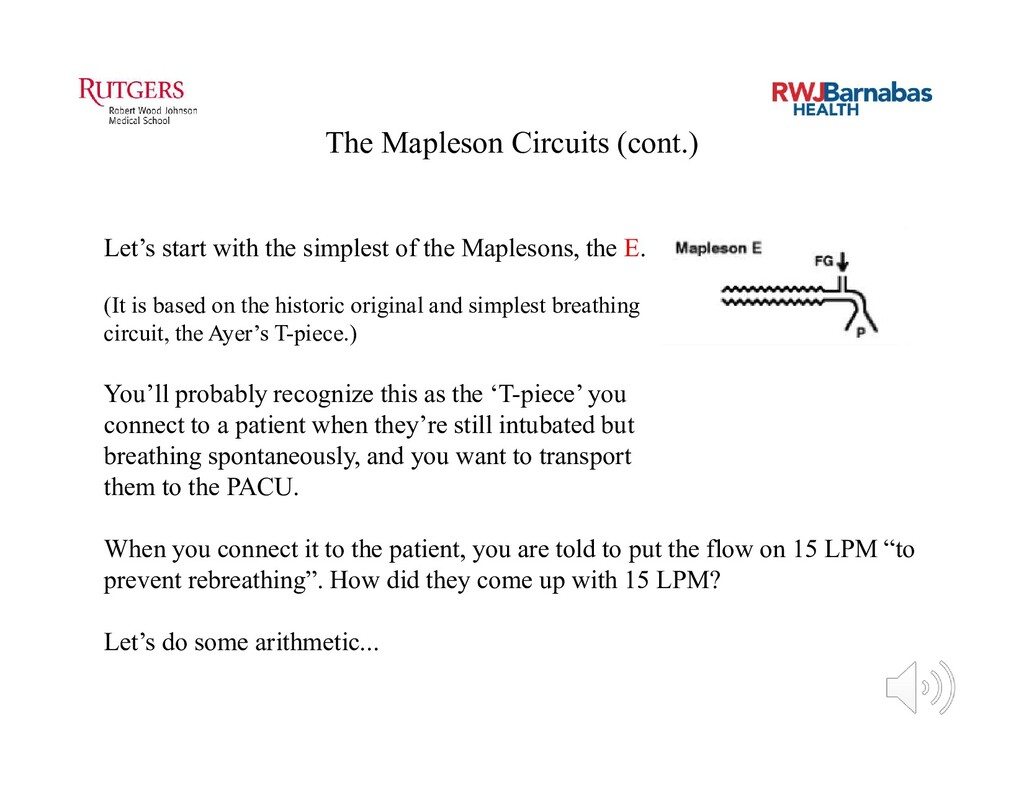
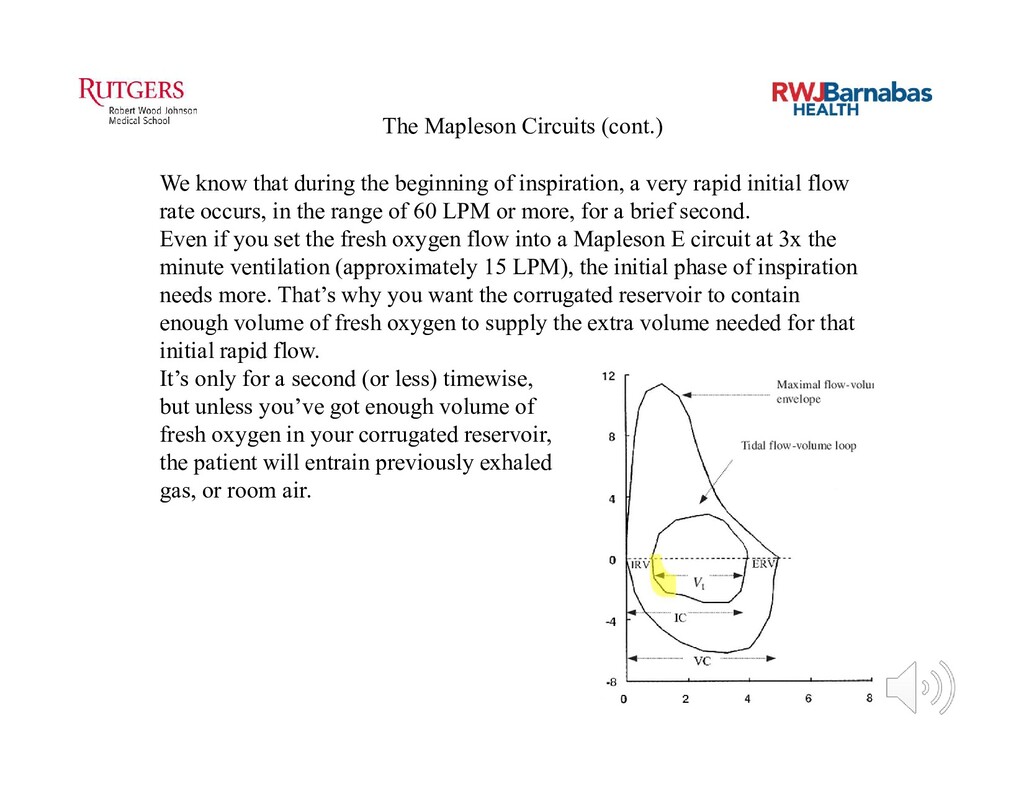
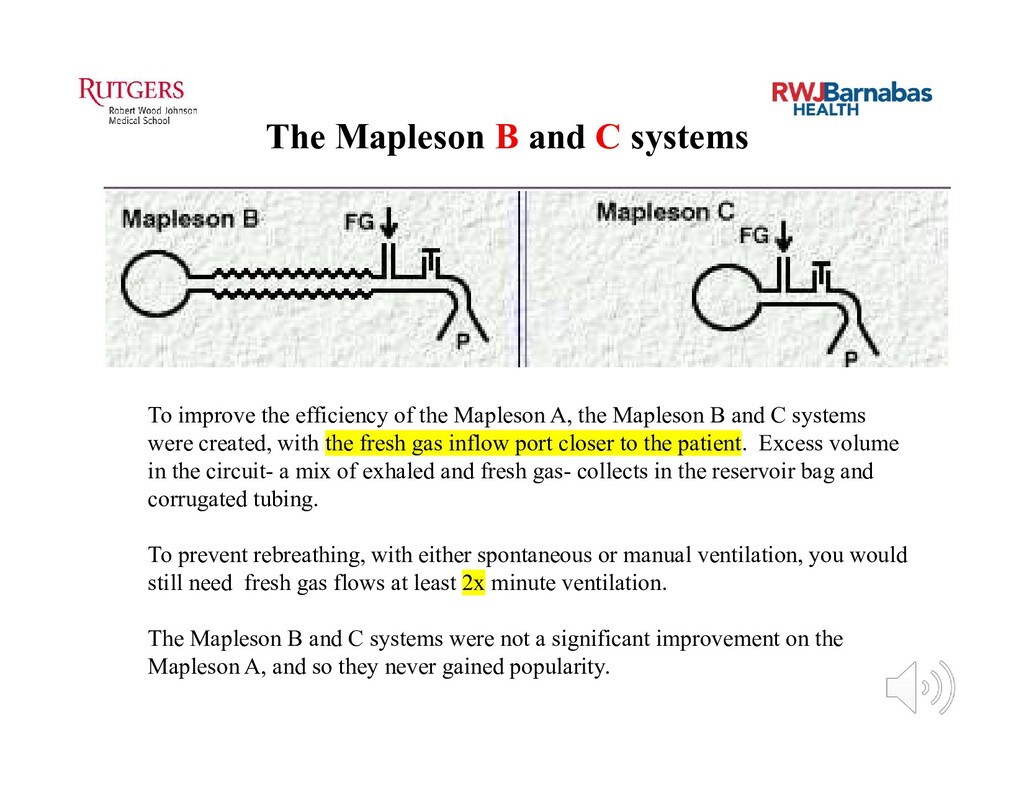
![Mapleson Breathing Circuits In 1954, Dr. William Mapleson [1926-2018], a](https://files.speakerdeck.com/presentations/6292e4426fdf422f9c2cfcbb5c45f908/slide_2.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}