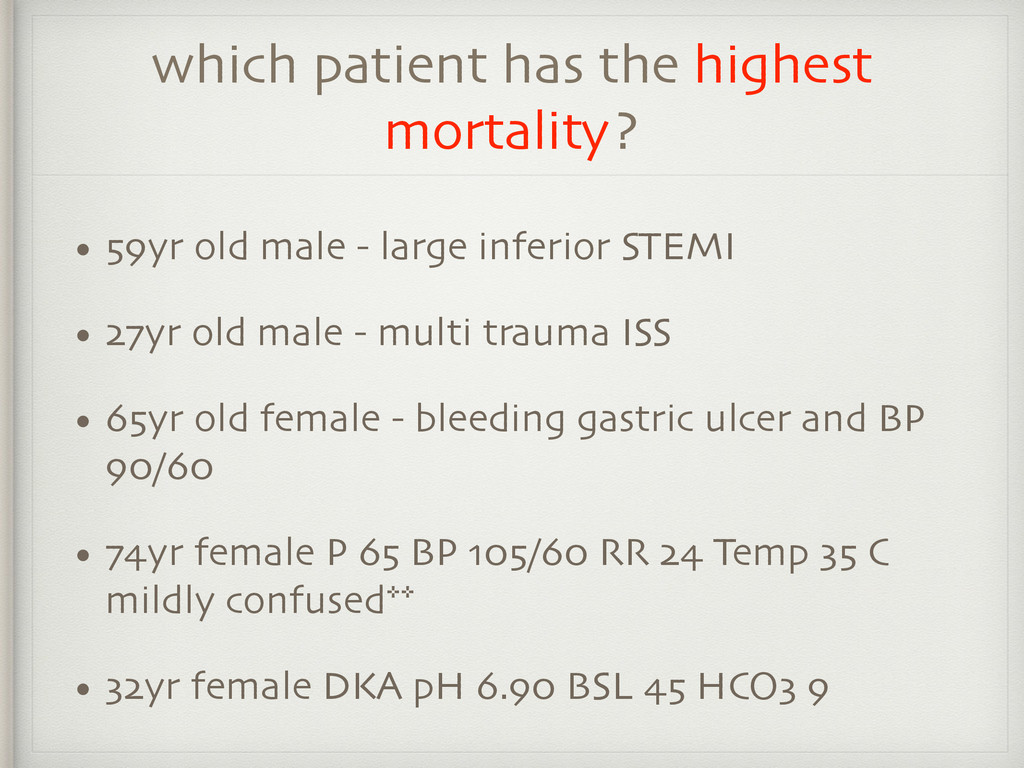
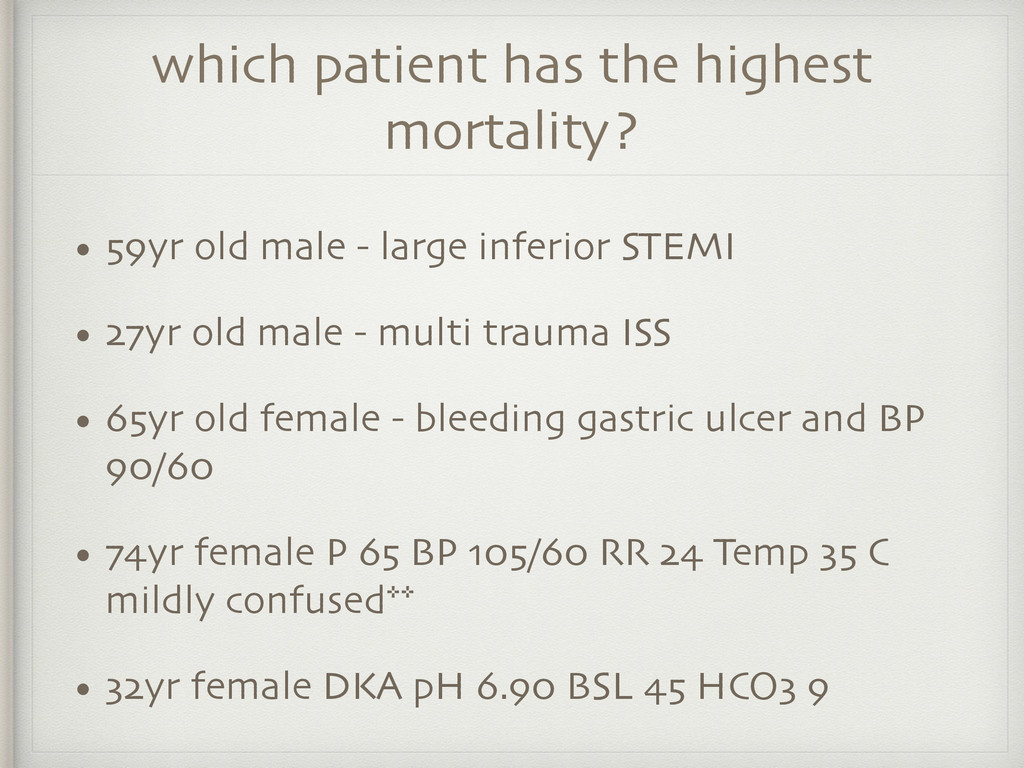
- large inferior STEMI • 27yr old male - multi trauma ISS • 65yr old female - bleeding gastric ulcer and BP 90/60 • 74yr female P 65 BP 105/60 RR 24 Temp 35 C mildly confused** • 32yr female DKA pH 6.90 BSL 45 HCO3 9
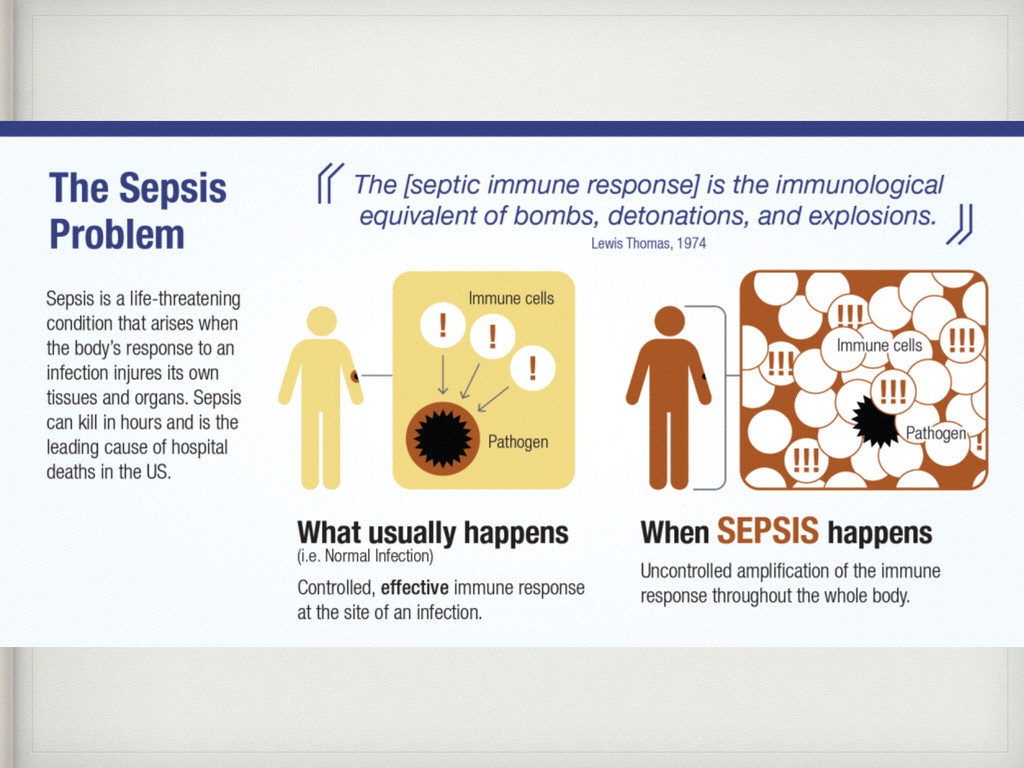
a systemic response • Expect the patient to have signs and symptoms of a systemic response • May not always have symptoms and signs at the site of infection
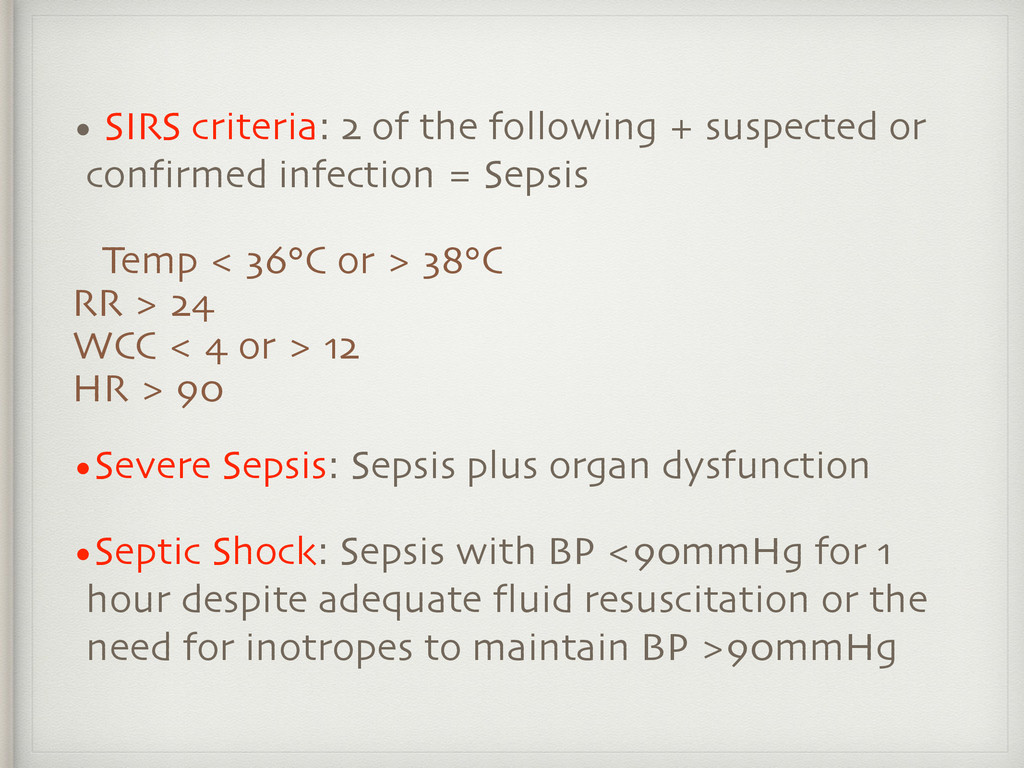
confirmed infection = Sepsis Temp < 36°C or > 38°C RR > 24 WCC < 4 or > 12 HR > 90 •Severe Sepsis: Sepsis plus organ dysfunction •Septic Shock: Sepsis with BP <90mmHg for 1 hour despite adequate fluid resuscitation or the need for inotropes to maintain BP >90mmHg
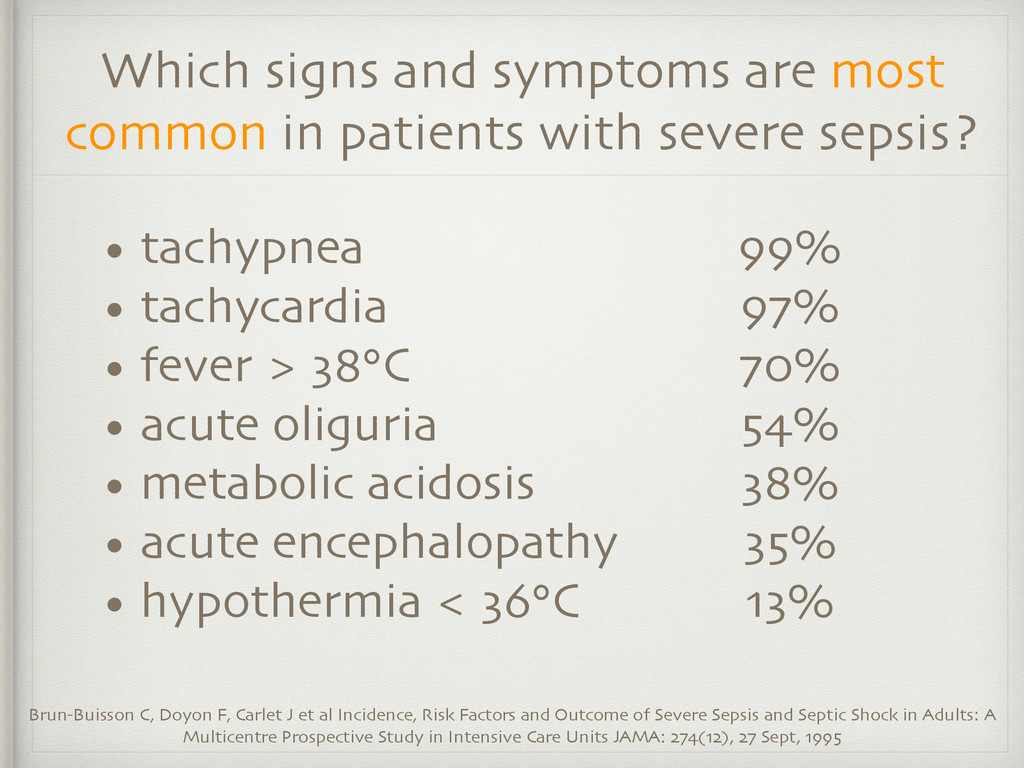
oliguria • metabolic acidosis • acute encephalopathy • hypothermia < 36°C Which signs and symptoms are most common in patients with severe sepsis? Brun-Buisson C, Doyon F, Carlet J et al Incidence, Risk Factors and Outcome of Severe Sepsis and Septic Shock in Adults: A Multicentre Prospective Study in Intensive Care Units JAMA: 274(12), 27 Sept, 1995 99% 97% 70% 54% 38% 35% 13%
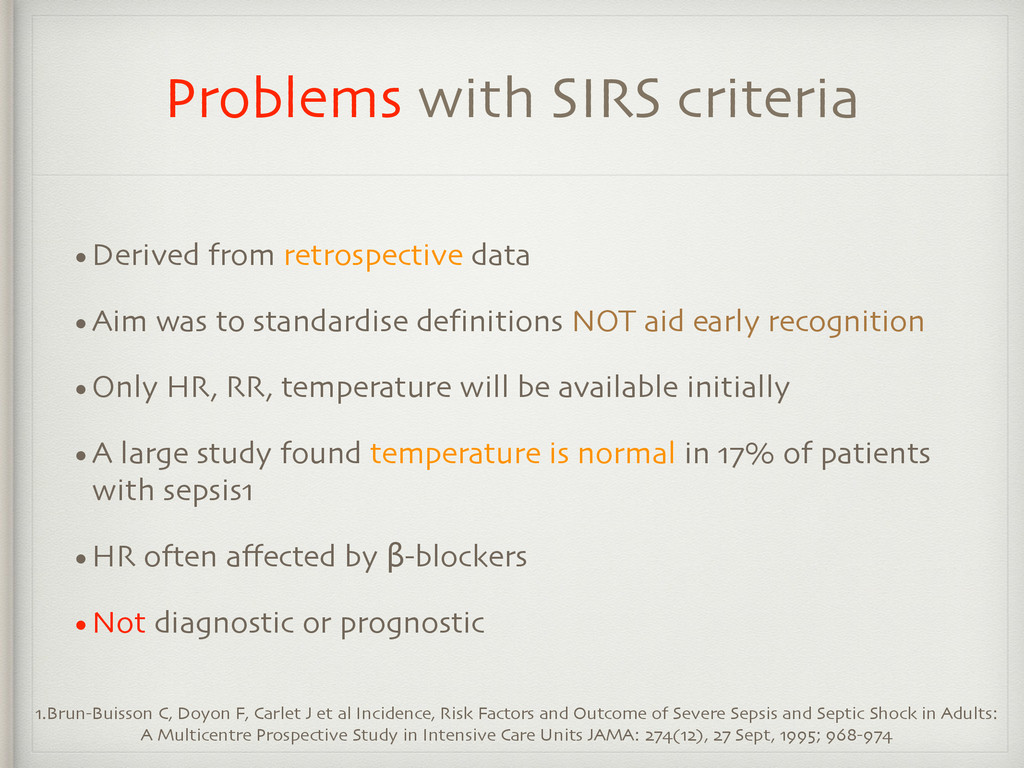
to standardise definitions NOT aid early recognition •Only HR, RR, temperature will be available initially •A large study found temperature is normal in 17% of patients with sepsis1 •HR often affected by β-blockers •Not diagnostic or prognostic 1.Brun-Buisson C, Doyon F, Carlet J et al Incidence, Risk Factors and Outcome of Severe Sepsis and Septic Shock in Adults: A Multicentre Prospective Study in Intensive Care Units JAMA: 274(12), 27 Sept, 1995; 968-974
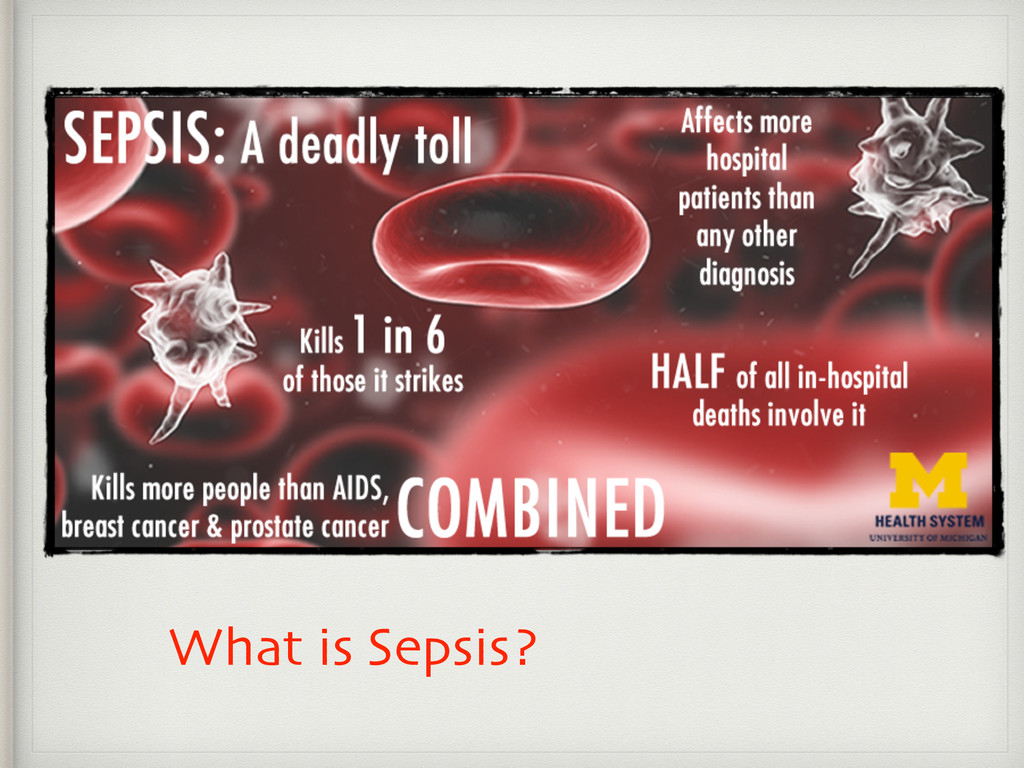
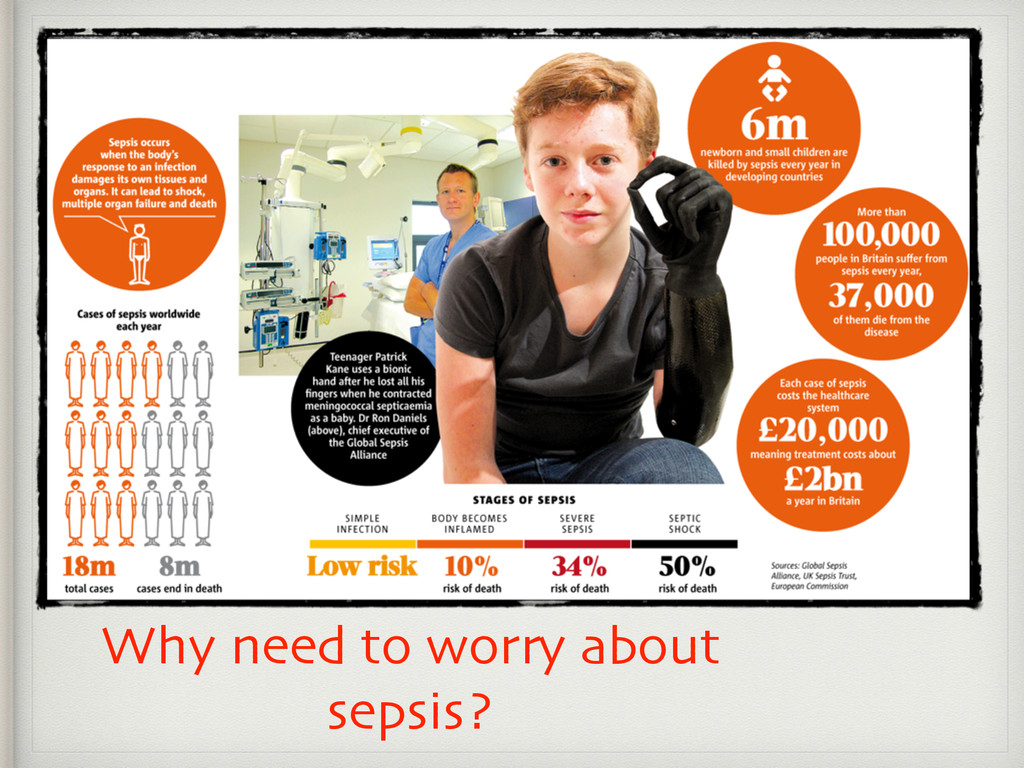
shock increased from 7.7% of ICU admissions to 14.0 % in Australia (4 fold increase in total patients)1 More common in the elderly —> incidence increases as the population ages •Cost The cost of care is huge (US$16.7 billion in 2001)2 1. Peake S, for the ARISE Investigators: The outcome of sepsis and septic shock presenting to the Emergency Department in Australia and New Zealand. Critical Care 2007, 11(Suppl 2):P73 2. Angus DC et al: Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit Care Med 29:1303, 2001
- large inferior STEMI • 27yr old male - multi trauma ISS • 65yr old female - bleeding gastric ulcer and BP 90/60 • 74yr female P 65 BP 105/60 RR 24 Temp 35 C mildly confused** • 32yr female DKA pH 6.90 BSL 45 HCO3 9
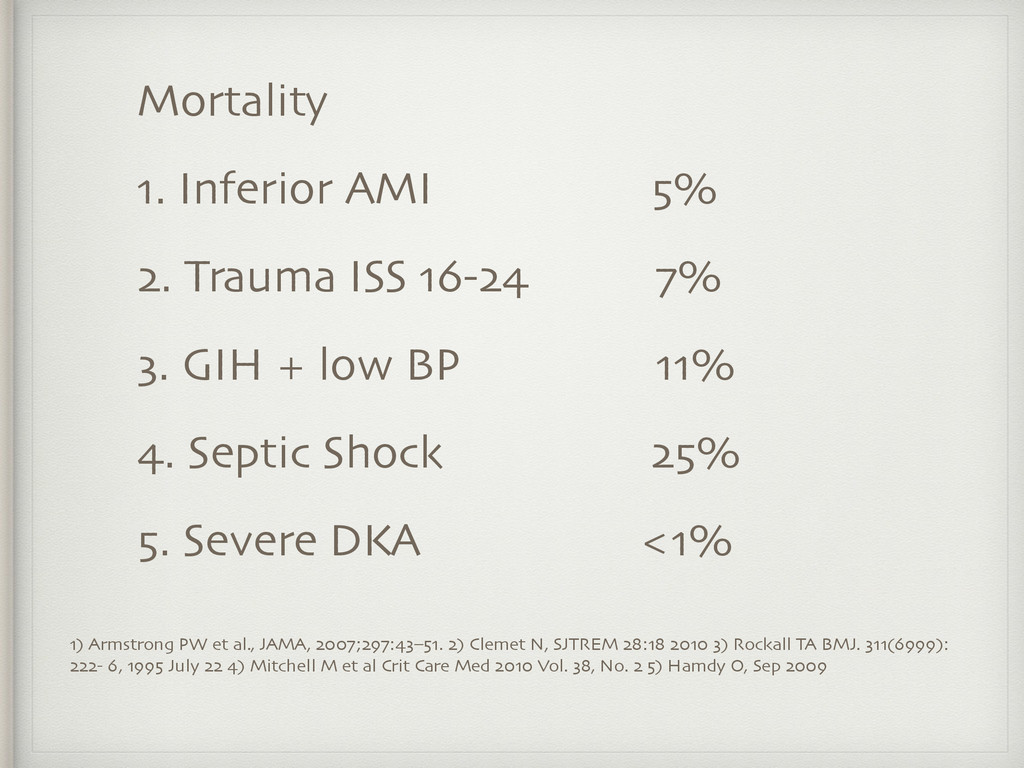
SJTREM 28:18 2010 3) Rockall TA BMJ. 311(6999): 222- 6, 1995 July 22 4) Mitchell M et al Crit Care Med 2010 Vol. 38, No. 2 5) Hamdy O, Sep 2009 Mortality 1. Inferior AMI 5% 2. Trauma ISS 16-24 7% 3. GIH + low BP 11% 4. Septic Shock 25% 5. Severe DKA <1%
and quality improvement in the NSW public health system. It was established in 2004 to promote and support improved clinical care, safety and quality across NSW. The SEPSIS KILLS program aims to reduce preventable harm to patients through improved recognition and management of severe infection and sepsis in emergency departments and inpatient wards throughout NSW. The Clinical Excellence Commission (CEC) Clinical Focus Report on Recognition and Management of Sepsis found deficits in a range of clinical settings in NSW health care facilities in 2009. The lack of timely recognition and appropriate management was further demonstrated in the findings from the CEC Quality Systems Assessment. The focus of the program is: RECOGNISE risk factors, signs and symptoms of sepsis RESUSCITATE with rapid intravenous fluids and antibiotics within the first hour of recognition of sepsis REFER to senior clinicians and specialty teams, including retrieval as required The SEPSIS KILLS program is a quality improvement initiative that has been developed from international evidence-based practice. The goal is to reduce preventable harm to patients with sepsis through early recognition and prompt management.
Hour (Dr. R Adam Cowley, surgeon) • AMI Time is muscle (Dr. Eugene Braunwald, cardiologist) • STROKE Time is Brain (Dr. Morgan Campbell, neurologist) • SEPSIS KILLS TIME IS LIFE
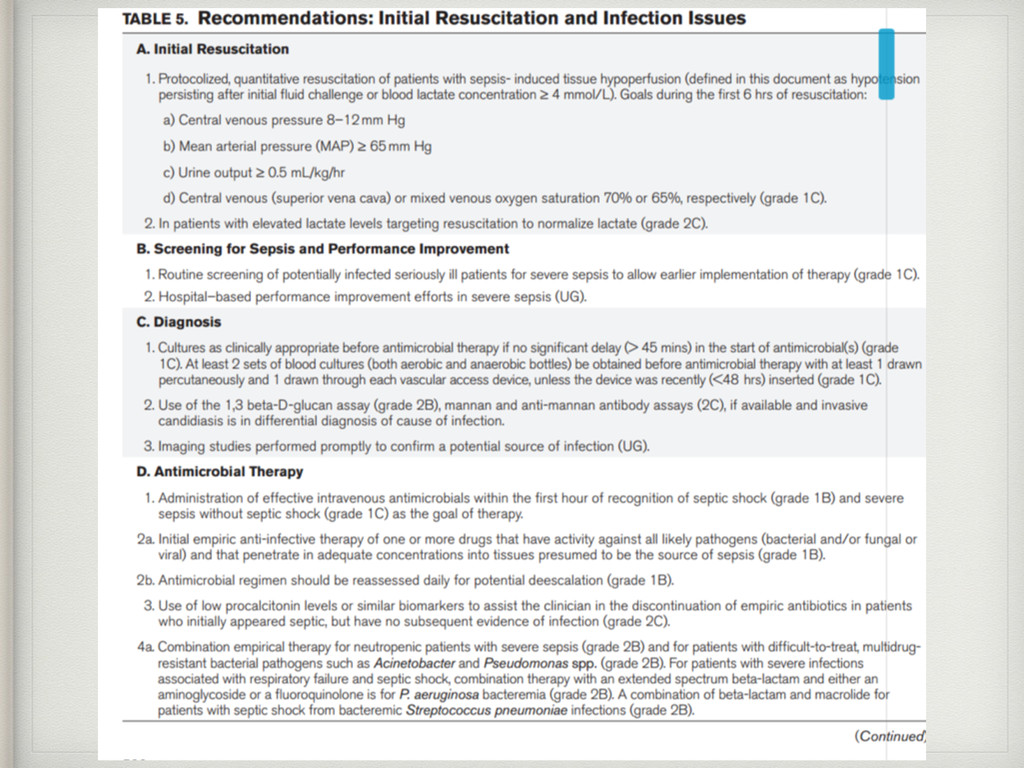
Society of Critical Care Medicine and the European Society of Intensive Care Medicine committed to reducing mortality from severe sepsis and septic shock worldwide. Initiated in 2002, the Campaign progressed in phases that have expanded the scope and reach of the Campaign via publication of 3 editions of evidence-based guidelines, implementation of a performance improvement program, and analysis and publication of data from more than 30,000 patient charts collected around the world. Now recommitted to increasing the number of hospitals contributing data to 10,000 worldwide; to applying the guidelines to 100% of patients in whom the diagnosis is suspected; and to developing a strategy to improve the care of septic patients in underresourced areas. The potential to save lives is enormous. Assuming that the reduction in mortality seen to date can be sustained and 10,000 hospitals comply with the Campaign recommendations, we could save 400,000 lives if we treat only half of the eligible patients with the Surviving Sepsis Campaign Bundles.
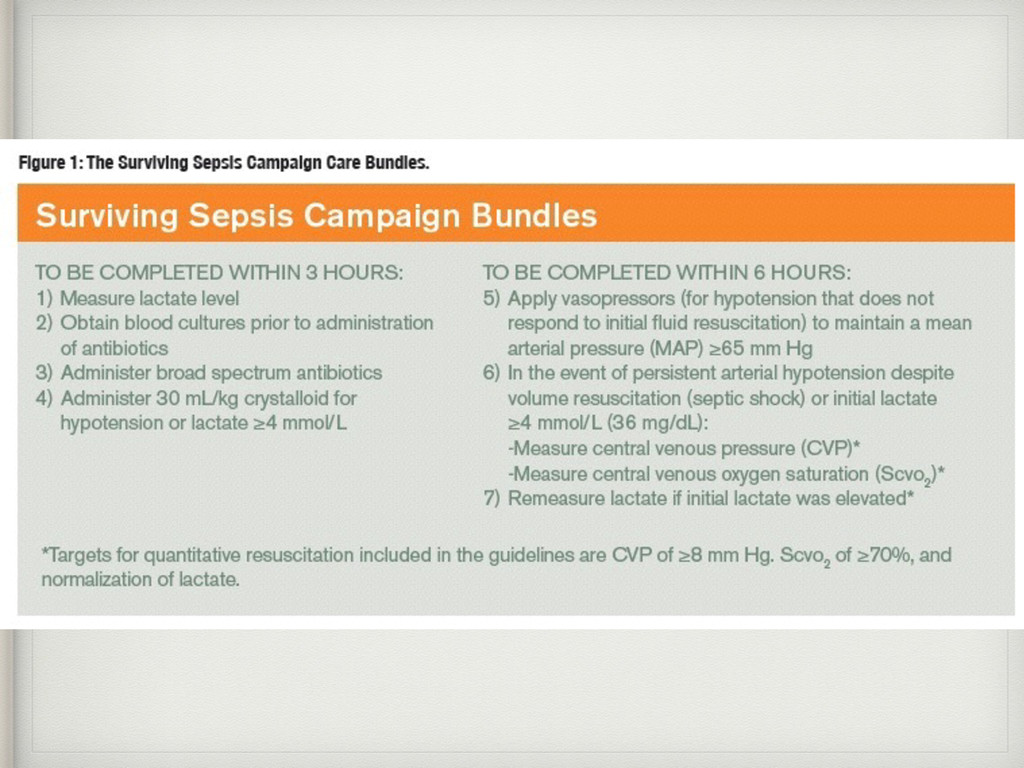
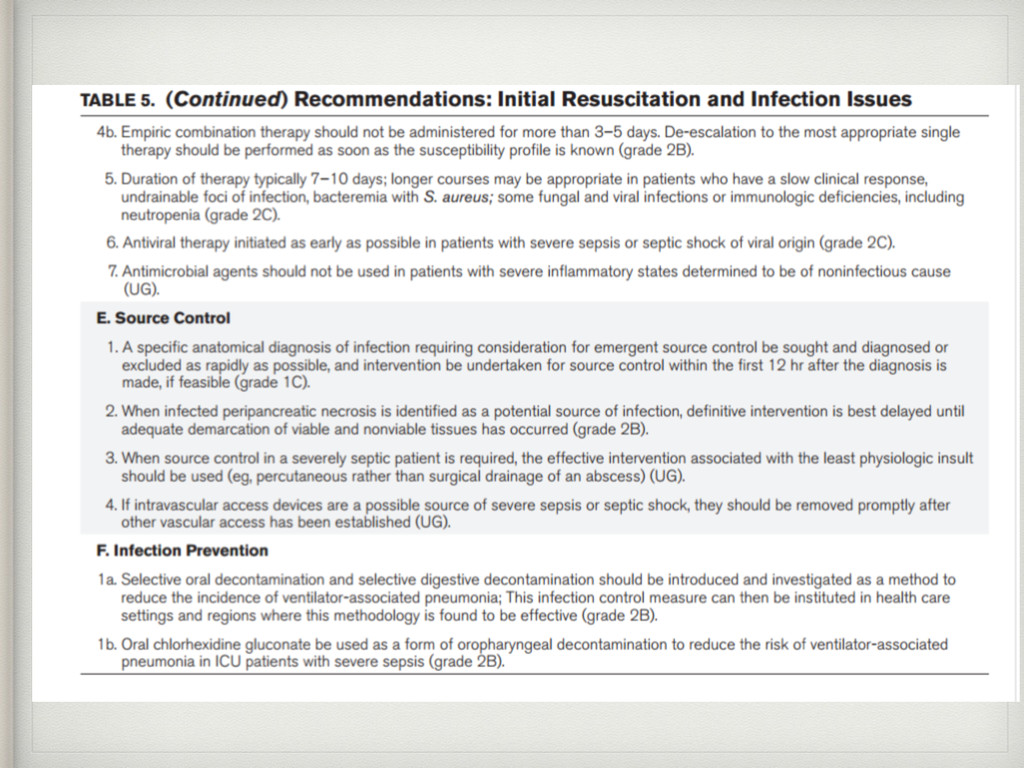
lactate level • 2. Obtain blood cultures prior to administration of antibiotics • 3. Administer broad spectrum antibiotics • 4. Administer 30ml/kg crystalloid for hypotension or lactate ≥4mmol/L
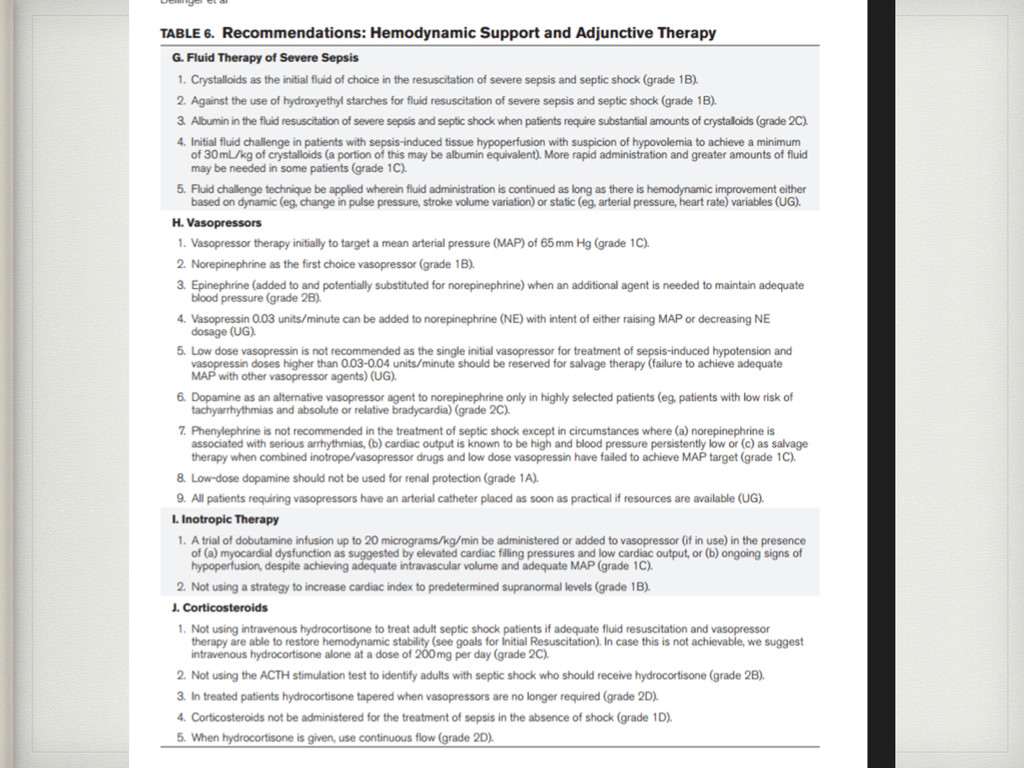
vasopressors (for hypotension that does not respond to initial fluid resuscitation) to maintain a mean arterial pressure (MAP) ≥65mmHg • 6. In the event of persistent hypotension after initial fluid administration (MAP < 65 mm Hg) or if initial lactate was ≥4 mmol/L, re-assess volume status and tissue perfusion and document findings according to Table 1. • 7. Re-measure lactate if initial lactate elevated.
Repeat focused exam (after initial fluid resuscitation) by licensed independent practitioner including vital signs, cardiopulmonary, capillary refill, pulse, and skin findings. • OR TWO OF THE FOLLOWING: Measure CVP Measure ScvO2 Bedside cardiovascular ultrasound Dynamic assessment of fluid responsiveness with passive leg raise or fluid challenge
Risk Factors and Outcome of Severe Sepsis and Septic Shock in Adults: A Multicentre Prospective Study in Intensive Care Units JAMA: 274(12), 27 Sept, 1995 •Peake S, for the ARISE Investigators: The outcome of sepsis and septic shock presenting to the Emergency Department in Australia and New Zealand. Critical Care 2007, 11(Suppl 2):P73 •Angus DC et al: Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome, and associated costs of care. Crit Care Med 29:1303, 2001 •Armstrong PW et al., JAMA, 2007;297:43–51 •Clemet N, SJTREM 28:18 2010 • Rockall TA BMJ. 311(6999):222- 6, 1995 July 22 •Mitchell M et al Crit Care Med 2010 Vol. 38, No. 2 •Hamdy O, Sep 2009 •Dellinger RP, Levy MM, Rhodes A, et al: Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013; 41:580-637
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}