This is the third of five lectures for my MCAT review course at Saint Louis University. More details are available at https://chris-prener.github.io/mcat
https://chris-prener.github.io/mcat ▸ Contact at [email protected] ▸ Plan to take a quick break around 7pmI am not a Psychologist or a Psychiatrist! ▸ We’ll do Chapter 3 today and Chapters 4 & 5 during session 3 on March 28th (6pm to 8pm)
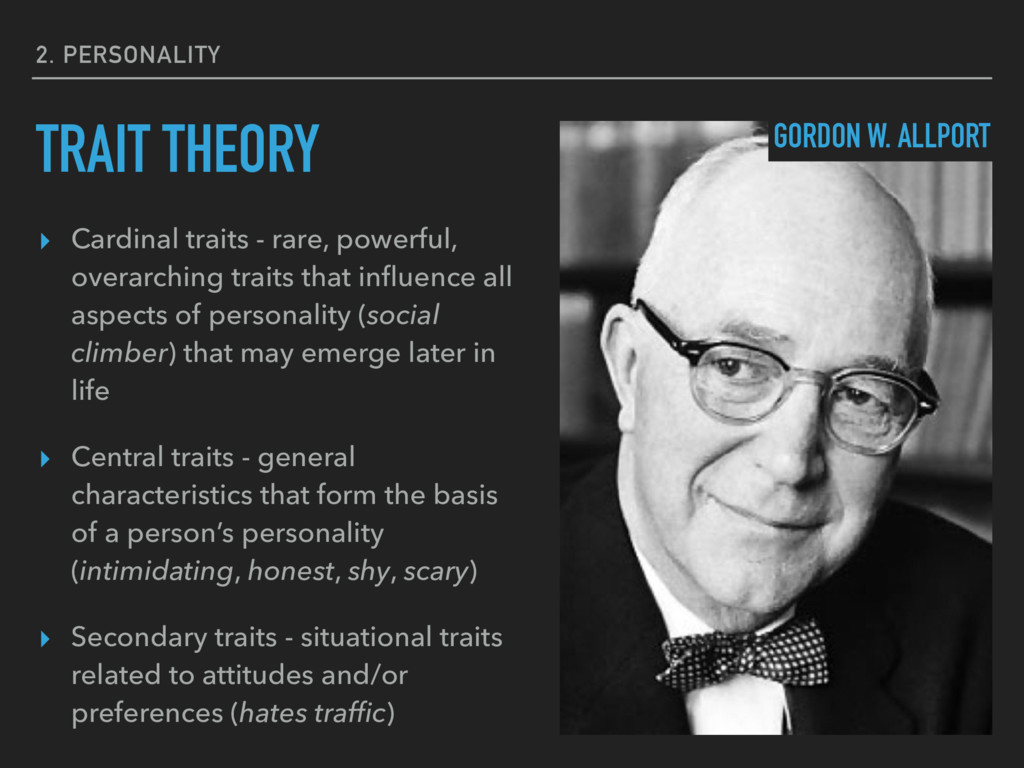
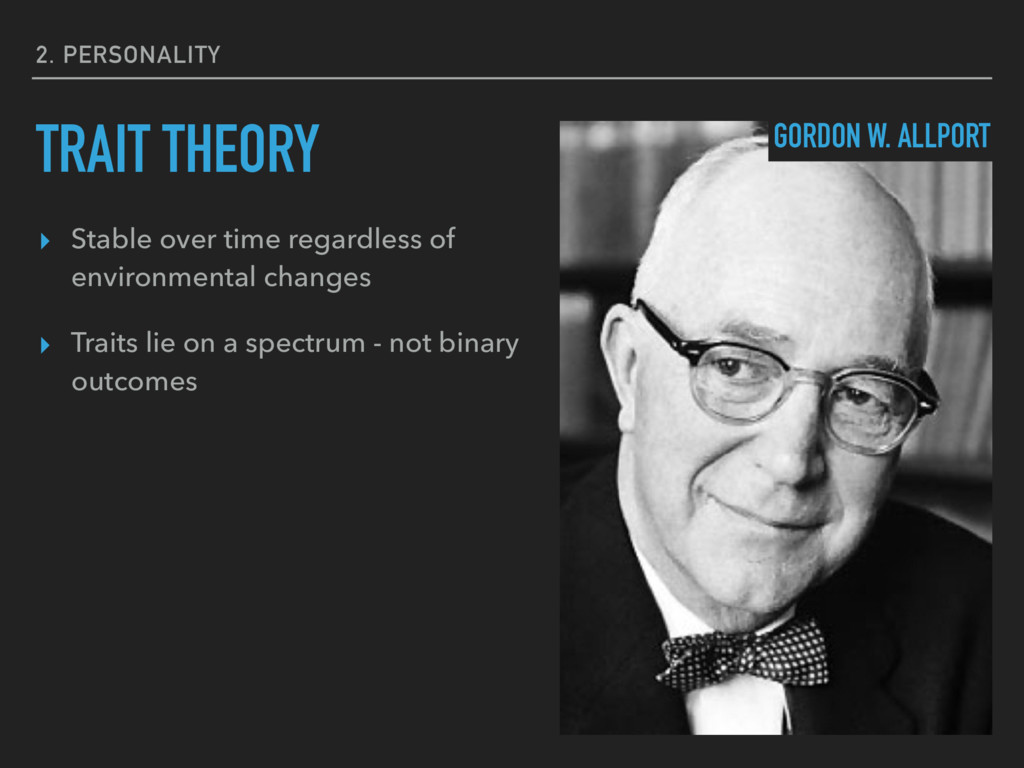
that influence all aspects of personality (social climber) that may emerge later in life ▸ Central traits - general characteristics that form the basis of a person’s personality (intimidating, honest, shy, scary) ▸ Secondary traits - situational traits related to attitudes and/or preferences (hates traffic) TRAIT THEORY GORDON W. ALLPORT
present from birth ▸ Superego - develops later in life through socialization ▸ Ego - directs behavior in a way that balances the drives of the id and the superego ▸ This process takes place outside of conscious awareness PSYCHOANALYTIC THEORY SIGMUND FREUD
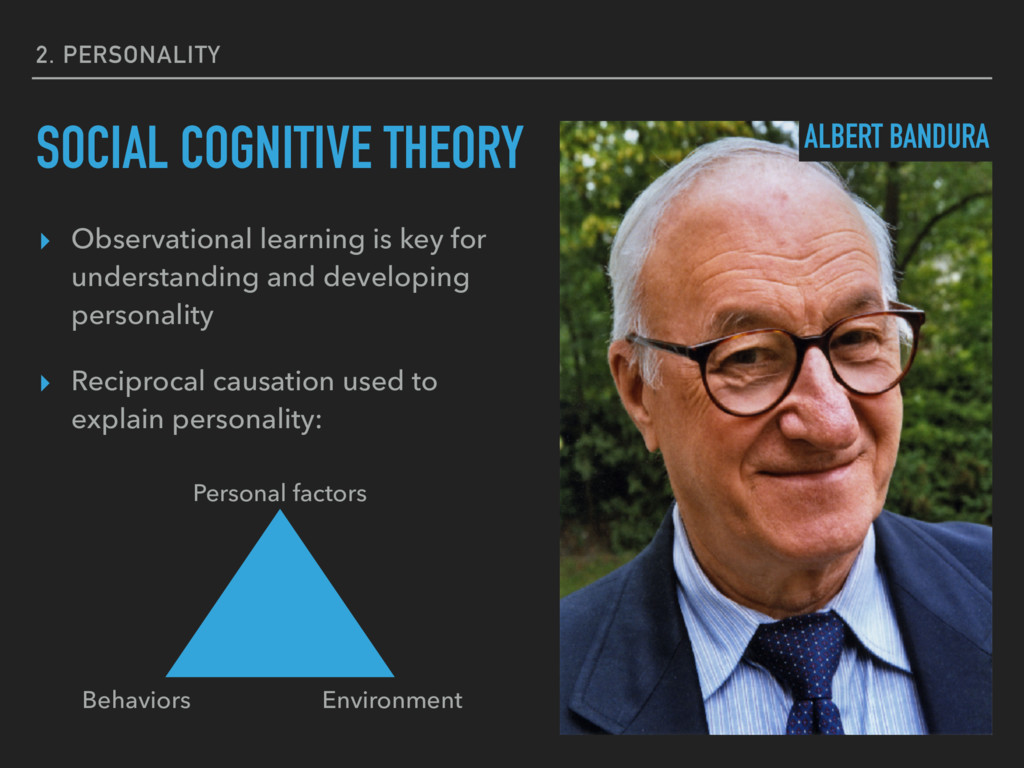
developing personality ▸ Reciprocal causation used to explain personality: SOCIAL COGNITIVE THEORY ALBERT BANDURA Personal factors Behaviors Environment
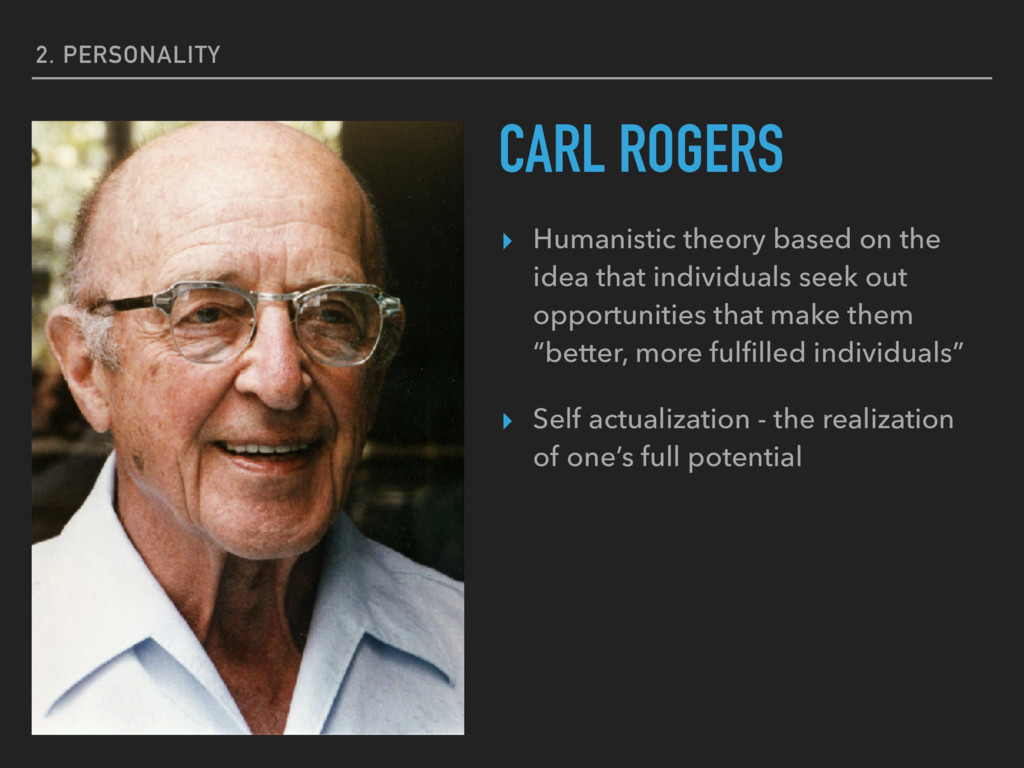
individuals seek out opportunities that make them “better, more fulfilled individuals” ▸ Self actualization - the realization of one’s full potential CARL ROGERS
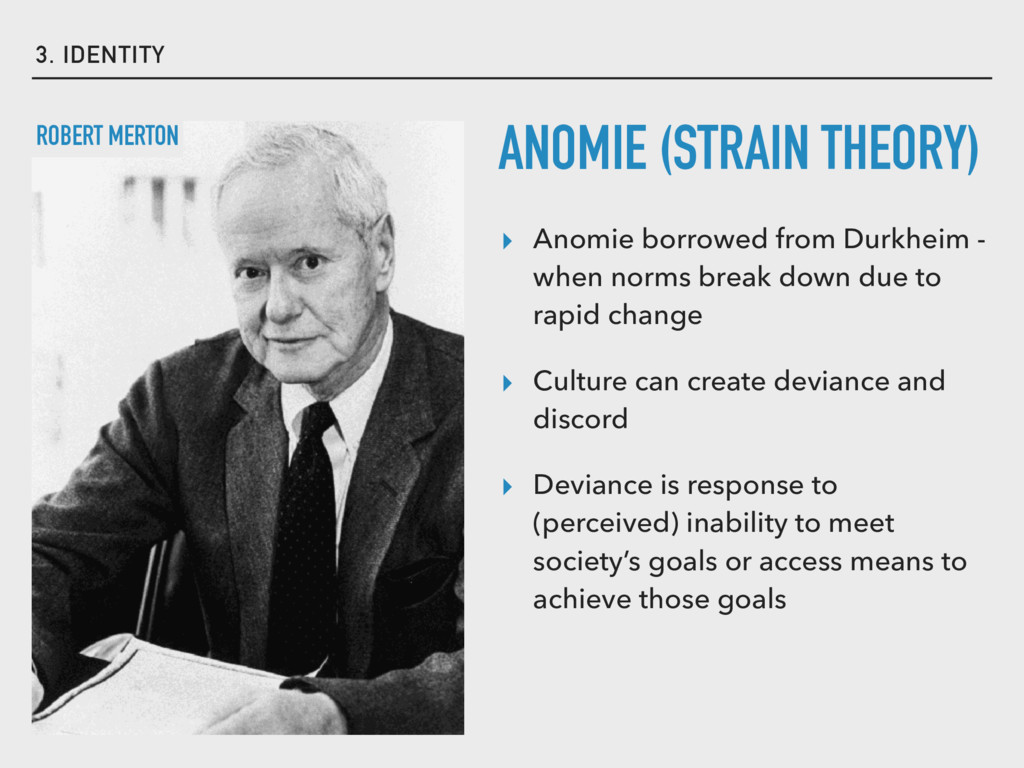
break down due to rapid change ▸ Culture can create deviance and discord ▸ Deviance is response to (perceived) inability to meet society’s goals or access means to achieve those goals ANOMIE (STRAIN THEORY) ROBERT MERTON
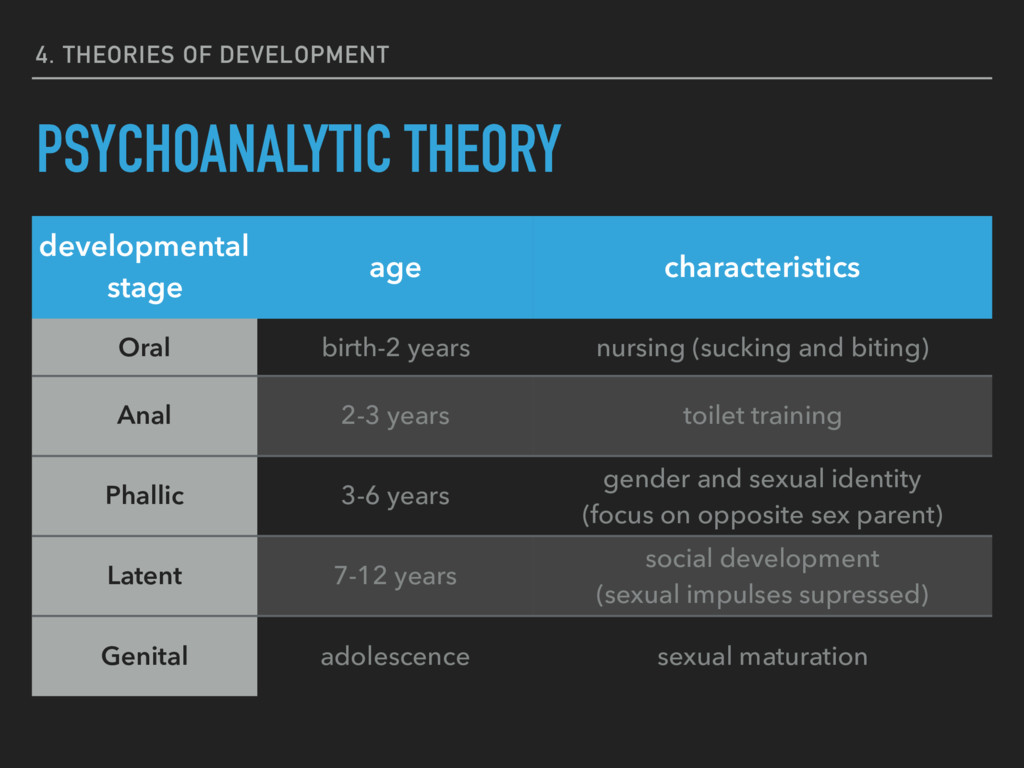
Oral birth-2 years nursing (sucking and biting) Anal 2-3 years toilet training Phallic 3-6 years gender and sexual identity (focus on opposite sex parent) Latent 7-12 years social development (sexual impulses supressed) Genital adolescence sexual maturation
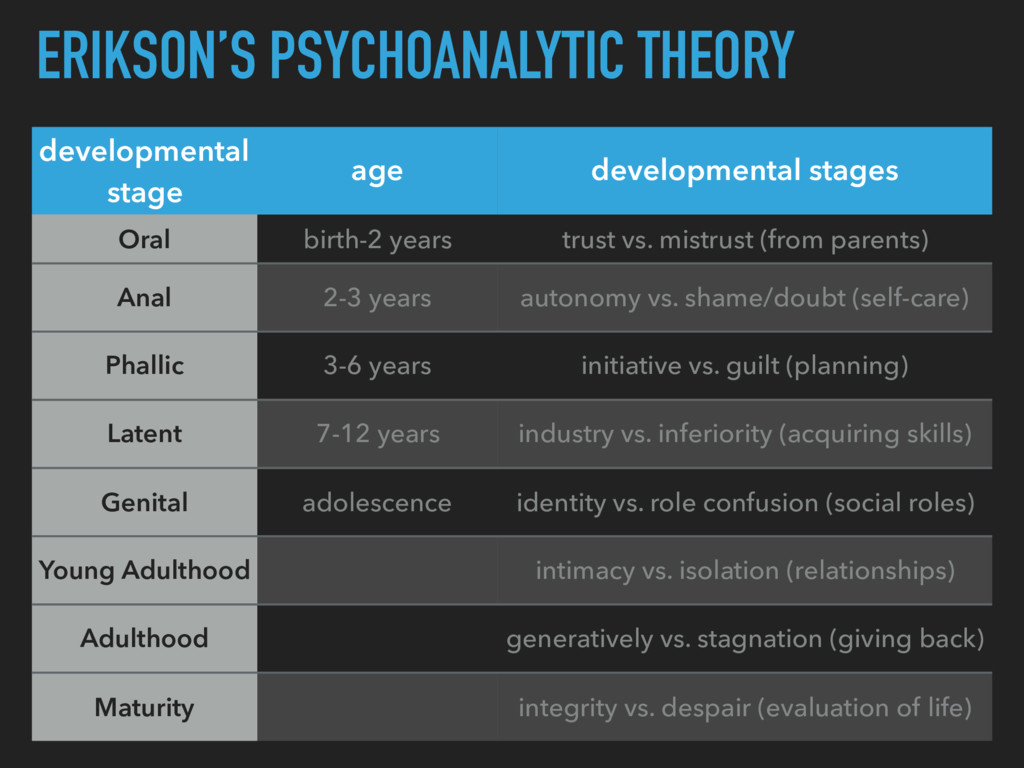
years trust vs. mistrust (from parents) Anal 2-3 years autonomy vs. shame/doubt (self-care) Phallic 3-6 years initiative vs. guilt (planning) Latent 7-12 years industry vs. inferiority (acquiring skills) Genital adolescence identity vs. role confusion (social roles) Young Adulthood intimacy vs. isolation (relationships) Adulthood generatively vs. stagnation (giving back) Maturity integrity vs. despair (evaluation of life)
INTO THIS COUNTRY, SHE NEEDS TO LEAVE HER TOWEL HOME. BECAUSE THE REASON THIS COUNTRY IS HERE AND SAFE TODAY IS BECAUSE OF JESUS CHRIST…WE WERE ONE NATION UNDER GOD. THE MUSLIMS ARE INTO ALLAH. THEY CAN'T LIVE THERE [IN THEIR HOME COUNTRIES] ANYMORE BECAUSE OF ALL THE TURMOIL AND UNREST. HERE WE STILL HAVE SOMEWHAT PEACE. Bill Jackson, Elizabethtown, NY
PEACE, FOLLOW OUR RULES AND BE ONE NATION UNDER GOD. OR STAY HOME. I'M NOT MAKING YOU CHANGE YOUR RELIGION, OR WHATEVER YOU WANT TO CALL IT, YOUR BELIEF. BUT IF YOU WANT THIS, WHAT WE WANT, THEN YOU GOT TO DO WHAT WE'RE DOING TO GET IT. Bill Jackson, Elizabethtown, NY
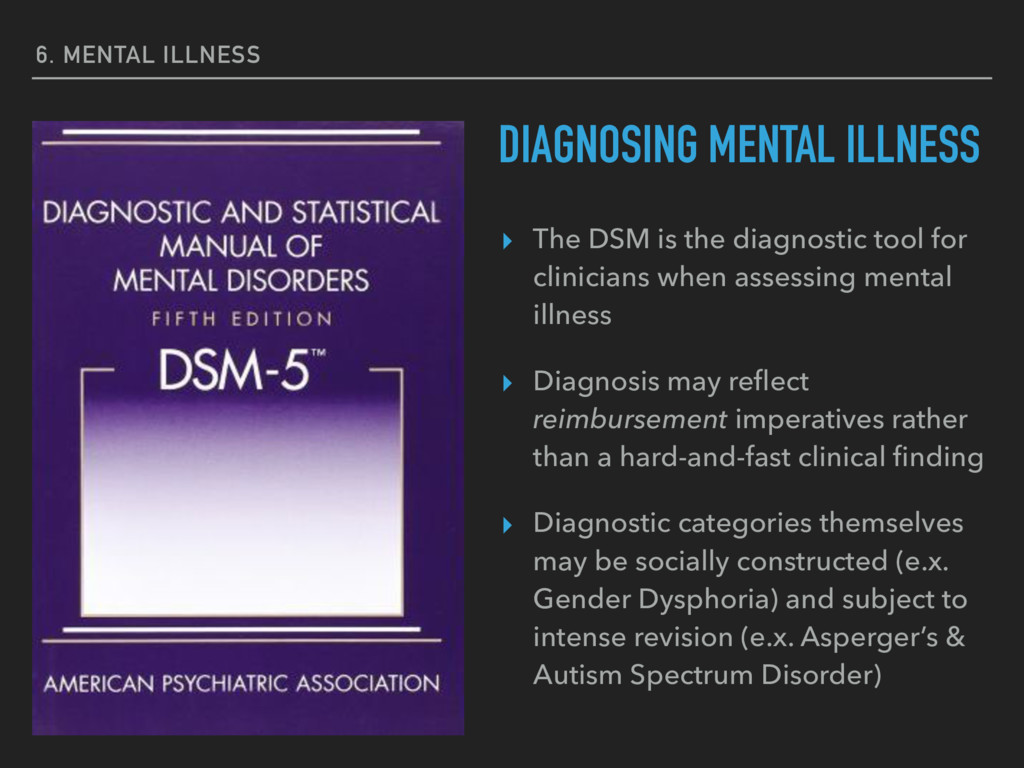
for clinicians when assessing mental illness ▸ Diagnosis may reflect reimbursement imperatives rather than a hard-and-fast clinical finding ▸ Diagnostic categories themselves may be socially constructed (e.x. Gender Dysphoria) and subject to intense revision (e.x. Asperger’s & Autism Spectrum Disorder) DIAGNOSING MENTAL ILLNESS
(pain, fatigue, motor problems) that lead to substantial, functional psychological impairment ▸ Emphasis placed on the patient’s experience regardless of the underlying biological nature of the physical symptoms ▸ Up to 20% of primary care patients have symptoms that fit DSM criteria for diagnosis ▸ Diagnostic categories have been contested ▸ Diagnoses include Somatic Symptom Disorder, Illness Anxiety Disorder, Conversion Disorder, and Facitious Disorder
to the future or hypothetical scenarios (and thus considered unwarranted) ▸ Characterized by both physical and emotional experiences of anxiety ▸ Broader category (including PTSD) is most diagnosed category of illnesses in the U.S. ▸ 15% of U.S. population likely to experience an anxiety disorder during their lifetime with 10% experiencing symptoms each year ▸ Diagnoses include Generalized Anxiety Disorder, Panic Disorder, and specific phobias
to any life threatening or traumatic event ▸ Can also include third-party exposure ▸ Symptoms include re-experiencing the event, hallucinations, and disrupted sleep ▸ Lifetime prevalence of approximately 6-7% in the population, with women several times more likely to experience PTSD ▸ High prevalence among veterans (14% among OIF/OEF; 30% for Vietnam veterans) ▸ There is also an Acute Stress Disorder for symptoms (including dissociative symptoms like numbing) immediately occurring but receding within a month
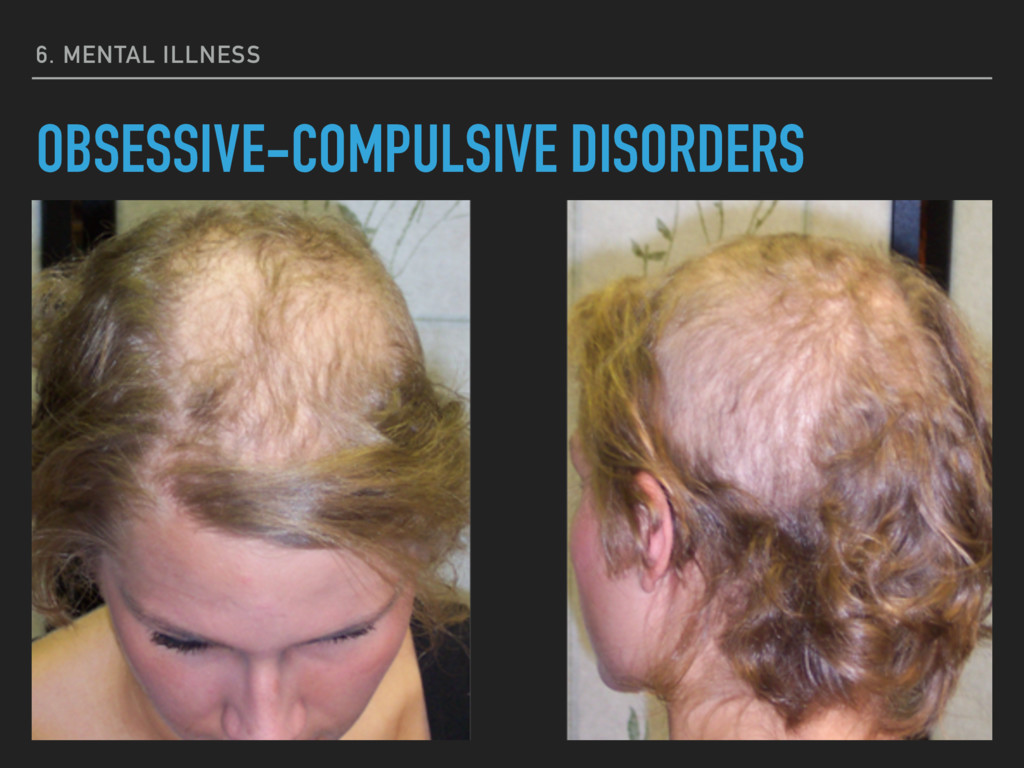
and compulsive (ritualistic behavior) behaviors that impede daily functioning ▸ Low prevalence - only 1% of adult U.S. population experiences this in a given year with a lifetime prevalence of 1.6%. ▸ Specific diagnoses include Body Dysmorphic Disorder, Hoarding Disorder, Trichotillomania, and Excoriation Disorder.
(depression) and/or extreme excitement (mania), or the oscillation between the two ▸ Depressive disorders are characterized by persistent depression that may be severe ▸ Persistent but less severe symptoms may be diagnosed as Persistent Depressive Disorder while severe symptoms may be diagnosed as Major Depressive Disorder. ▸ Roughly 7% of U.S. adults experience major depressive episodes each year with women twice as likely to experience these symptoms
heritability and may have etiological roots in neurological disruption ▸ Successful treatment using monoamine inhibitors and selective serotonin re-uptake inhibitors has led to hypothesis about these roots ▸ Bipolar disorders are characterized by mania that is disruptive for at least a week at a time (Bipolar I) or is less disruptive and does not cause severe impairment (Bipolar II). ▸ Bipolar disorders may also have symptoms associated with psychotic disorders (including delusions and hallucinations) ▸ Lifetime prevalence for bipolar disorders is about 4%
an experience of hallucinations, delusions, and disorganized speech ▸ Some evidence of heritability (with consequences for how we treat children with risk of developing the disease) ▸ Synaptic pruning (shedding of weak or redundant neurological connections) that is accelerated or intensified during young adulthood are at a higher risk for schizophrenia ▸ Estimates of lifetime prevalence are 0.5% to 1.0%; about 2 million Americans have the illness
in psychological functioning - disruption in memory, identity, or consciousness ▸ Prevalence of less than 1% in the population ▸ Diagnoses include Depersonalization/derealization disorder and dissociative identity disorder (very contested)
personality traits that inhibit social functioning - can include instability in moods, attitude, behavior, and self image ▸ Diagnoses are contested and there is criticism about the way these disorders are categorized and labeled ▸ Lifetime prevalence is 9%, women are more likely to receive a diagnosis than men ▸ Diagnoses include Antisocial Personality Disorder, Avoidant Personality Disorder, and Borderline Personality Disorder
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![ATTRIBUTION ERROR “Automatically [favoring] dispositional attributions over situational ones when](https://files.speakerdeck.com/presentations/f02becccdf974a959c6299786dabca00/slide_70.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}