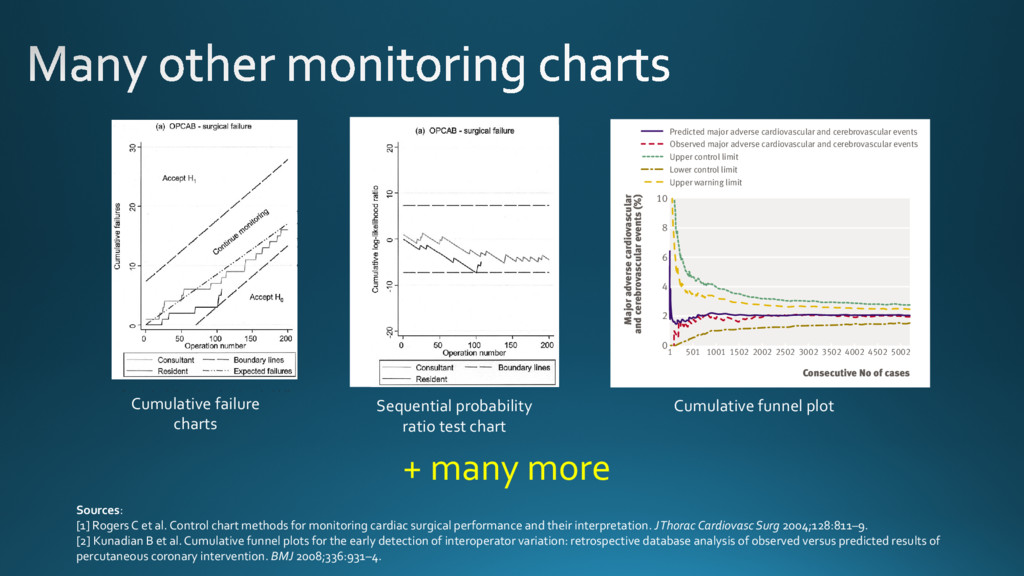
operations needed graph is more intuitive because it is easier to identify changes in Figure 1. Cumulative failure charts for (a) surgical failure after off-pump CABG (OPCAB) and (b) 30-day mortality after orthotopic heart transplantation in adults. Expected failure rates (p 0 ) were set at overall failure rates for the programs as a whole: (a) 8.5% for 1 consultant and 4 residents and (b) 12% for 8 centers. Boundary lines were constructed to detect a 50% increase in failures (odds ratio, 1.5): (a) 3.7% (p 1 ؍ 12.2%) and (b) 5.0% (p 1 ؍ 17.0%). False-positive (␣) and false-negative () error rates are 5% for both charts. Lines representing expected cumulative failures (— · · ) are shown in both charts, although these are not usually included. In (a), which depicts the consultant and 1 of the 4 residents, the consultant’s failure rate is similar to the overall failure rate (closely follows the — · · line), but is less than expected for the resident. The resident’s performance was confirmed as acceptable (or better) after 100 operations, when the lower boundary line was reached. In (b), which depicts 2 of the 8 transplant centers, performance at center A was consistently better than expected and was confirmed to be acceptable or better after 80 transplantations. Performance at center B was in line with overall mortality for the first 100 transplantations, but increased steadily thereafter. By transplantation 167, center B was close to the 5% upper boundary, having already crossed the 10% upper boundary (not shown). Rogers et al Statistics for the Rest of Us STATISTICS However, plotting boundary lines to detect deviations from accept- able performance is more intuitive with cumulative failures or cumulative log-likelihood ratio charts. Therefore, we consider the two types of chart to be complementary. A line with a gradient corresponding to the acceptable (ex- pected) failure rate could be added to cumulative failure charts, but VLAD or CRAM chart. The graph, which starts at 0, is incre- mented by 1 Ϫ p 0i for a failure and is decremented by p 0i for a success, where p 0i denotes the predicted probability of failure for operation i, derived from the appropriate risk model (Figure 4). The graph has a natural interpretation: it moves upward if the failure rate increases above that predicted by the risk model, moves Figure 2. Cumulative log-likelihood ratio test charts for (a) surgical failure after off-pump CABG (OPCAB) and (b) 30-day mortality after orthotopic heart transplantation in adults. Data and parameter settings for constructing boundary lines (p 0 , p 1 , ␣, and ) are the same as for Figure 1. Lines representing expected cumulative failures have not been included; note that such lines, if included, would not be horizontal through 0 but would slope downward from 0 toward the lower boundary, which denotes acceptance of H 0 . These figures provide an alternative representation of the data shown in Figure 1. Interpretation of the graphs in relation to the boundary lines is the same. The points at which the graphs for the resident and center A cross the lower acceptance boundary coincide with Figure 1. Statistics for the Rest of Us Rogers et al STATISTICS Cumulative failure charts Sequential probability ratio test chart tive data that will serve to improve the quality of health care. Although comparative performance of UK cardiac surgeons has been published in the public arena,15 operator specific data for percutaneous cor- onary intervention are not yet available. The task force of the American College of Cardio- logy and American Heart Association has recently published recommendations for standards to assess operator proficiency and institutional programme quality.16 We address these recommendations and provide a method to implement them in a UK setting. We used the north west quality improvement pro- gramme risk model and then used cumulative funnels and funnel plots to display the observed major adverse cardiovascular and cerebrovascular events against the predicted rate of these events. Comparative perfor- mance of UK cardiac surgeons has been disseminated using these plots.17 In cardiology, funnel plots have been used to interpret the dataset of the myocardial infarction national audit project (a UK cardiology dataset that provides specific performance tables).18 Weaimedtoshowthatoperatorspecificoutcomesafter percutaneous coronary intervention can be monitored successfully using funnel plots and cumulative funnel plots. METHODS A detailed database of clinical, procedural, and angiographic variables has been maintained on all patients undergoing percutaneous coronary inter- vention in our unit since 1994. The dataset is based on the British Cardiovascular Intervention Society national dataset,19 with several additional data ele- ments. The prospective acquisition of data is accom- plished by immediate input from the operators after enzyme levels but is not required in the national dataset. We considered Q wave myocardial infarction occurring in the context of angioplasty therapy for acute ST elevation myocardial infarction to be an outcome of the original coronary event and not a complication of percutaneous coronary intervention. Consecutive No of cases Major adverse cardiovascular and cerebrovascular events (%) 1 501 1001 1502 2002 2502 3002 3502 4002 4502 5002 r adverse cardiovascular rebrovascular events (%) 4 6 8 10 0 2 4 6 8 10 Predicted major adverse cardiovascular and cerebrovascular events Observed major adverse cardiovascular and cerebrovascular events Upper control limit Lower control limit Upper warning limit Predicted major adverse cardiovascular and cerebrovascular events Observed major adverse cardiovascular and cerebrovascular events Upper control limit Lower control limit Upper warning limit Cumulative funnel plot Sources: [1] Rogers C et al. Control chart methods for monitoring cardiac surgical performance and their interpretation. J Thorac Cardiovasc Surg 2004;128:811–9. [2] Kunadian B et al. Cumulative funnel plots for the early detection of interoperator variation: retrospective database analysis of observed versus predicted results of percutaneous coronary intervention. BMJ 2008;336:931–4. + many more
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![4,920 valve operations from 1997 to 2004 [9]. Subse- quently,](https://files.speakerdeck.com/presentations/6290fd4cd5734604aa7aa351a77053d7/slide_9.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}