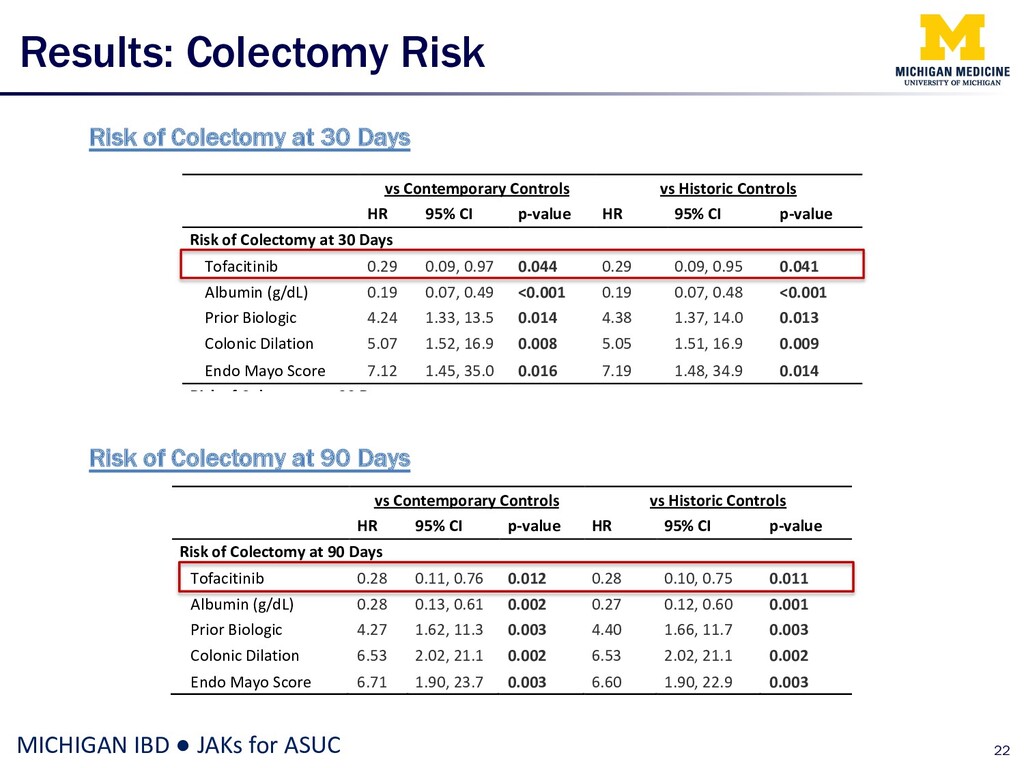
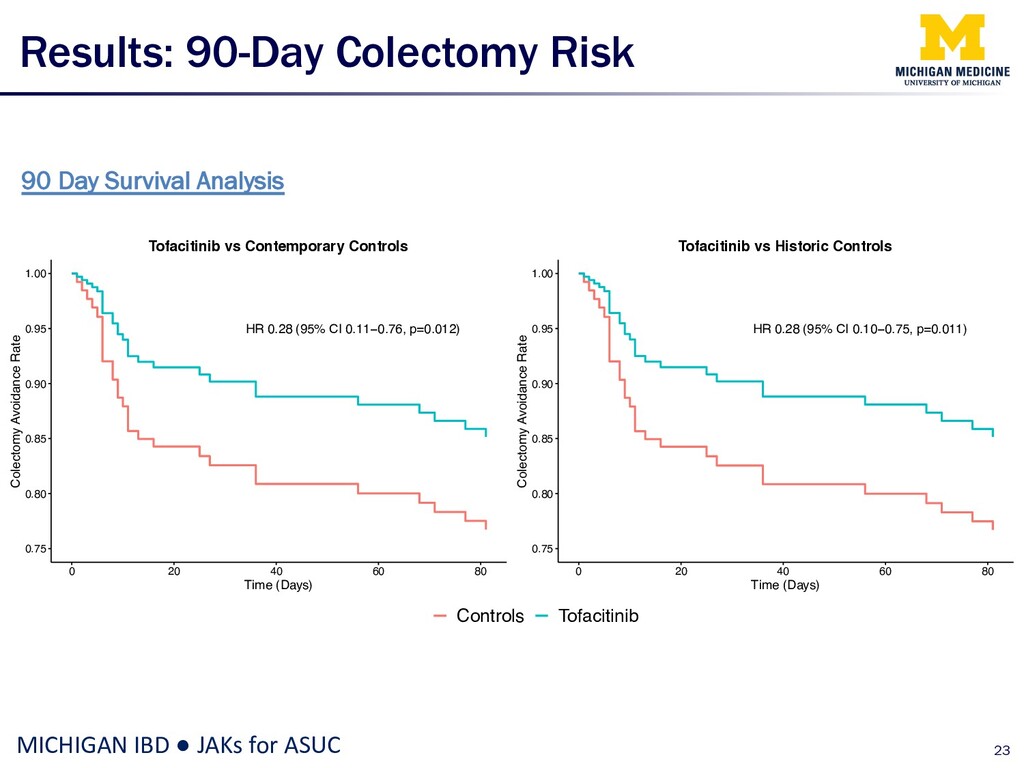
Risk of Colectomy at 30 Days Risk of Colectomy at 90 Days vs Contemporary Controls vs Historic Controls HR 95% CI p-value HR 95% CI p-value Risk of Colectomy at 30 Days Tofacitinib 0.29 0.09, 0.97 0.044 0.29 0.09, 0.95 0.041 Albumin (g/dL) 0.19 0.07, 0.49 <0.001 0.19 0.07, 0.48 <0.001 Prior Biologic 4.24 1.33, 13.5 0.014 4.38 1.37, 14.0 0.013 Colonic Dilation 5.07 1.52, 16.9 0.008 5.05 1.51, 16.9 0.009 Endo Mayo Score 7.12 1.45, 35.0 0.016 7.19 1.48, 34.9 0.014 Risk of Colectomy at 90 Days Tofacitinib 0.28 0.11, 0.76 0.012 0.28 0.10, 0.75 0.011 Albumin (g/dL) 0.28 0.13, 0.61 0.002 0.27 0.12, 0.60 0.001 Prior Biologic 4.27 1.62, 11.3 0.003 4.40 1.66, 11.7 0.003 Colonic Dilation 6.53 2.02, 21.1 0.002 6.53 2.02, 21.1 0.002 Endo Mayo Score 6.71 1.90, 23.7 0.003 6.60 1.90, 22.9 0.003 vs Contemporary Controls vs Historic Controls HR 95% CI p-value HR 95% CI p-value Risk of Colectomy at 90 Days Tofacitinib 0.28 0.11, 0.76 0.012 0.28 0.10, 0.75 0.011 Albumin (g/dL) 0.28 0.13, 0.61 0.002 0.27 0.12, 0.60 0.001 Prior Biologic 4.27 1.62, 11.3 0.003 4.40 1.66, 11.7 0.003 Colonic Dilation 6.53 2.02, 21.1 0.002 6.53 2.02, 21.1 0.002 Endo Mayo Score 6.71 1.90, 23.7 0.003 6.60 1.90, 22.9 0.003
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}