Presented at the 3rd Annual Open Source EHR Summit - Key takeaways:
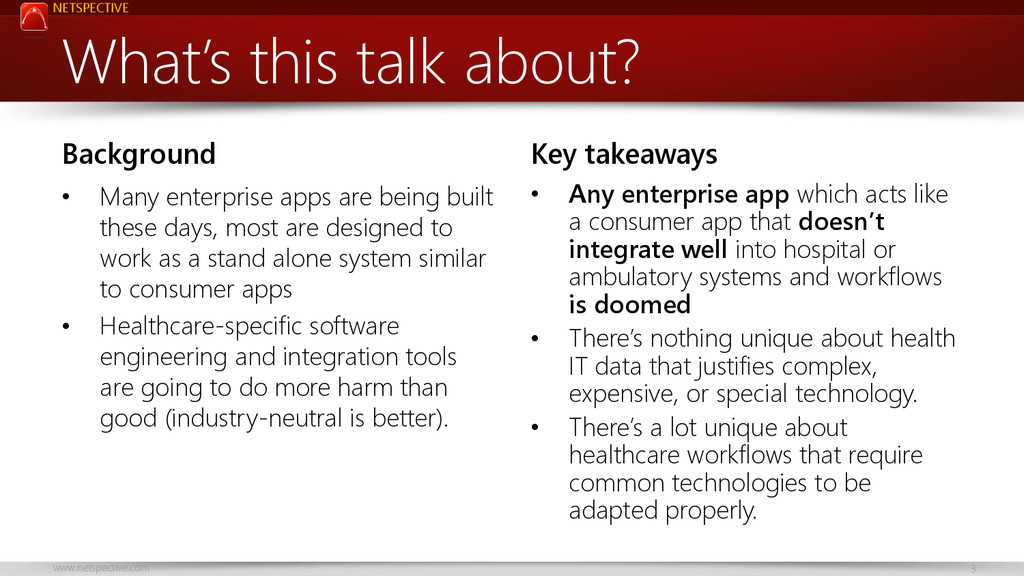
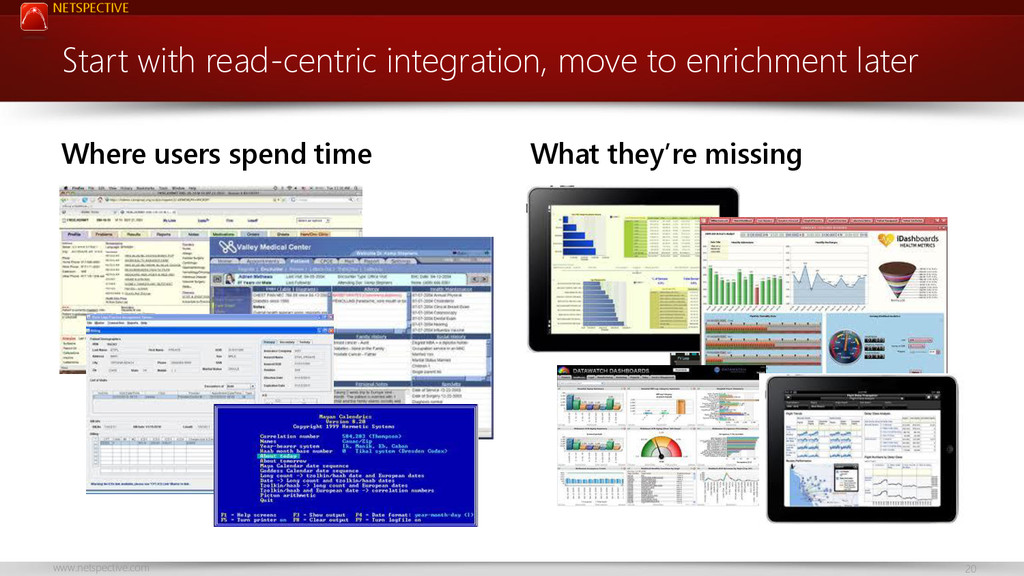
* Any enterprise app which acts like a consumer app that doesn’t integrate well into hospital or ambulatory systems and workflows is doomed
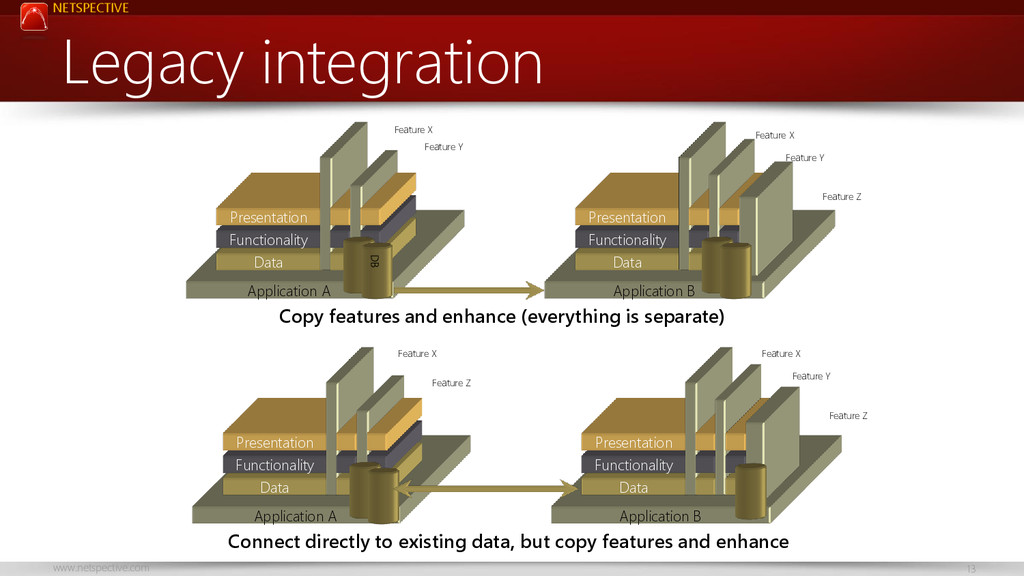
* There’s nothing unique about health IT data that justifies complex, expensive, or special technology.
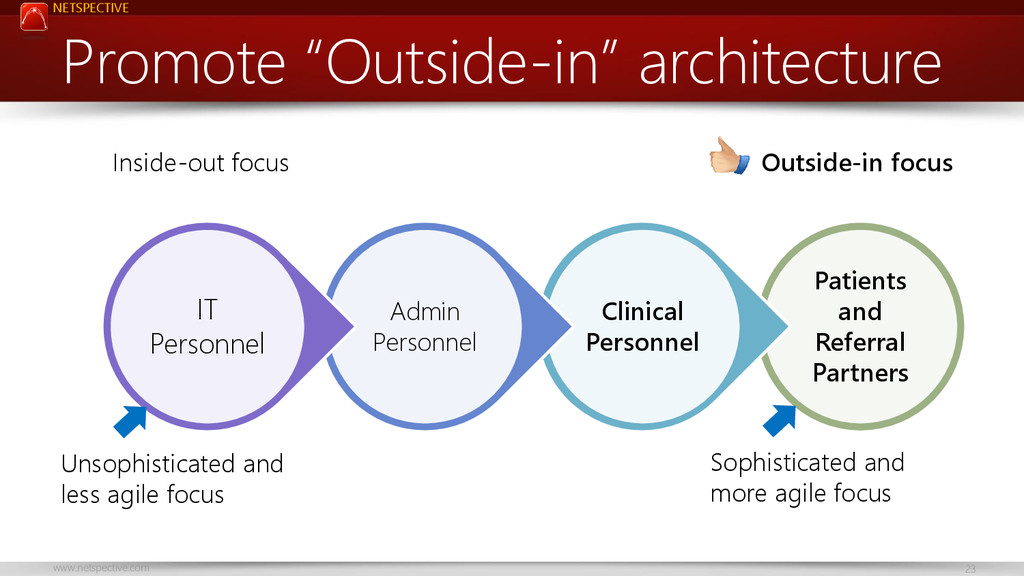
* There’s a lot unique about healthcare workflows that require common technologies to be adapted properly.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Thank You Visit http://www.netspective.com http://www.healthcareguy.com E-mail [email protected] Follow @ShahidNShah Call](https://files.speakerdeck.com/presentations/d2428db018150132d2ab56002d6aedf7/slide_30.jpg){kind=link}