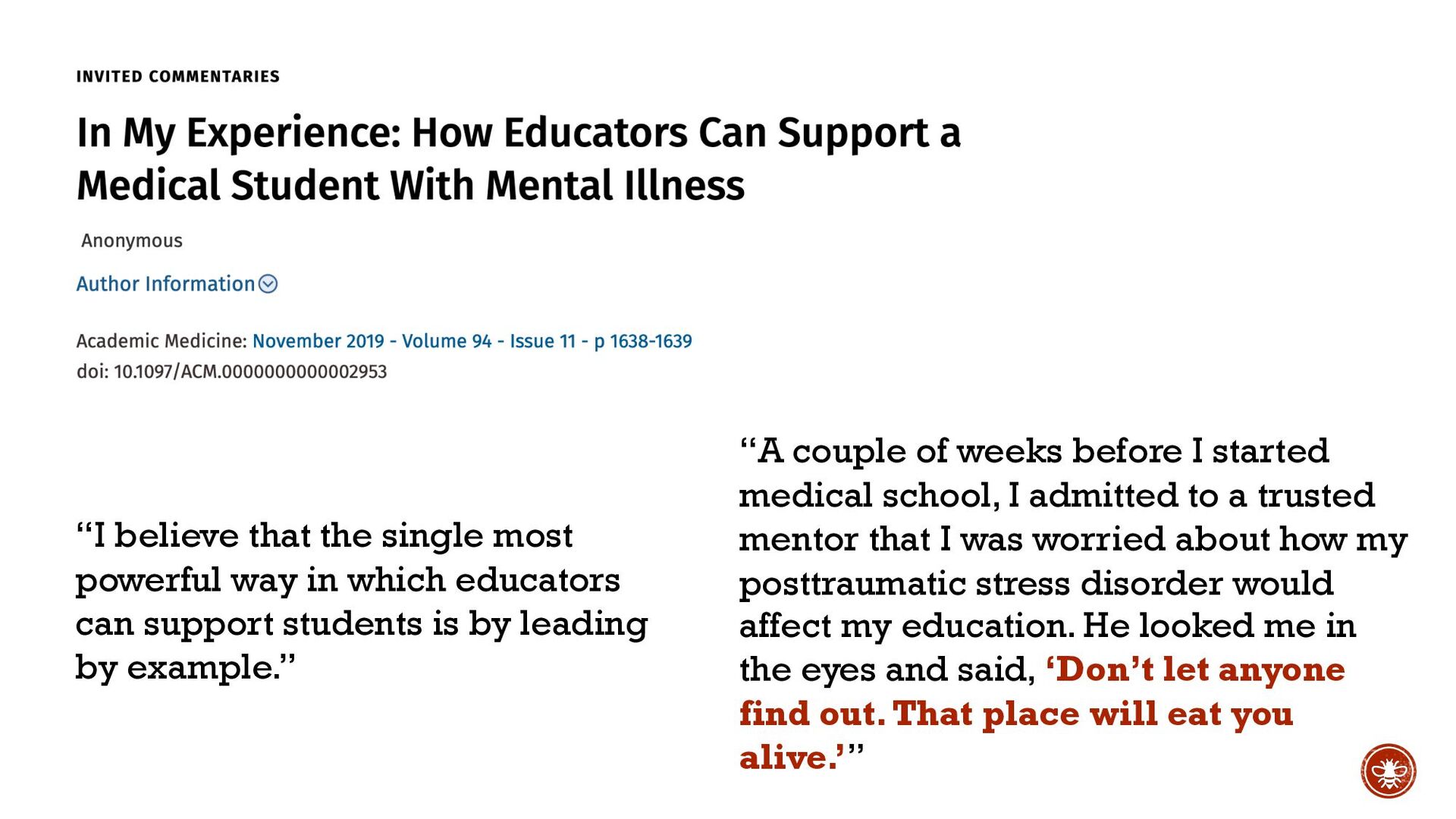
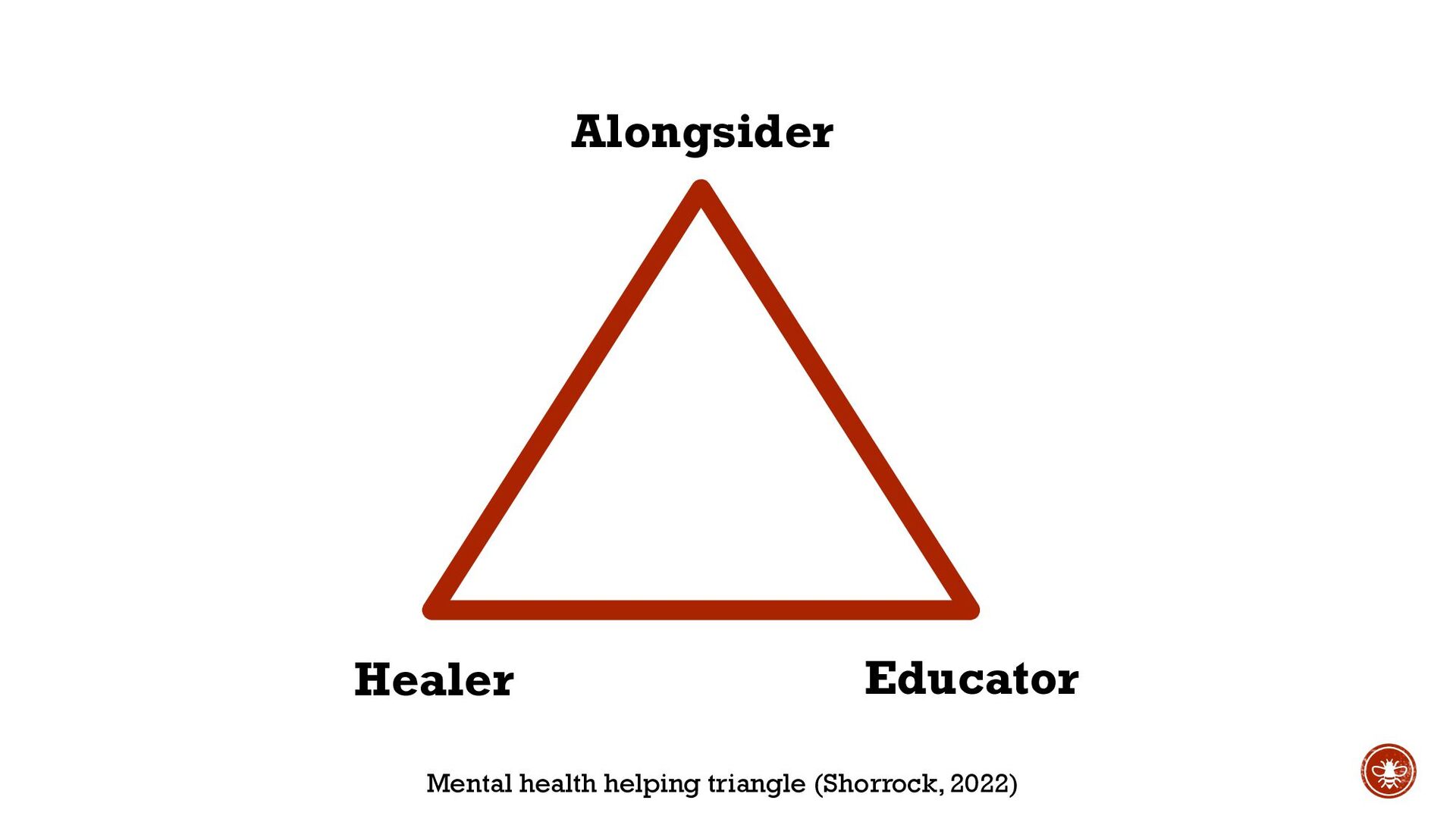
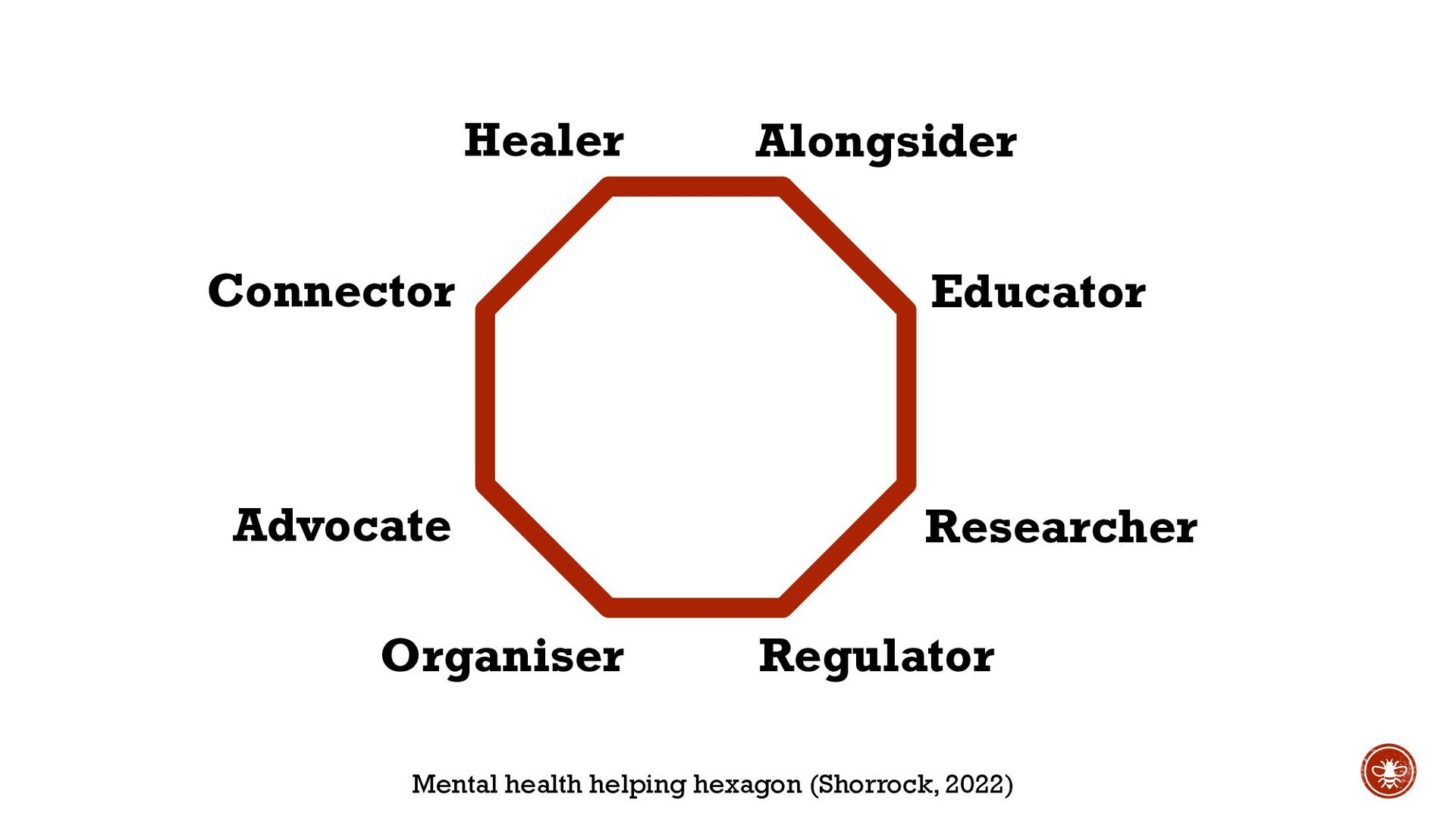
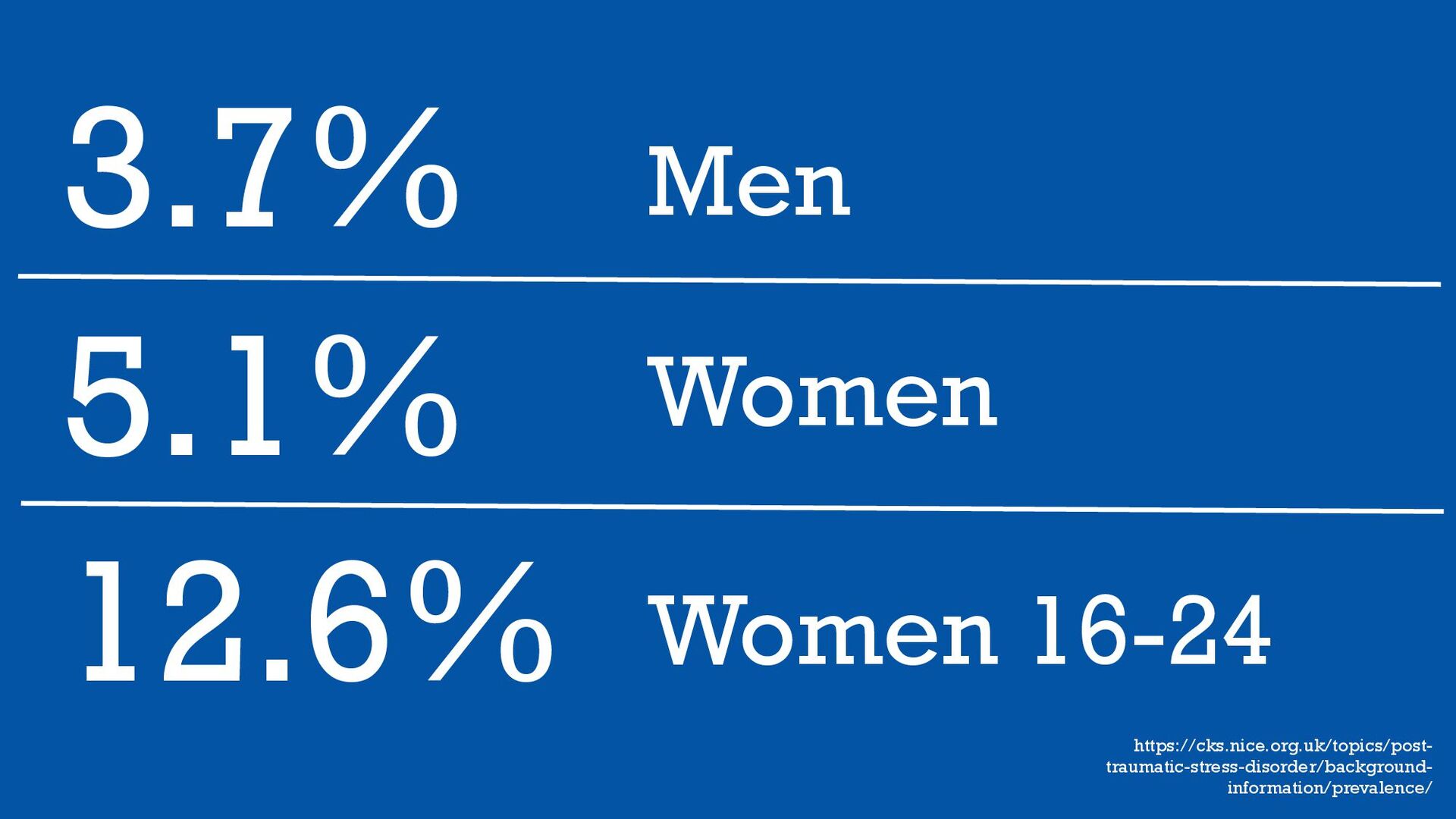
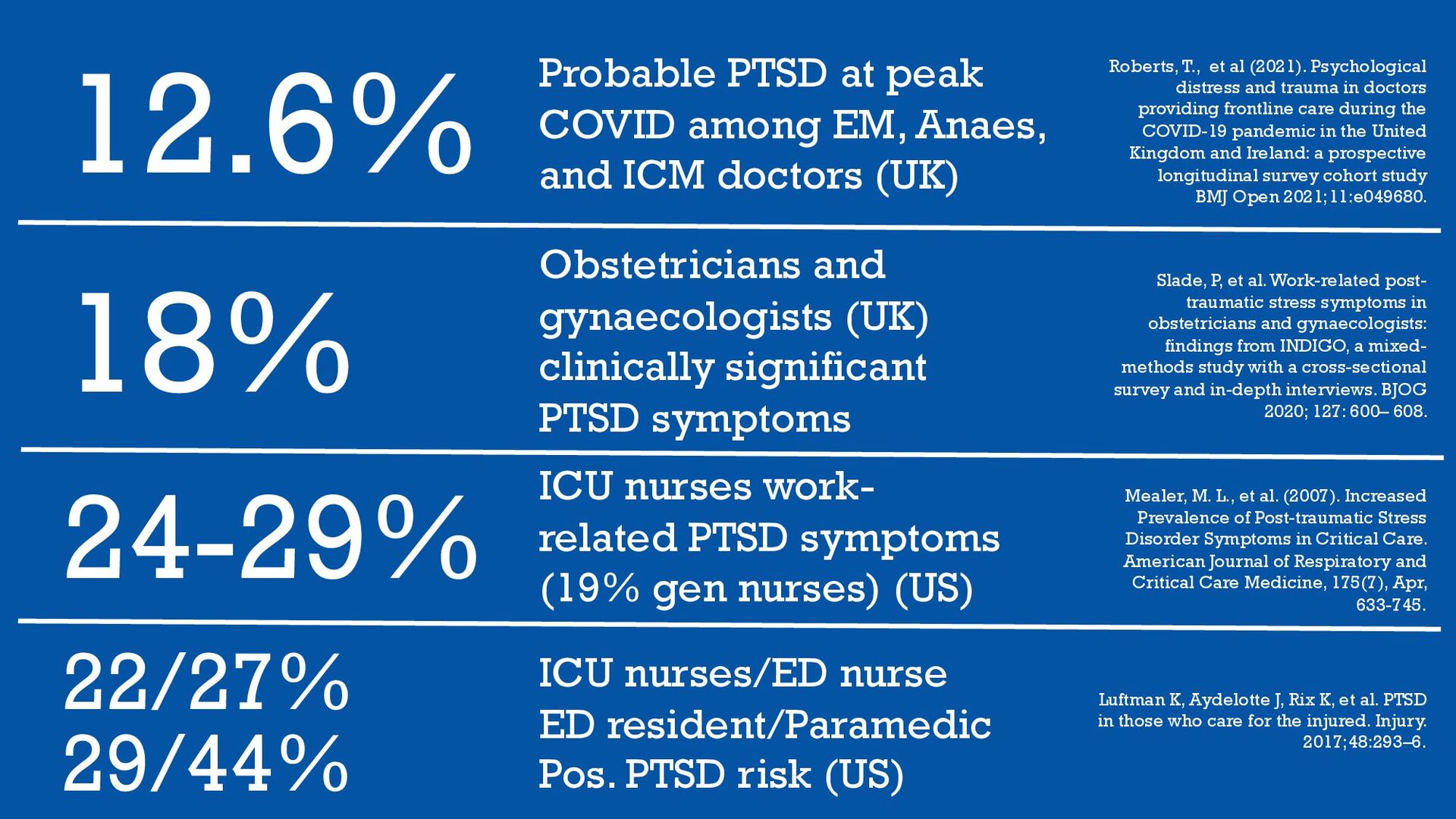
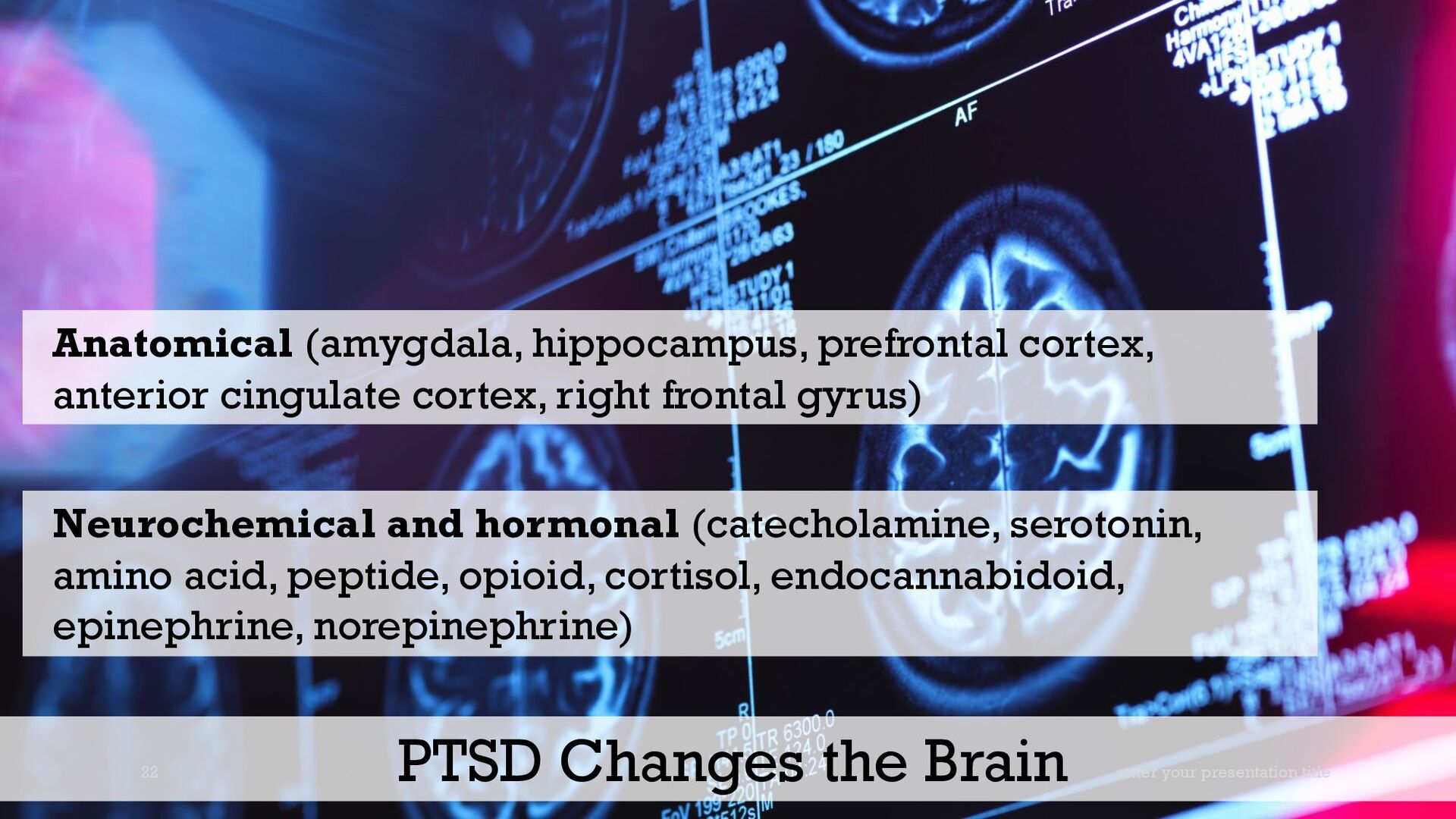
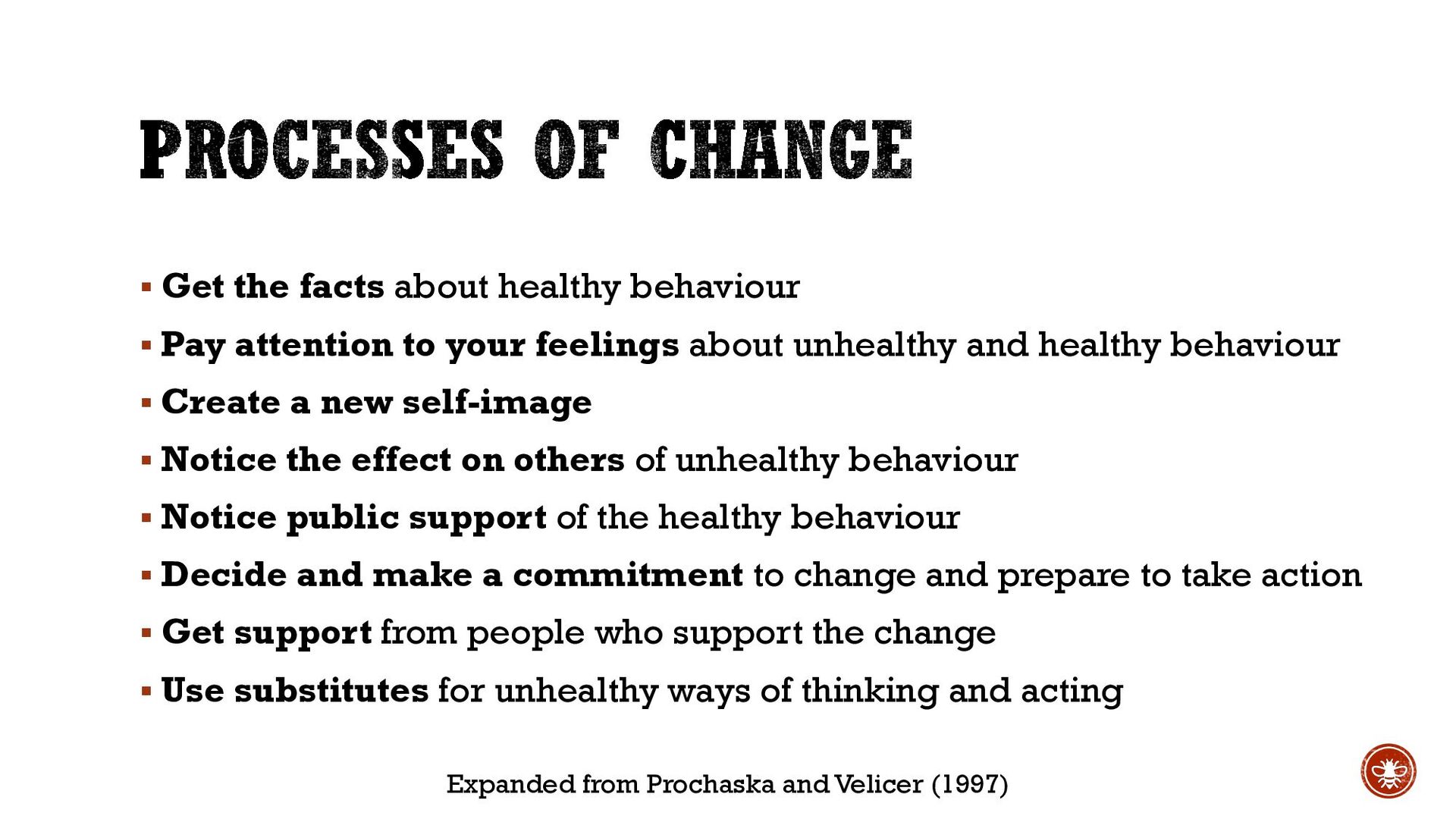
Trauma is at the heart of much mental distress and many problems of living, including those that have their roots in conditions and events at work. But many are unaware of how trauma has impacted their lives, or what to do about it. In some cases, the result can be acquired neurodiversity and hidden disability, requiring changes to work and lifestyle, as well as medical intervention. Dr Steven Shorrock, psychologist and ergonomist working in aviation, shares his personal experience of PTSD and sheds light on what is known about traumatic stress, psychological injury, and recovery, including learning from behaviour change science.
Shorrock, S. (2022, 6-8 November). Invited keynote: We need to talk about trauma. Association for Simulated Practice in Healthcare – ASPiH Conference 2022: All things being equitable. Diversity, inclusivity and simulation, 6-8 November, Birmingham, UK. https://aspih.org.uk/event/conference-2022/
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}