requirements of each person. Everyone has different requirements based on activity and resting energy expenditure (which equals total daily energy expenditure 9900-10,100 kcal/day daily energy expenditure 2500-2600 kcal/day daily energy expenditure
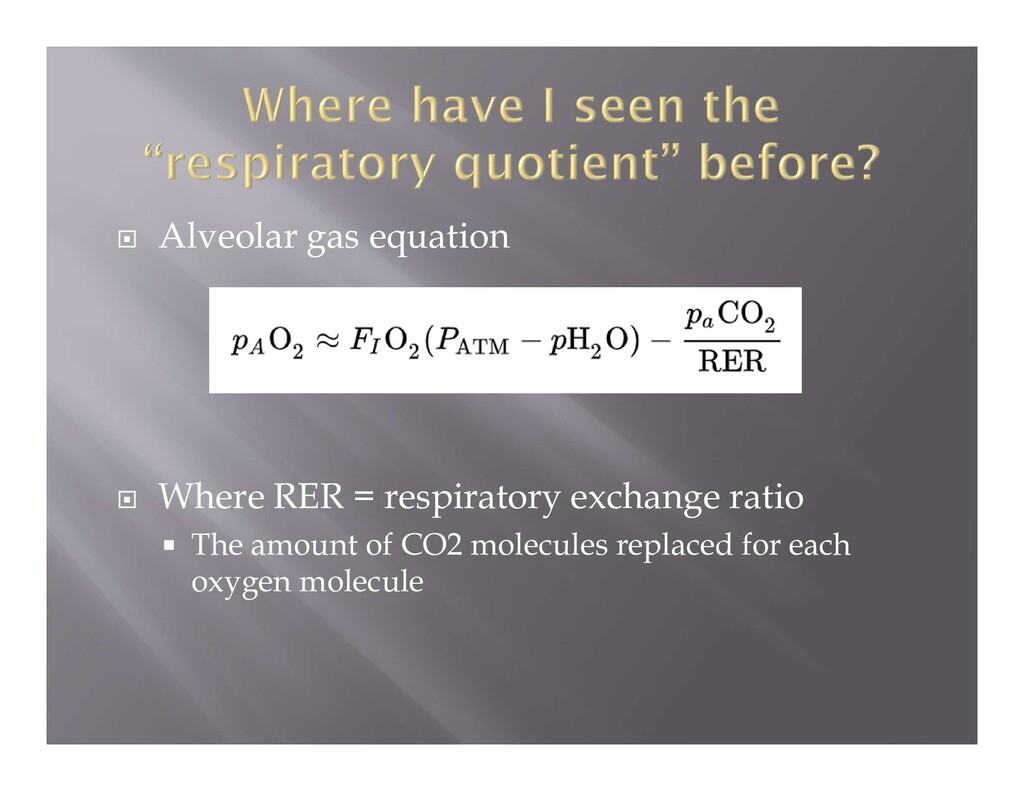
nutrients (proteins, carbohydrates, lipids) This process 1) consumes oxygen 2) produces carbon dioxide 3) produces heat 4) produces water It is not possible to measure heat/water production in hospitalized patients but it is possible to measure oxygen consumption and carbon dioxide production Process to calculate this is called INDIRECT CALORIMETRY
REE (kcal/day) = 25 x body weight (kg) Actual body weight used unless it is 25% higher than ideal body weight in which case adjusted body weight is used Adjusted weight = [(actual – ideal) 0.25] + ideal
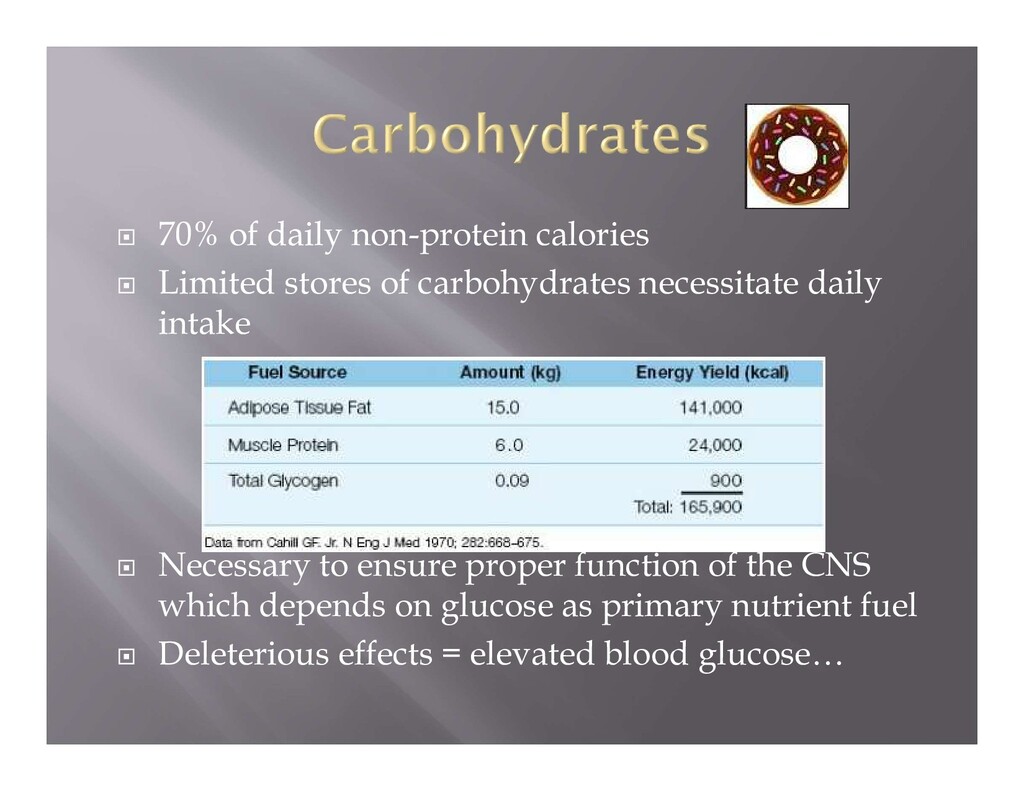
carbohydrates necessitate daily intake Necessary to ensure proper function of the CNS which depends on glucose as primary nutrient fuel Deleterious effects = elevated blood glucose…
whole lectures about lipids…but not going to today Propofol Drug is mixed in a 10% lipid emulsion 1.1 kcal / mL In ICU must factor in infusion into caloric intake
catabolism = more nitrogen excretion) Usual requirement is 0.8-1 g/kg but ICU patients may require more (1.2-1.6 g/kg) Protein requirement is derived from “nitrogen balance” which is nitrogen intake – nitrogen excretion The goal is a positive nitrogen balance of 4-6 grams Nitrogen Balance (g/24 hours) = (protein intake / 6.25)-[UUN+4-6] Must have enough non-protein calories to have the body avoid using proteins for energy (again, more equations but we are not nutritionists)
Thiamine deficiency (B1) Plays an important role in carbohydrate metabolism (substrate in Krebs cycle) Can cause Wernicke’s encephalopathy, dry beriberi (peripheral neuropathy) wet beriberi (cardiomyopathy) Vitamin C deficiency Scurvy Collagen defects Fat Soluble Vitamins A, D, E, K Deficiencies can occur with diseases of malabsorption Cystic fibrosis
feeds! Why? 1) mimics normal nutritional intake Should be started within 24-48 hours in order to take advantage of the effects below 2) reduces infection risk Preserves structural integrity of GI tract mucosa Improves immune function of bowel During bowel rest, gastric mucosa atrophies which increases the amount of bacterial translocation
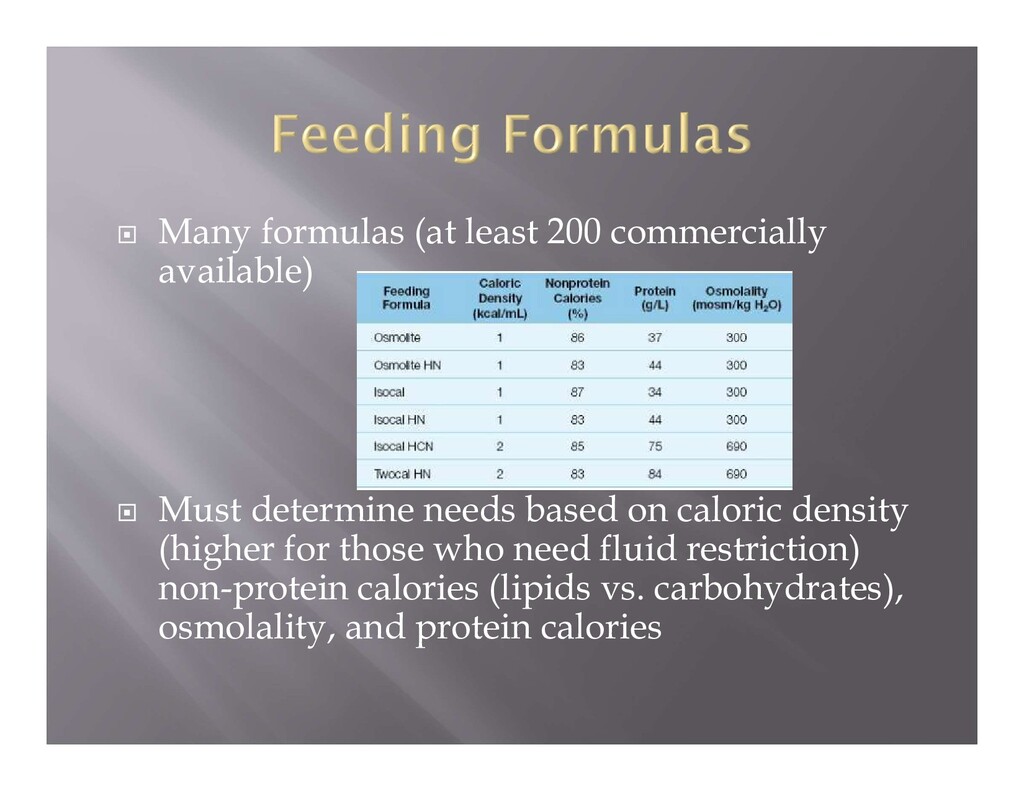
determine needs based on caloric density (higher for those who need fluid restriction) non-protein calories (lipids vs. carbohydrates), osmolality, and protein calories
Generally 50-60 cm Complication: Up to 1% of insertions can advance into trachea In OR can determine this by Inability to ventilate appropriately Circuit leaks Extremely small volumes or desaturation when placed to suction
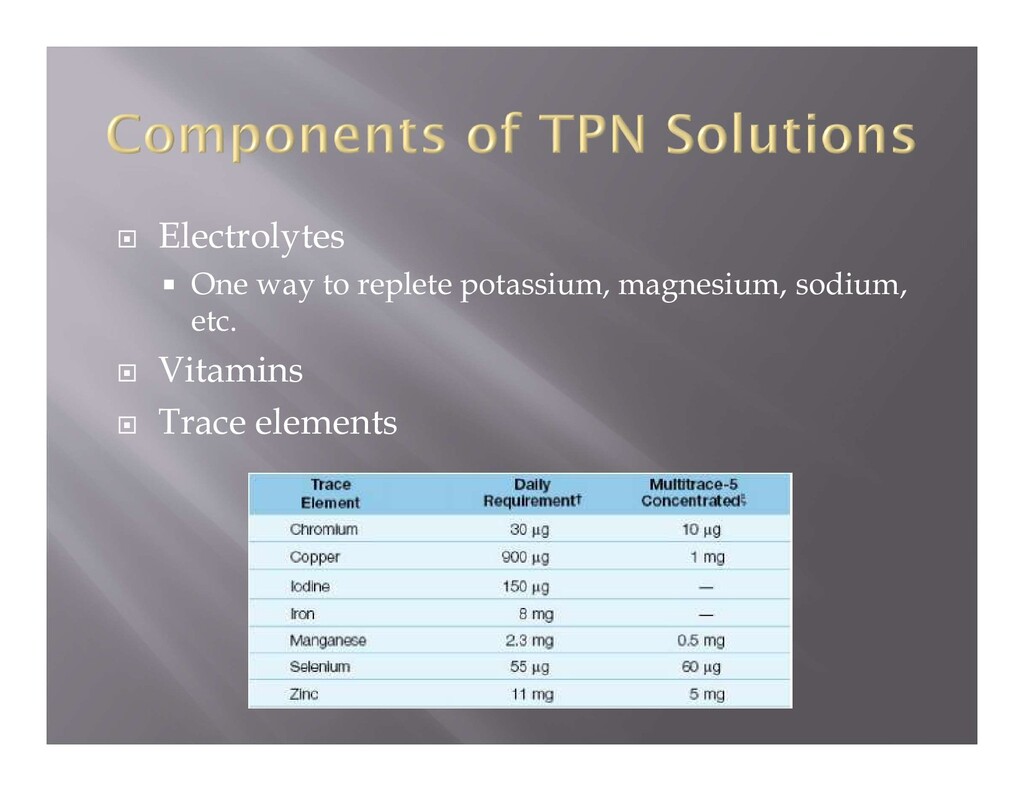
carbohydrate (50% dextrose solution used most often) Protein additives = amino acids (essential and non-essential generally given in 10% amino acid solution) Special amino acid solutions can be used for renal failure, hepatic failure, and severe metabolic distress Lipids = given in emulsion form, 30% of daily calorie needs Dextrose causes these solutions to be hyperosmolar which means that central vein must be used (phlebitis)
Calories = 25 x weight (kg) = kcal/day = 25x70 = 1750 kcal/day Proteins =1.4 (or 1.2-1.6) x weight (kg) = g/day = 98 g/day 2) Determine the volume of solution needed to deliver the protein that is needed (standard solution is 50 g/L protein and 250 g/L dextrose called A10 -D50 ) Vol of A10 -D50 = protein need (g/day) / protein concentration (g/L) = 98/50 = 1.9 L solution daily Can run continuously (1.9/24 = 80 cc/hour) or in bolus feeds 3) Determine the amount of non-protein calories in that volume of solution 1.9 L x 250 g dextrose = 475 g dextrose x 3.4 calories/gram = 1615 kcal/ day from dextrose
calorie needs 1750 kcal needed – 1615 kcal from dextrose = 135 kcal of lipid needed If 10% lipid emulsion is used (1 kcal/cc) then 135 cc lipid emulsion can be added to the solution 5) If at all confused, refer back two slides
these solutions, hyperglycemia is common (BG levels > 300 in 20% of patients in one study) Can begin insulin infusions or add insulin to the TPN solution itself if persistent hyperglycemia
phosphate Hypophosphatemia shown to have correlation with mortality in hospitalized patients Can have difficulty weaning from mechanical ventilation due to associated muscle weakness (NO ATP!)
concentration of oxidizable lipids Hepatic steatosis - elevated liver enzymes due to overfeeding and accumulation of lipids in the liver Cholestasis- lack of lipids in the proximal small bowel prevents cholecystokinin mediated contraction of the gallbladder leading to bile stasis Bowel Sepsis Lack of bulk in the bowel leads to atrophic changes as discussed above
from hyperosmolarity and hyper/hypoglycemia TPN may be continued if hyperosmolarity will not pose a significant intraoperative problem New data shows that abrupt discontinuation of TPN is not likely to lead to hypoglycemia as was previously believed (Grade A evidence) Strict asepsis must be maintained (keep one line separate for TPN administration)
healthy, 35 year old woman is mechanically ventilated in the ICU. Her respiratory quotient is 0.97. Her primary metabolic fuel is most likely to be A) proteins B) fats C) carbohydrates D) TPN RQ = CO2 eliminated / O2 consumed Fats = 0.7, protein = 0.8, carbs = 1.0
patient is having difficulty weaning from the ventilator. Her injuries are unrelated to her respiratory mechanics. Her electrolytes are within normal limits. She has been receiving TPN as she suffered significant bowel injury. What should the next step be? A) add phosphate to her TPN solution B) modify her TPN solution to contain more protein and lipid C) change nothing and give more time to wean D) start enteral feeding
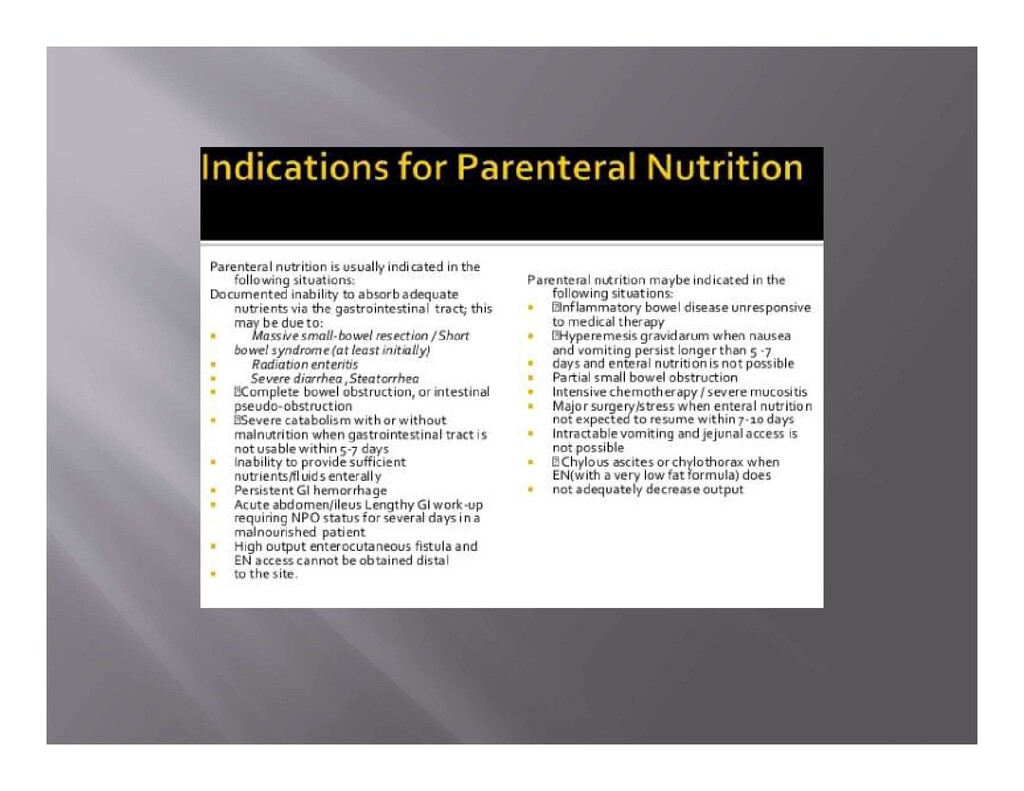
for TPN? A) 65 year old man with sepsis due to influenza B) 32 year old female with mild flare of inflammatory bowel disease C) 32 year old female with short gut syndrome D) 65 year old man in heart failure with an LVAD
ICU after a major MVC where he suffered significant trauma. Enteral feeds are initiated 24 hours after admission. Which of the following amino acids will be most beneficial to add to the feeds? A) aspartic acid B) glutamate C) Tyrosine D) Cysteine Glutamate is a non-essential amino acid which can be depleted in major trauma or burn injuries. It helps to maintain intact gut mucosa which decreases the chance of infection and maintains healthy cells of the immune system
complication from TPN administration? A) increased translocation of bacteria through the GI tract B) infection from indwelling central lines C) gastrointestinal mucosal hypertrophy D) hyperglycemia E) hypophosphatemia F) hypermagnesemia Complications from TPN administration can include bacterial translocation, infection, hyperglycemia, hypophosphatemia and hyper/hypomagnesaemia
occurs when nutrition is re- instituted after a period of starvation. Hypophosphatemia occurs due to depletion from rebuilding of tissues leading to muscle weakness and glucose intolerance. Hypocalcemia, hypomagnesemia and hypokalemia may also be associated. It is important to begin refeeding with a balanced fat, carbohydrate and protein diet that is below the resting energy expenditure.
with anorexia nervosa. Two days later she complains of muscle weakness and fatigue. What is most likely to be found in this patient? A) hypophosphatemia, hypoinsulinemia, decreased protein, fat and glycogen synthesis B) hypophosphatemia, hyperinsulinemia, increased protein, fat and glycogen synthesis C) hyperphosphatemia, hypoinsulinemia, increased protein, fat and glycogen synthesis D) hyperphosphatemia, hyperinsulinemia, decreased protein, fat and glycogen synthesis
to using peripheral veins as opposed to central veins for administration of TPN? A) need for long-term administration B) osmolality of the solution C) risk of infection D) difficulty of insertion The highest osmolality solution that can be accommodated by peripheral veins is 750 msom/L (or a 12.5% dextrose solution). Higher osmolality solutions can cause increased risk of phlebitis. Central cannulation causes higher risk of Infection though the subclavian site can reduce this risk.
a bowel resection and end ileostomy for ruptured diverticulum. He is started on TPN several days later. Which of the following is the corresponding respiratory quotient for each of the metabolic fuels? A B C D
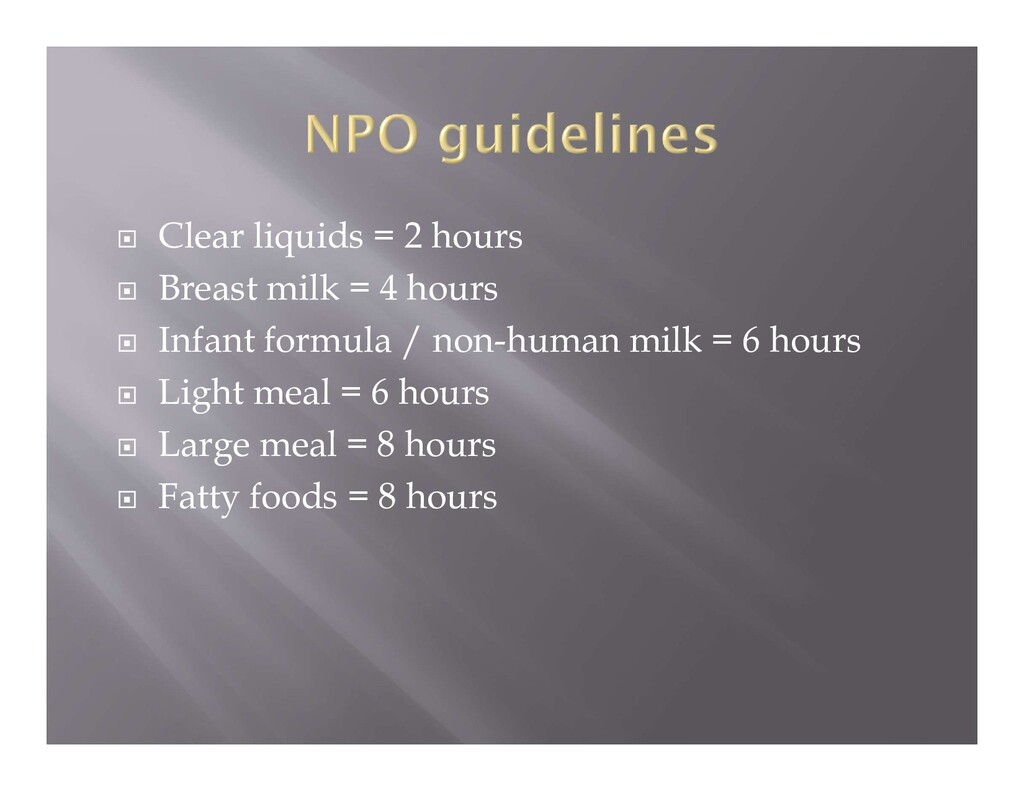
do an elective inguinal hernia repair on a 31 year old male. He ate toast and drank black coffee for breakfast at 6 am. What should you tell the surgeon is the earliest that you will be willing to do the case? A) 7 am B) 10 am C) 12 pm D) 2 pm
from baseline. How does FRC change under general anesthesia in an obese patient? A) increases by 20% from baseline B) reduced the same as a non-obese patient C) reduced by 30% from baseline D) reduced by 50% from baseline
wall compliance Rapid shallow breathing Increased work of breathing Leads to limited ventilatory capacity In addition, increased oxygen utilization and CO2 production leading to more ventilation requirements
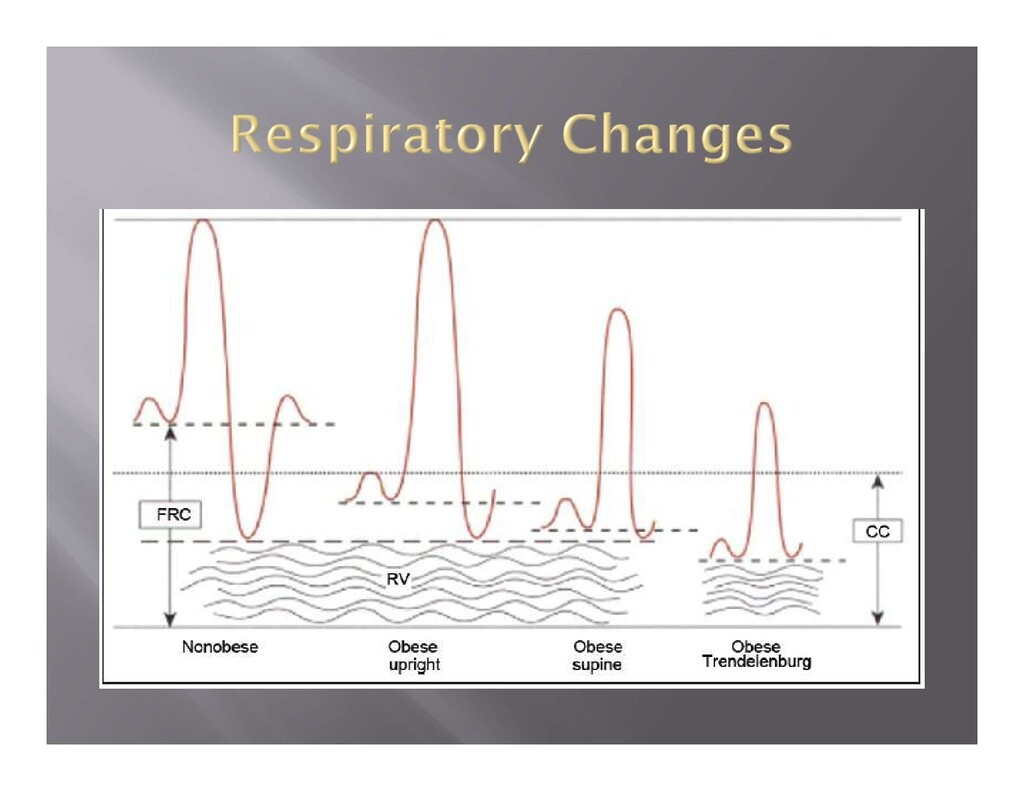
normal Decreased FRC Decreased Vital Capacity Decreased TLC Unchanged closing capacity However lung volumes may be reduced to the point of being below closing capacity Can cause right to left shunting and arterial hypoxemia Dead space unchanged Respiratory pattern accentuated with insufflation of abdomen
surgery under general anesthesia. Which of the following statements concerning cardiac output of this patient is true compared to a patient who weighs 70 kg? A) cardiac output is diminished by a factor of 2 B) cardiac output is diminished by 10% C) cardiac output is similar D) cardiac output is increased by 10% E) cardiac output is doubled
100 cc/minute Increased stroke volume and ventricular dilation Each kg of adipose contains about 3,000 meters of vessels Blood volume increased leading to propensity for hypertension Leads to concentric hypertrophy Leads to increased risk of heart failure, arrhythmias and ischemia Heart rate is unchanged
affect the cardiovascular system? A) hypoxemia and hypercapnea leading to increased pulmonary pressures and increased RV pressure (cor pulmonale) B) hypoxemia and hypocapnea leading to increased pulmonary pressures and increased RV pressure C) hyperoxia and hypercapnea leading to decreased pulmonary pressures and decreased RV pressure (cor pulmonale) D) hyperoxia and hypocapnea leading to decreased pulmonary pressures and decreased RV pressure
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}