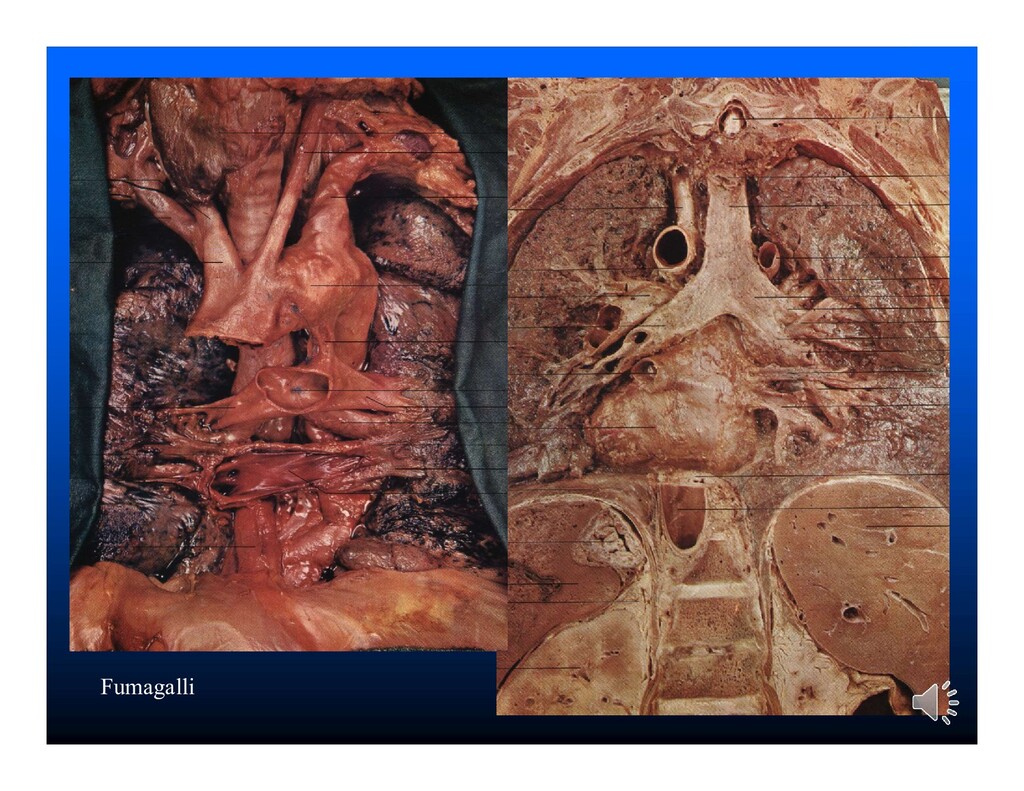
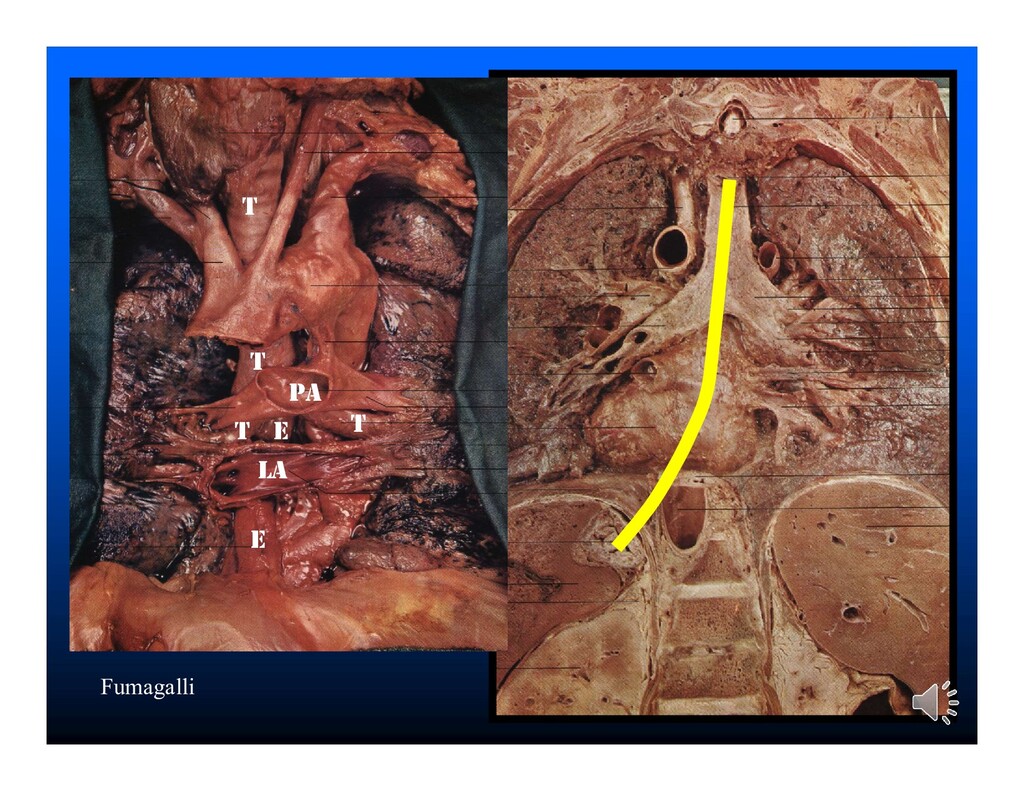
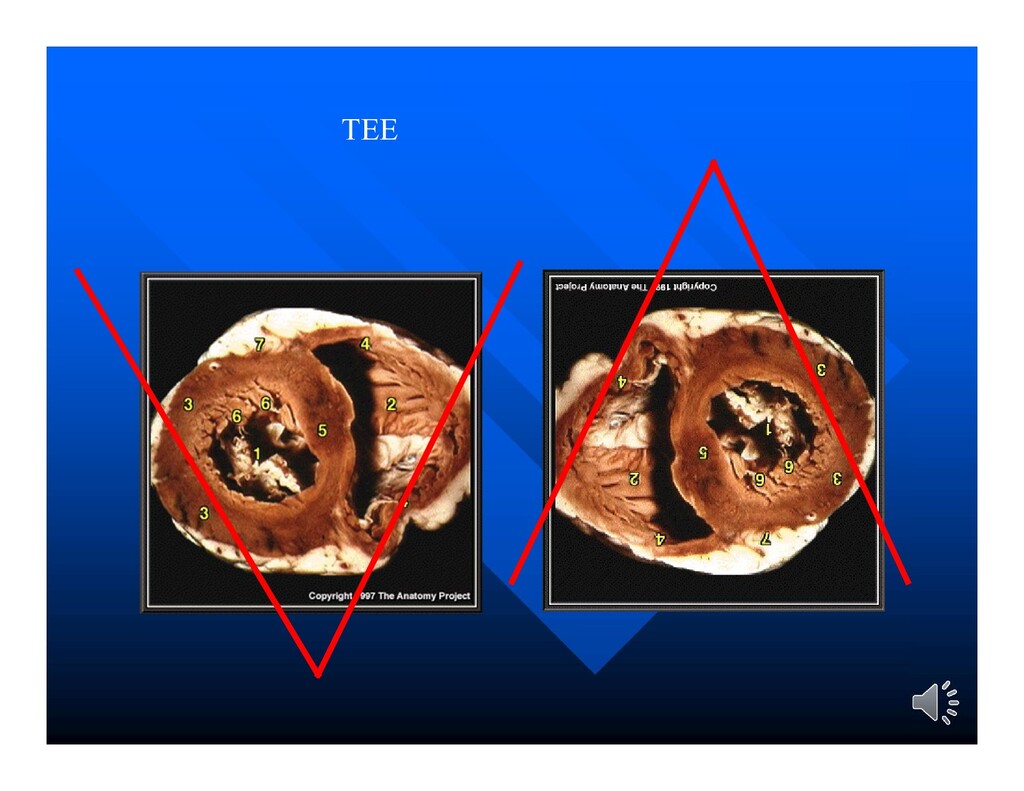
complete or adequately detailed information in the evaluation of: – posterior cardiac structures (e.g. left atrium, left atrial appendage, interatrial septum, the aorta distal to the root) – assessment of prosthetic cardiac valves – delineation of cardiac structures less than 3 mm in size (e.g. small vegetations or thrombi) Pavlides et al., 1990
is significantly limited by ultrasound interference by chest wall and lung especially in obese and elderly patients and in patients with COPD TEE is conclusive in many cardiac diseases so that it can diagnose 95% of cases versus 48% using TTE Pavlides et al., 1990
procedure: 5.6% 1.4% valvular 4.2% PFO Anesthesia & Analgesia 2002 95(4):824-7 TEE altered the management in five ways in the OR or ICU: 1) changing medical therapy 2) changing surgical therapy 3) confirmation of a diagnosis 4) positioning of an intravascular device 5) substitute to a pulmonary artery catheter Can J of Anaesthesia 2002 49(3):287-93
in 300 patients: clinical impact 1.3% 0.7% had an additional valve repair /replaced 0.7% diagnosed valvular malfunction / complication J Am Soc of Echocardiography 2001 14(7):659-67 TEE is a beneficial and cost-effective intervention in children requiring complex cardiac repair Surgical therapy was altered in 3% of patients. Am Heart Journal 1999 138:771-6
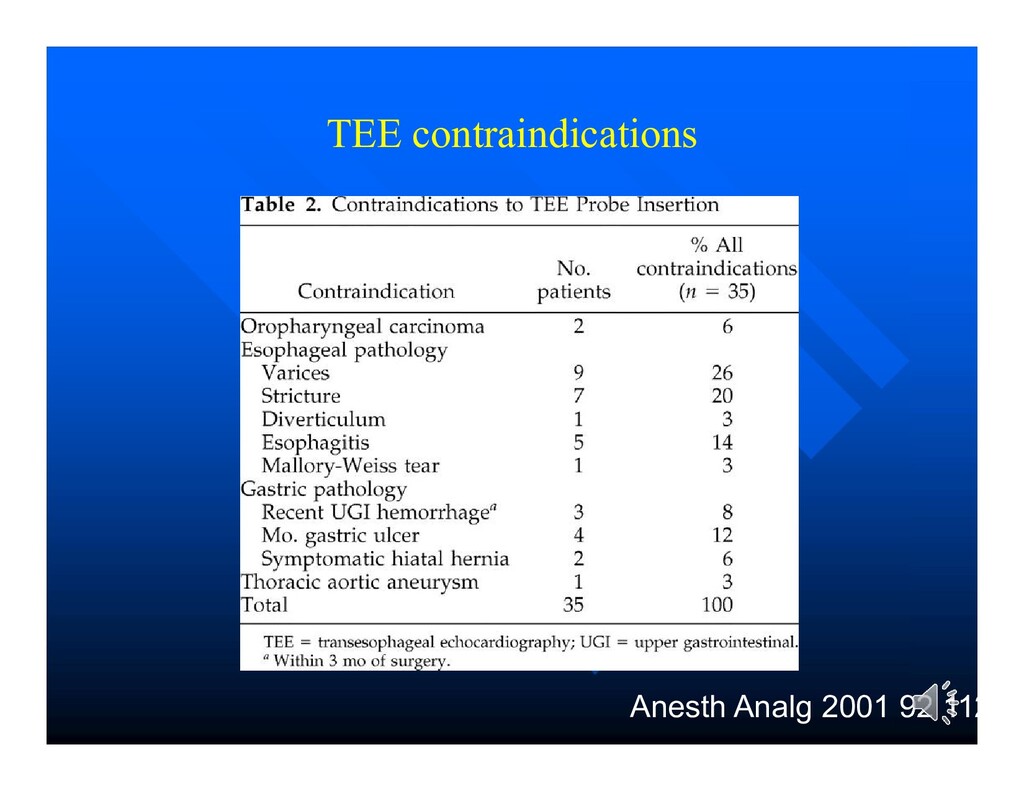
varices, dysphagia, etc) Severe respiratory insufficiency (non-intubated patient) Large ascending thoracic aortic aneurysm Absolute Esophageal or gastric perforation / recent surgery No cardiopulmonary resuscitation equipment available
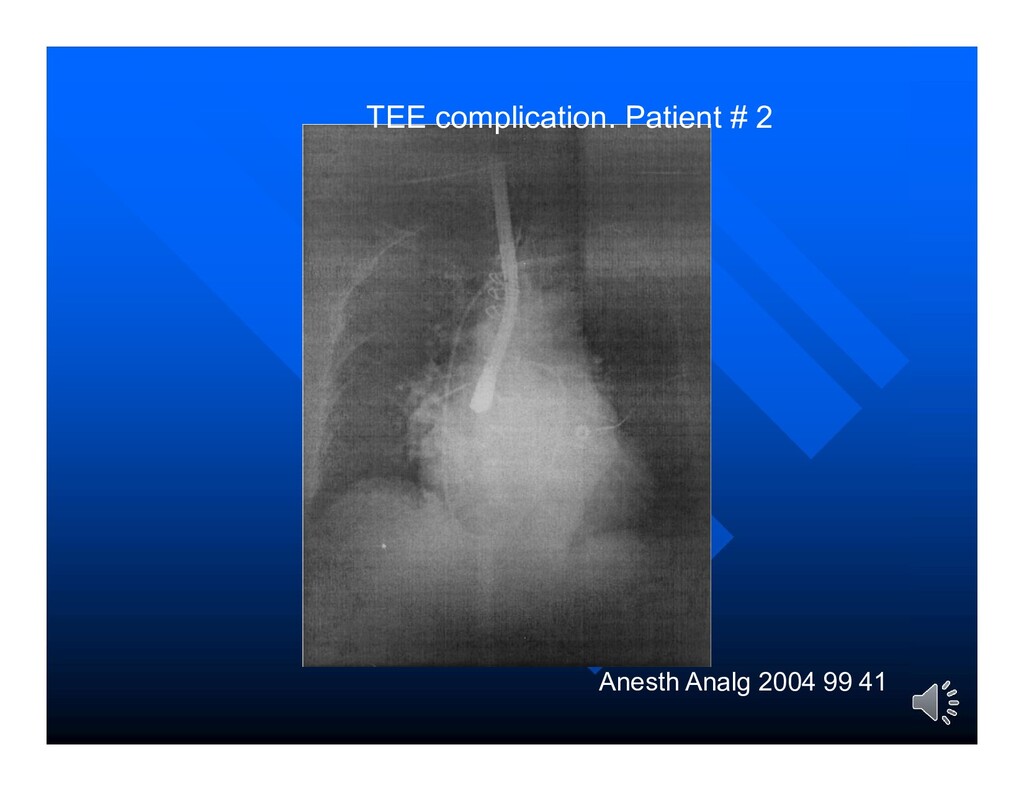
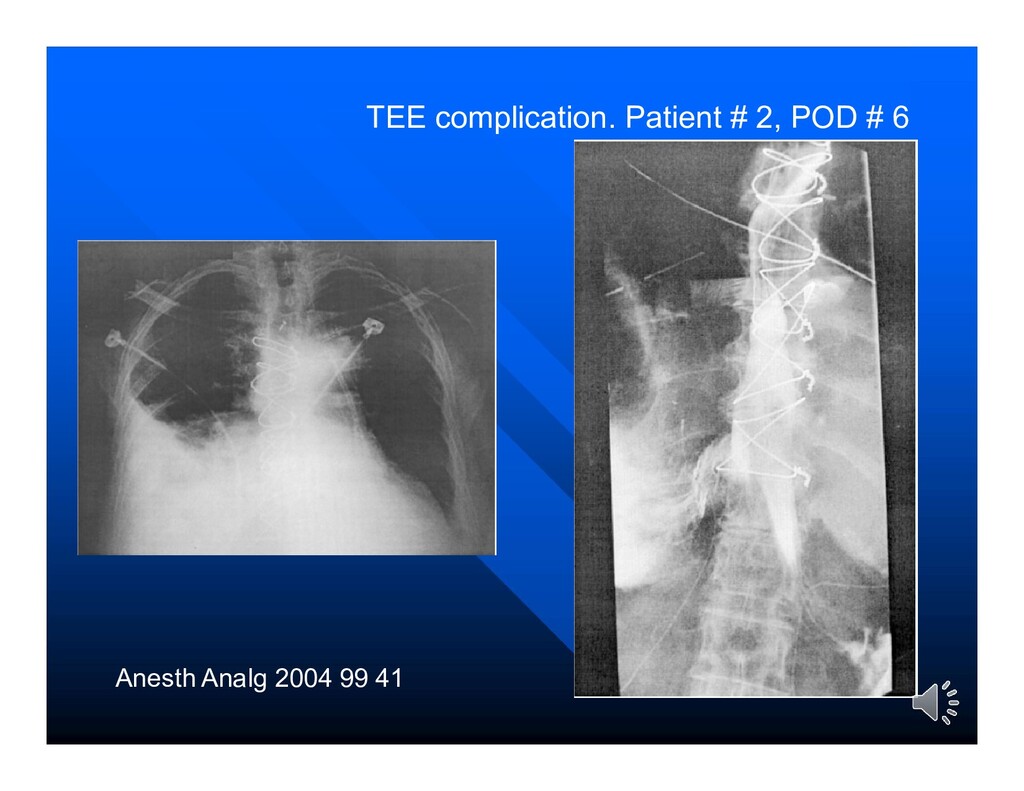
0.5% – Out of 10,000 one death »hemorrhage from esophageal cancer. –Swallowing dysfunction (7.8 times greater odds) –Gastro-esophageal injury estimated in one in 10,000 • ICU –Complications rate 1.7% –Serious Cx 0.2% (respiratory failure, seizures) • 7200 intraoperative TEE performed in cardiac surgical patients, • no mortality and a morbidity of only 0.2% were observed Anesth Analg. 2001;92:1126-30
jefe 1889, Óleo sobre lienzo, 290 x 445 cm. Luis Jimenez Aranda (1845-1928) Museo del Prado, Madrid. https://www.museodelprado.es/coleccion/obra-de-arte/una-sala-del-hospital-durante-la-visita- del/318cc81b-77d6-4688-ad98-ffbe3dd7a4a5
perform landmark-based techniques when an ultrasound is not available” Largest barrier appears to be the lack of a clear path for training and credentialing physicians in bedside ultrasound techniques. Conclusions
Easy to learn the basic examination Part of the training of the anesthesiologist, intensivist, trauma surgeon, and emergency physician (should be) Conclusions
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}