of the circuit O Review CPB related anesthetic goals O Discuss circulatory arrest and its consequences O Highlight high yield topics likely to show up on exams
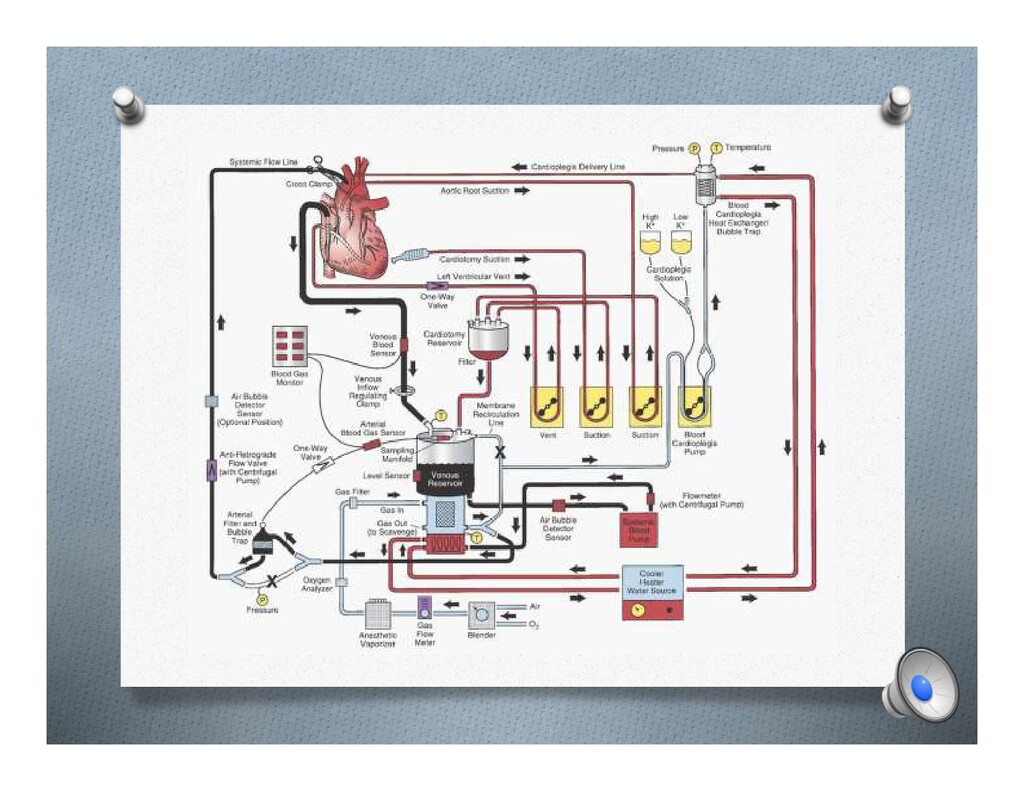
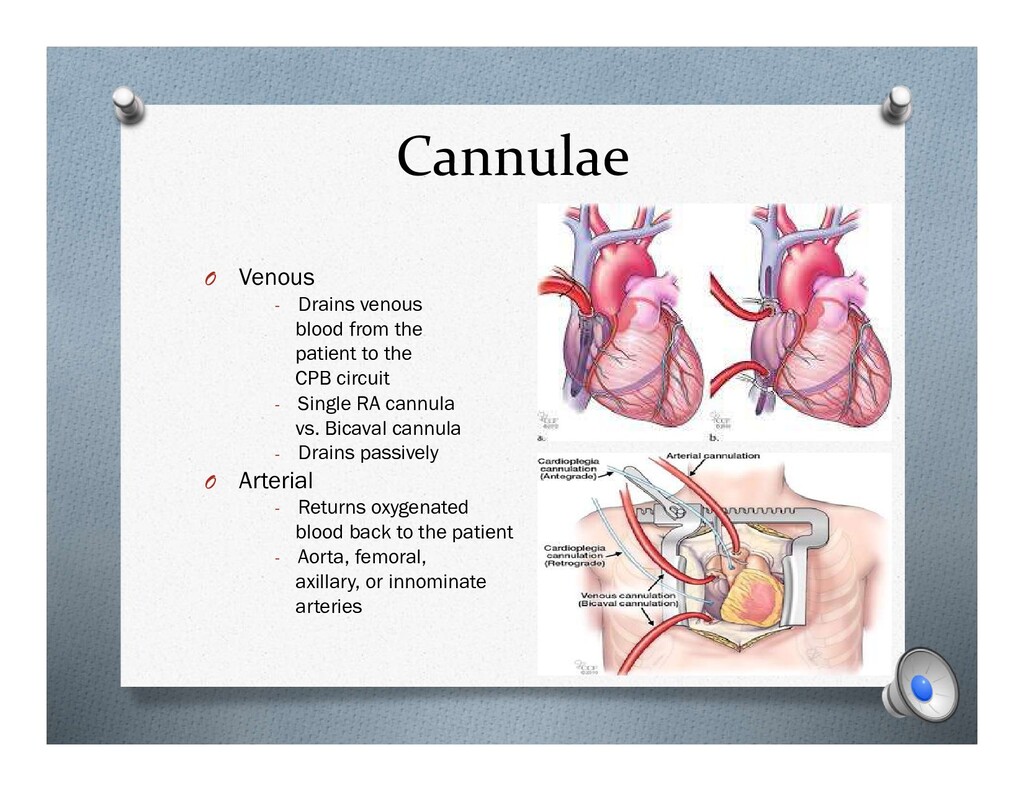
to the CPB circuit - Single RA cannula vs. Bicaval cannula - Drains passively O Arterial - Returns oxygenated blood back to the patient - Aorta, femoral, axillary, or innominate arteries
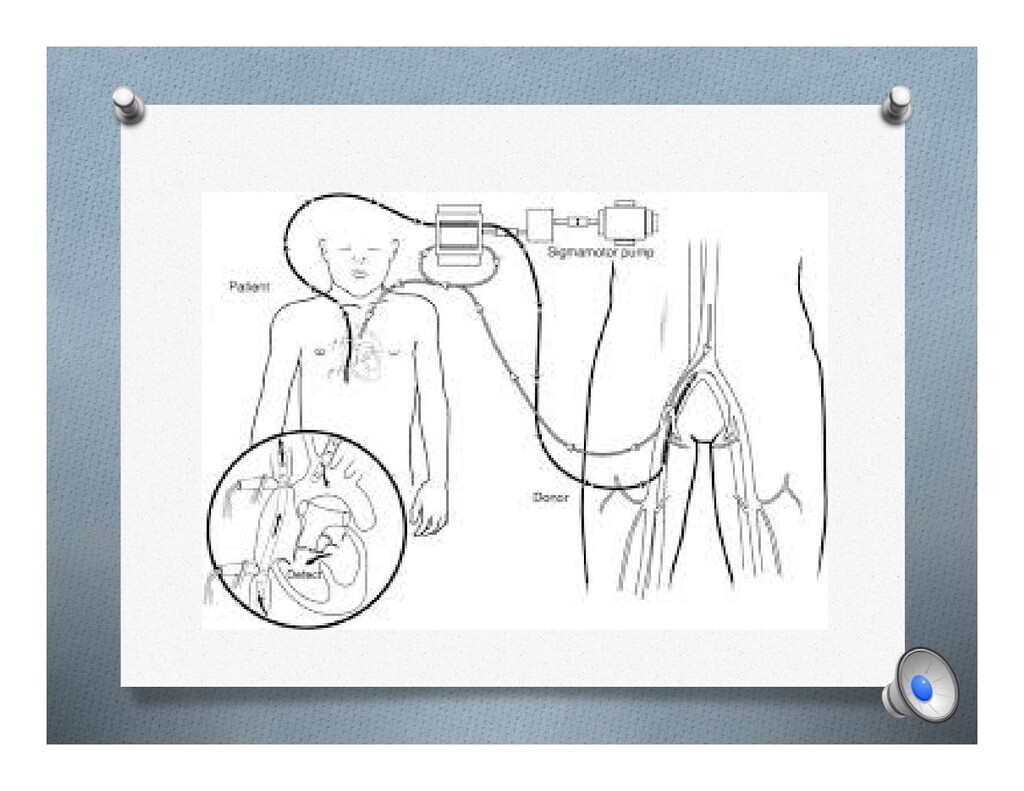
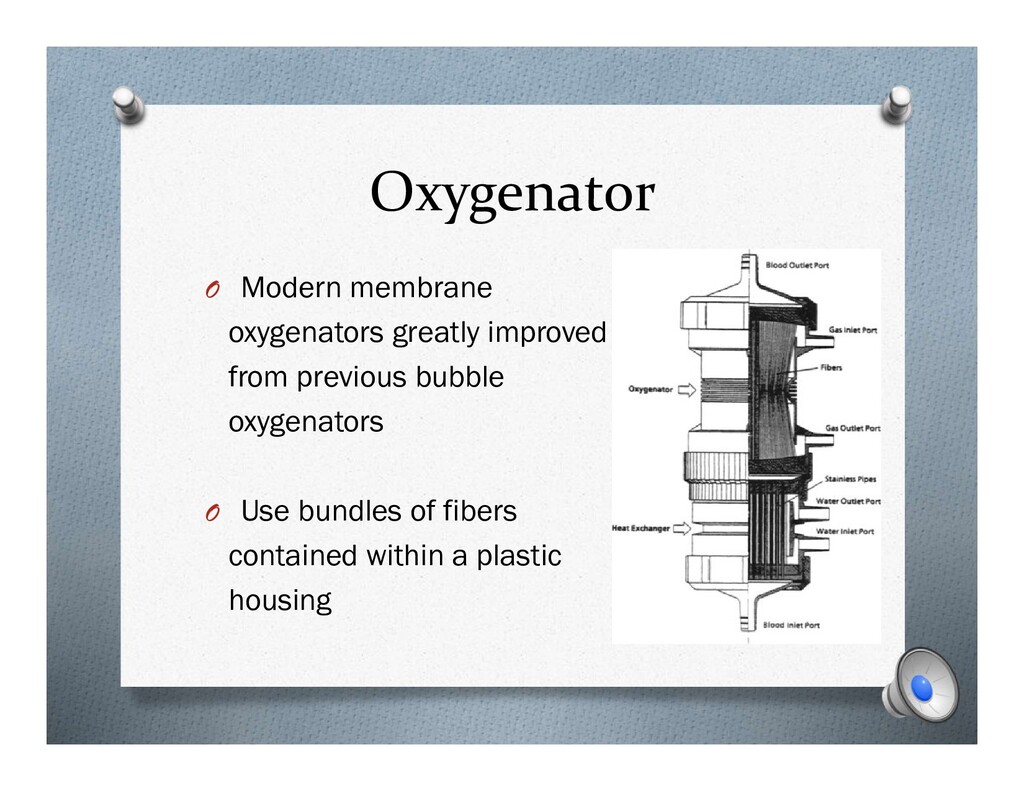
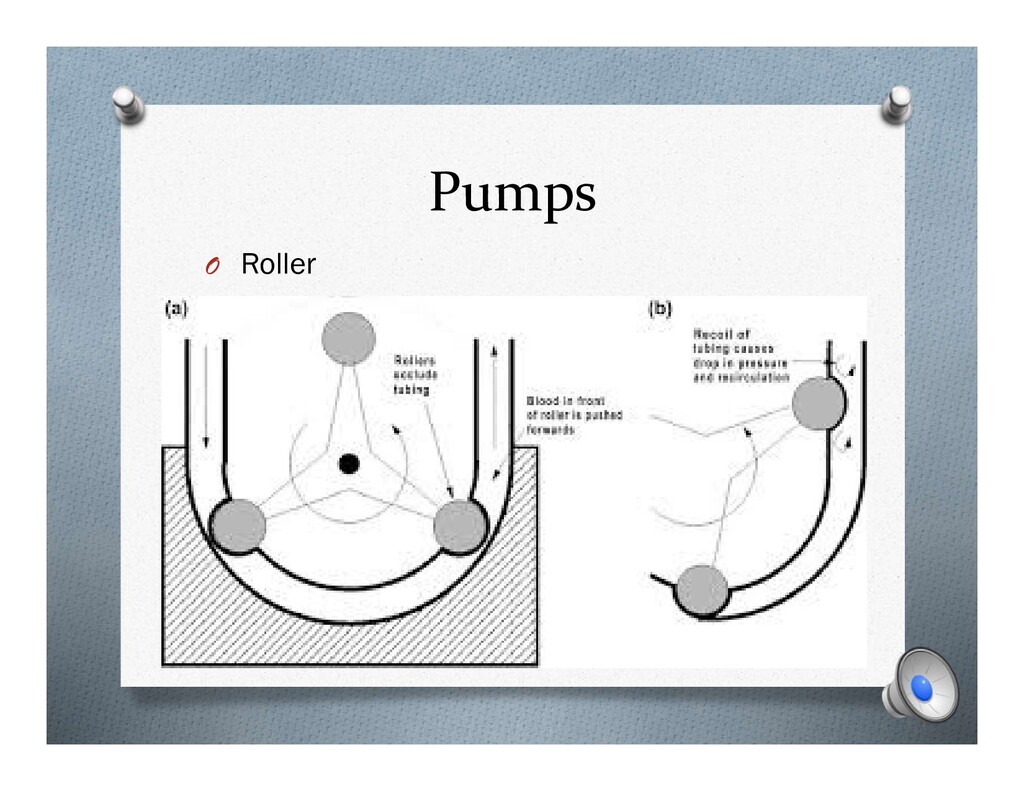
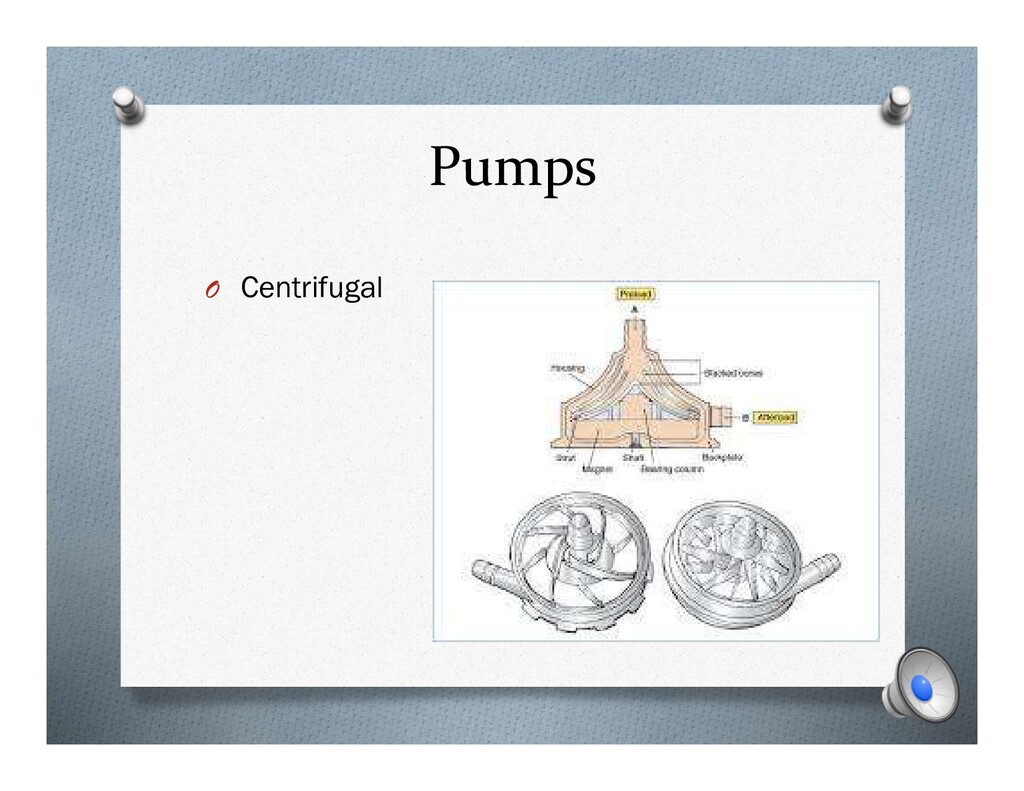
practice today O Centrifugal: magnetically controlled impeller rotate to provide flow O Roller: simplest and earliest type - Works by alternating tube compression and release 180 degrees apart
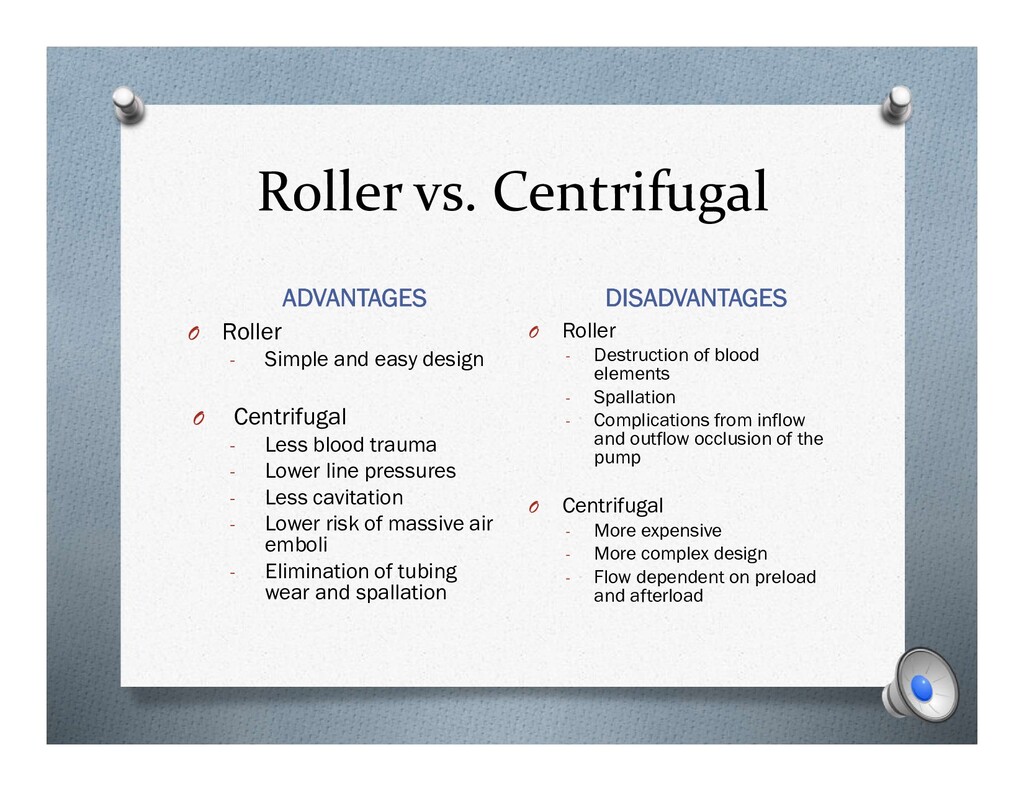
easy design O Centrifugal - Less blood trauma - Lower line pressures - Less cavitation - Lower risk of massive air emboli - Elimination of tubing wear and spallation O Roller - Destruction of blood elements - Spallation - Complications from inflow and outflow occlusion of the pump O Centrifugal - More expensive - More complex design - Flow dependent on preload and afterload
pulsatile flow. O Lack of pulsatile flow has been linked to renal dysfunction and production of ischemic metabolic by-products O Increased survival seen in high risk patients with the use of pulsatile flow on CPB
tubing O Crystalloid solution with additives - Mannitol - Albumin - Heparin - Calcium O Average prime volume ~ 1500 ml O RAP: patient blood partially primes CPB tubing
coagulation cascade O Preventing thrombosis requires anticoagulation prior to cannulae insertion O Heparin = AC of choice O What is the dose? O How is it monitored?
AT III alters its configuration and increases its thrombin inhibitory potency > 1,000 fold O Inhibiting thrombin prevents formation of fibrin clot O Higher doses required in patient’s on heparin preoperatively or in those with AT deficiencies
levels - First step: O try giving additional dose of heparin and recheck - Next step: O Give FFP (contains AT III) - Finally: O Administer exogenous AT III
Mild form: associated with transient decrease in platelet count 2. More severe form: autoimmune mediated decrease in platelet count 2/2 formation of anti- PF4 Platelet clumping and microvascular thrombosis O What to do with these patients: O Type 1, if possible wait until platelet number recovers before proceeding to surgery O Type 2, heparin alternatives should be used Defibrinogenating agents: Hirudin, Bivalrudin, and Factor Xa inhibitors
- Nature of the surgery itself - Reoperation (higher blood loss) - Use of anticoagulants or antiplatelet agents - Platelet dysfunction and coagulopathy due to CPB
of shed blood O cell saver - Use of antifibrinolytics O Aminocaproic acid and TXA - Retrograde autologous Prime - Ultrafiltration O Contraindications to autologous hemodilution: - Preoperative anemia - Unstable angina - High grade coronary stenosis (LM disease) - AS
O Lysine analogs O Bind plasminogen and block its ability to bind lysine residues on fibrinogen prevents lysis of fibrin clots - Aprotinin O Naturally occurring fibrinolytic O inhibits kallikrein, preserves platelet glycoprotein receptors, inhibits proinflammatory cytokine release, and inhibits plasmin and protein C O No longer in use in US
partially replaced by patient’s blood drained retrograde via arterial cannula - Reduces hemodilution and decrease in SVR when initiating CPB - Must watch for acute hypovolemic hypotension! O Ultrafiltration - AKA hemoconcentration - Done by perfusionist on CPB - Reduces free water, Increases HCT, preserves hemostasis, and decreases circulating inflammatory mediators
neuro protection - Benefits: O reduction in metabolic rate and O2 consumption O preservation of high-energy phosphate substrates O reduction in excitatory neurotransmitters - Can be active or passive (most cardiac surgeries involve active cooling to 32°C)
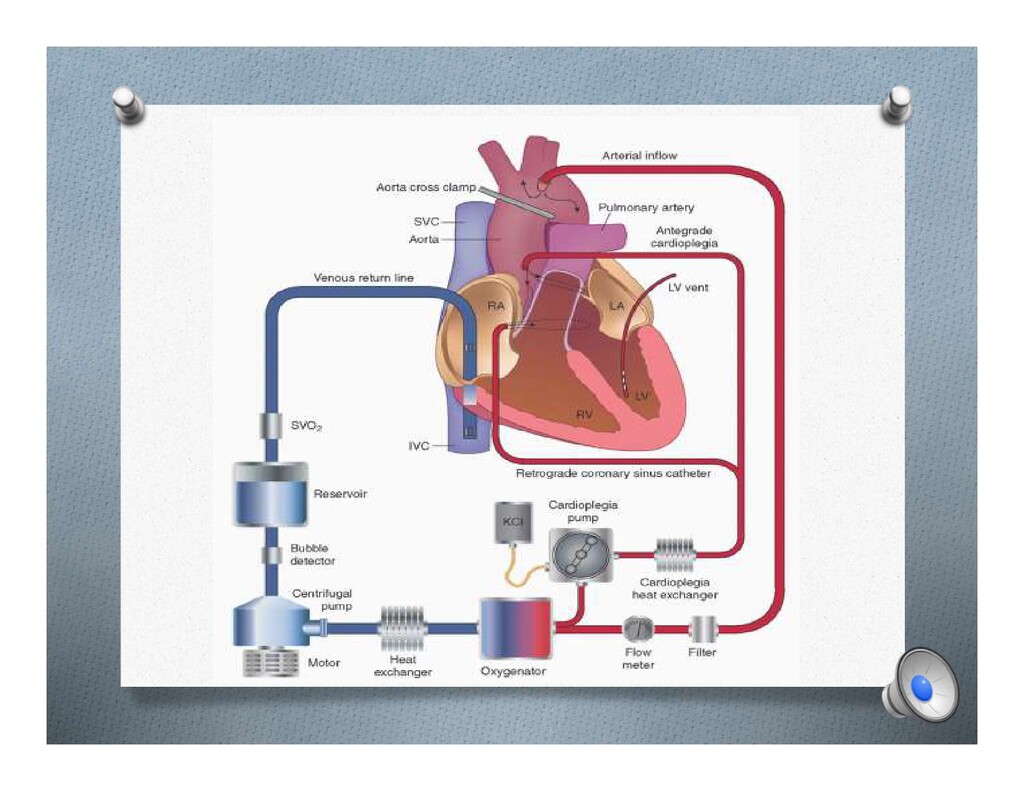
blood or crystalloid with high potassium concentration injected into coronary arteries or veins induces diastolic electrical arrest - Antegrade O injected via aortic root following cross clamping and into native coronary arteries O follows normal flow of blood - Retrograde O used in patients with severe CAD and/or AI O Coronary sinus catheter
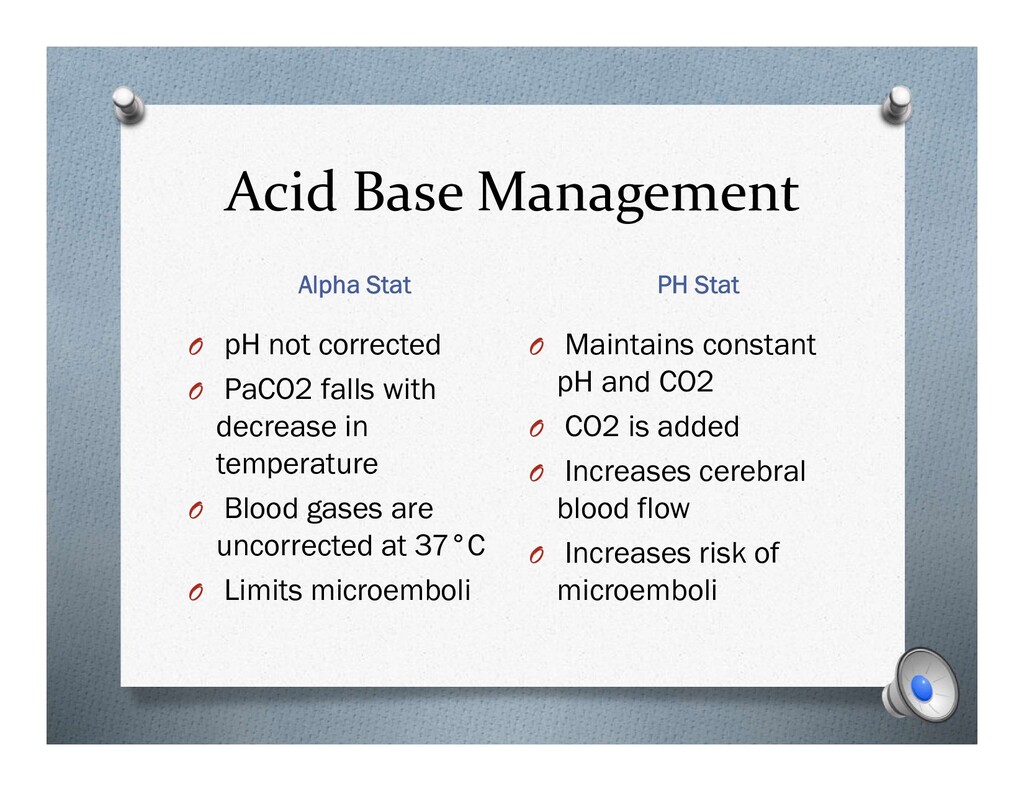
corrected O PaCO2 falls with decrease in temperature O Blood gases are uncorrected at 37°C O Limits microemboli O Maintains constant pH and CO2 O CO2 is added O Increases cerebral blood flow O Increases risk of microemboli
- Type A aortic dissections - Complex aortic arch repairs - Resection of IVC tumors O Temperature Control: - Cool to 18- 20 °C - Pack the head and heart with ice
- High dose steroids have been shown to attenuate cerebral response to ischemia - Cerebral oximetry monitoring - Antegrade and retrograde cerebral perfusion can extend acceptable period of DHCA O Physiologic Consequences - Extensive cooling and rewarming associated with significant coagulopathy - High risk of ischemic cerebral injury - Impaired glucose metabolism
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}