of acute pain • Define the elements involved in pain processing • Identify the chemical mediators of transduction and transmission of pain • Discuss Neural Plasticity as it relates to sensitization • Briefly identify various methods for assessing acute pain • Overview of treatment options for acute pain
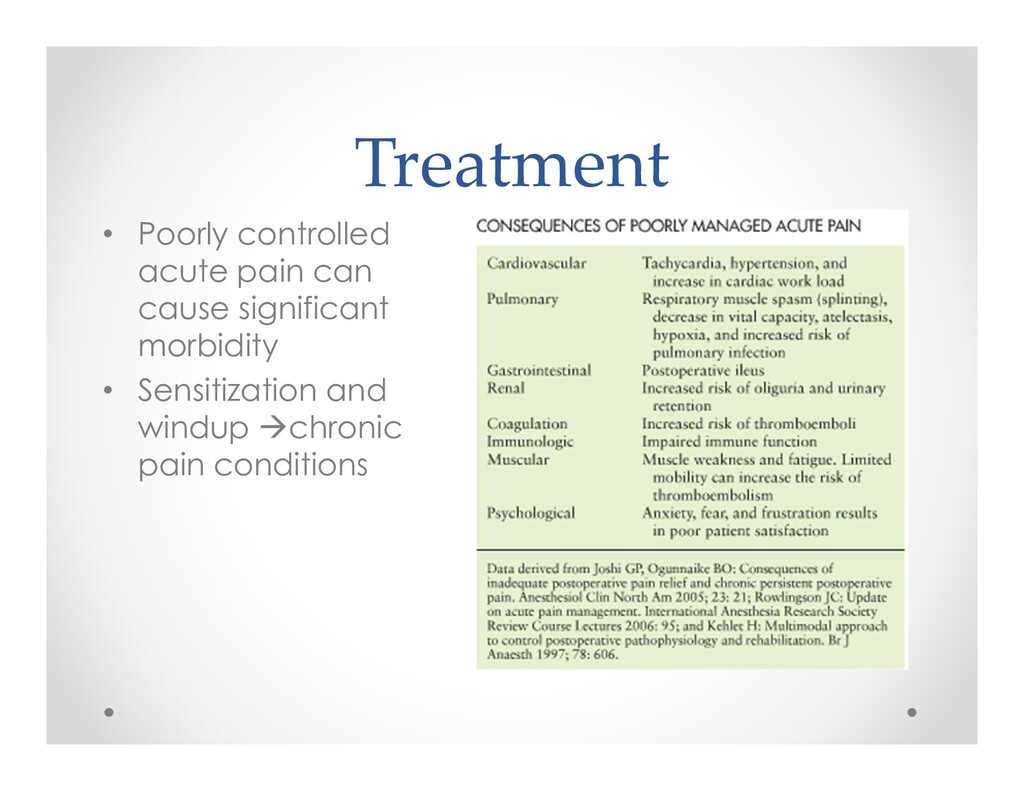
an adverse chemical, thermal or mechanical stimulus o Typically resolves within 1 month o Poor management can result in increased morbidity and mortality, delayed recovery, patient dissatisfaction, adverse psychological effects and neuronal plasticity
in response to a noxious stimulus o Visceral – Sympathetic and parasympathetic o Somatic • Inflammatory – in response to tissue damage and inflammation o Burn, arthritis • Neuropathic – primary lesion or dysfunction of peripheral or central nervous system o Central post-stroke pain syndrome, Tumor, Trigeminal neuralgia, CRPS, diabetic neuropathy, Spinal stenosis • Non-inflammatory/Non-neuropathic – Abnormal central processing o Fibromyalgia, irritable bowel syndrome
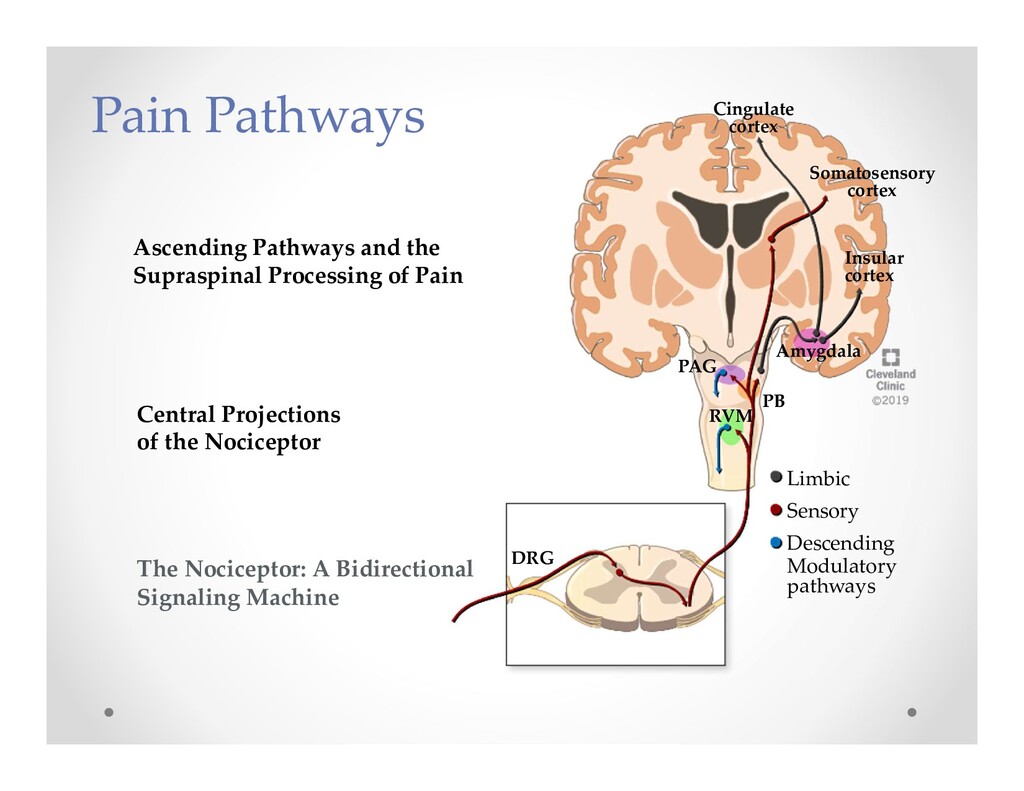
o Spinothalamic tract thalamus somatosensory cortex o Spinoparabrachial tract ventral medial nucleus of hippocampus and central nucleus of the amygdala (Limbic System)
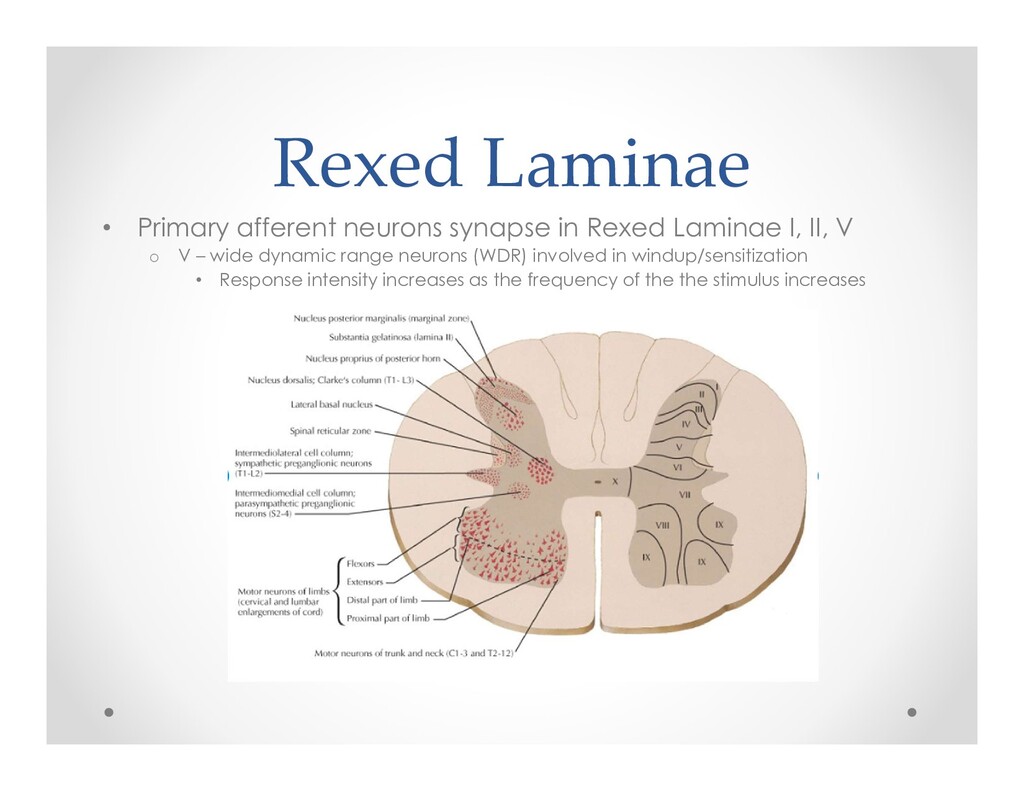
I, II, V o V – wide dynamic range neurons (WDR) involved in windup/sensitization • Response intensity increases as the frequency of the the stimulus increases
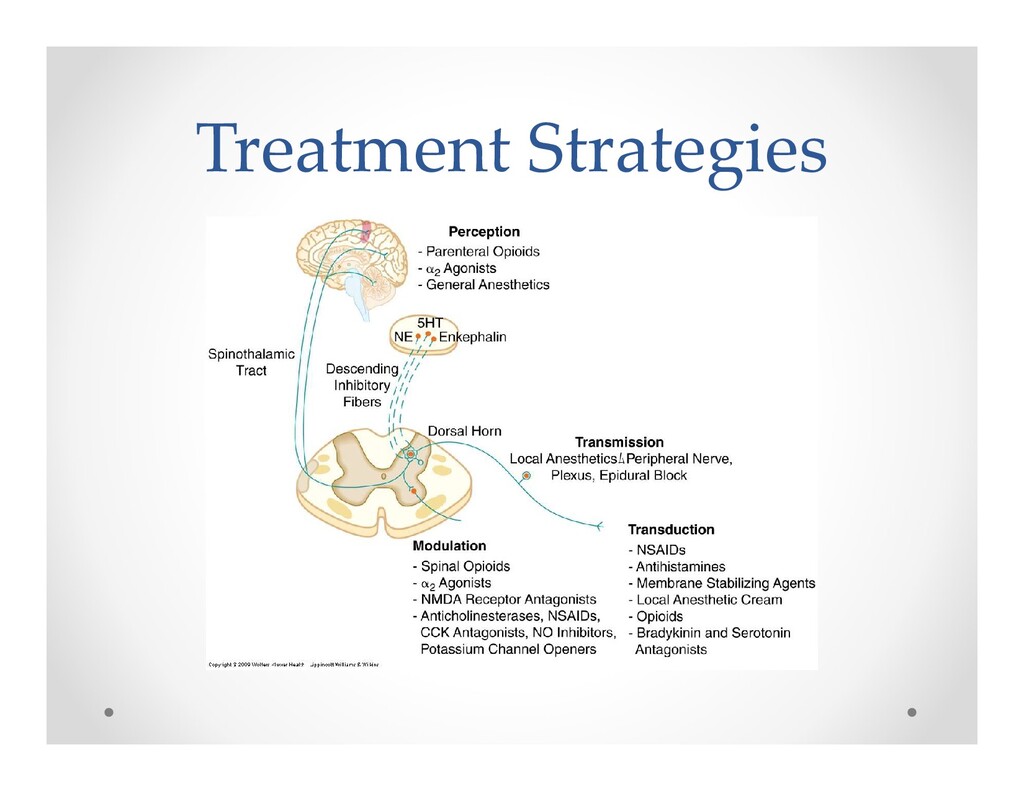
action potential • Transmission – AP is conducted through the nervous system via 1st, 2nd and 3rd order neurons from the periphery through the dorsal horn to the thalamus and cortex • Modulation – altering of afferent transmission o Inhibition vs. augmentation • GABA/glycine release • Activation of descending inhibitory efferent pathways from motor cortex, hypothalamus, PAG NE, 5-HT, endorphin release in dorsal horn • Central sensitization – windup occurs due to repetitive stimulation of WDR neurons by C fibers • Perception – integration of painful input into somatosensory or limbic cortex
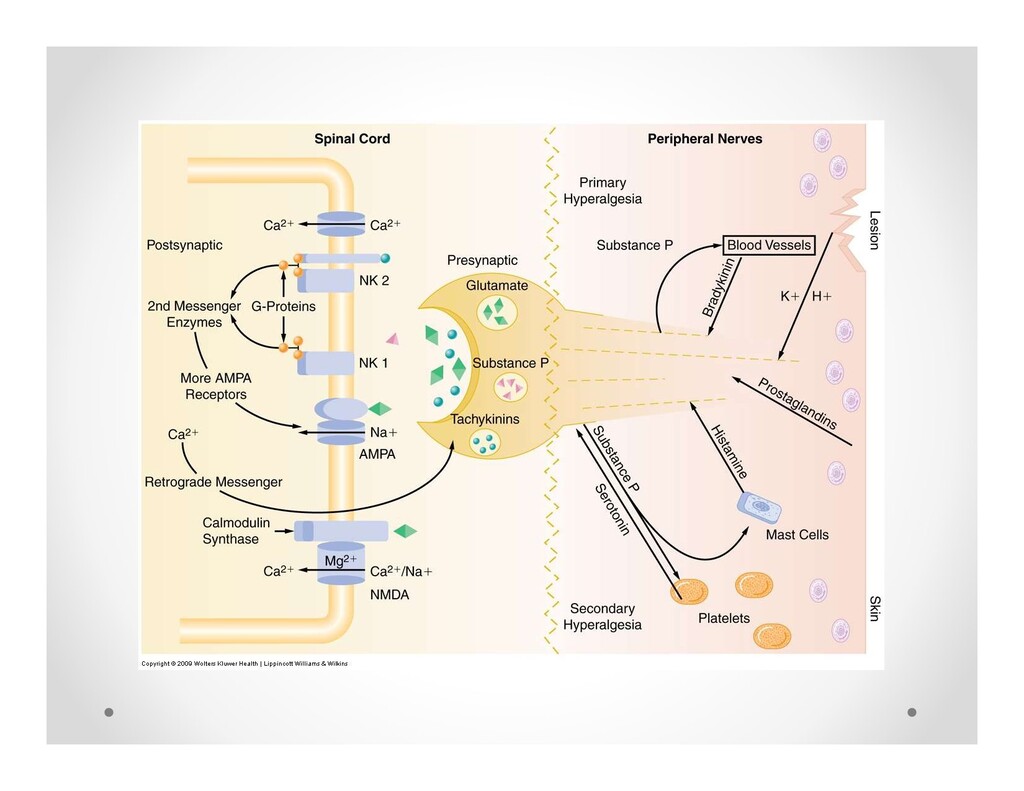
following prolonged depolarization of cell membrane • Crucial role in sensitization o Substance P removal of Mg blockade glutamate activation of NMDA receptor • AMPA • Kainate o Na channel dependent fast synaptic afferent input • Metabotropic
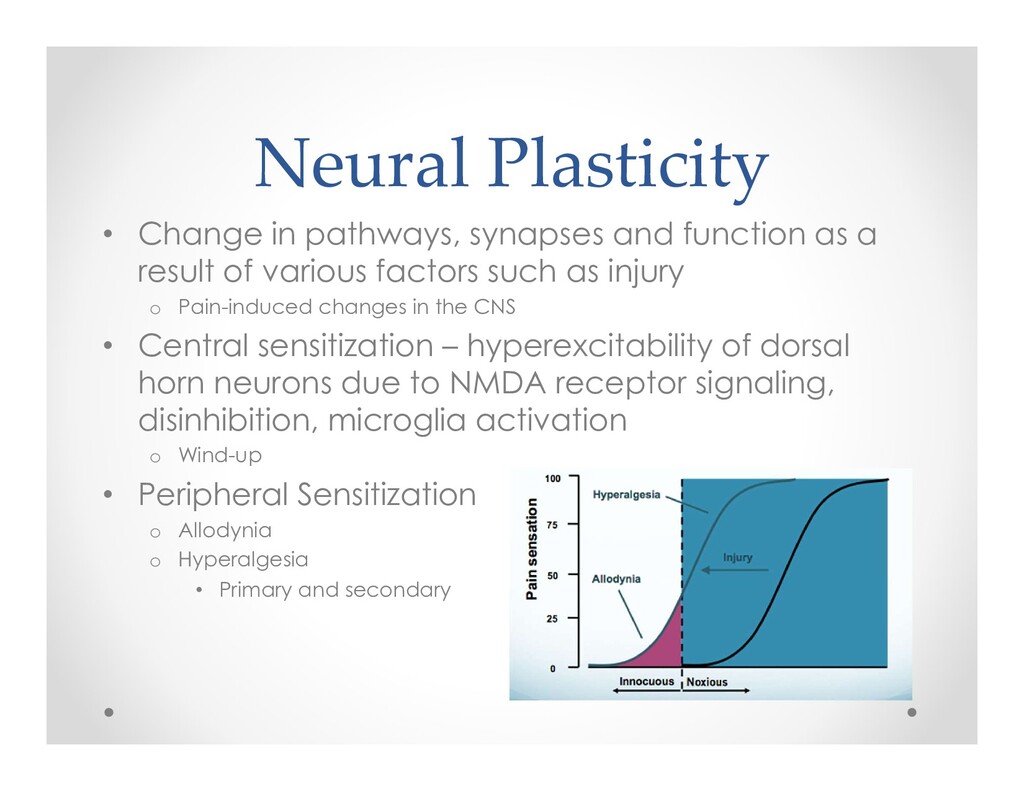
a result of various factors such as injury o Pain-induced changes in the CNS • Central sensitization – hyperexcitability of dorsal horn neurons due to NMDA receptor signaling, disinhibition, microglia activation o Wind-up • Peripheral Sensitization o Allodynia o Hyperalgesia • Primary and secondary
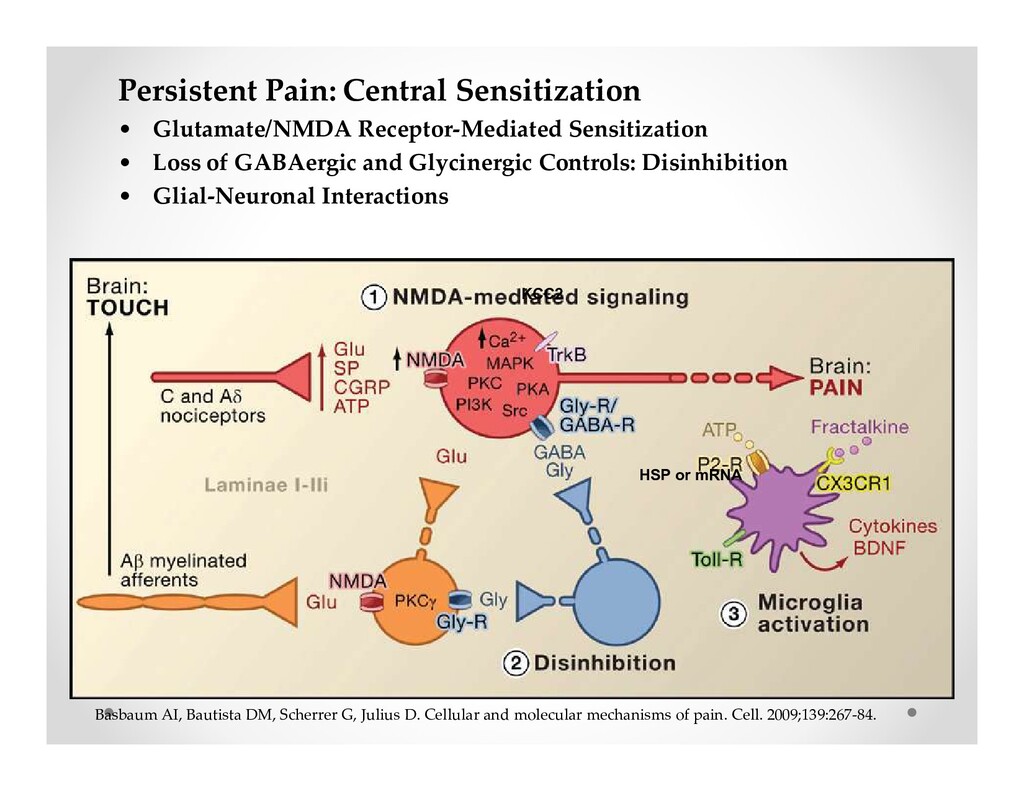
of GABAergic and Glycinergic Controls: Disinhibition • Glial-Neuronal Interactions HSP or mRNA KCC2 Basbaum AI, Bautista DM, Scherrer G, Julius D. Cellular and molecular mechanisms of pain. Cell. 2009;139:267-84.
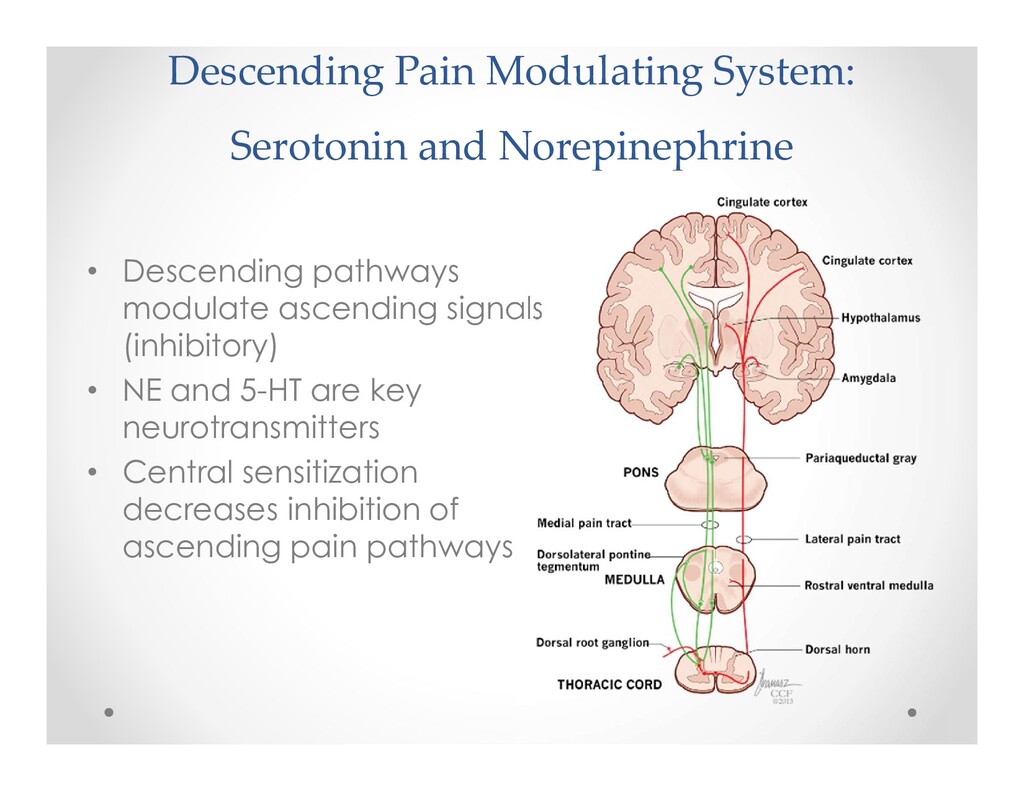
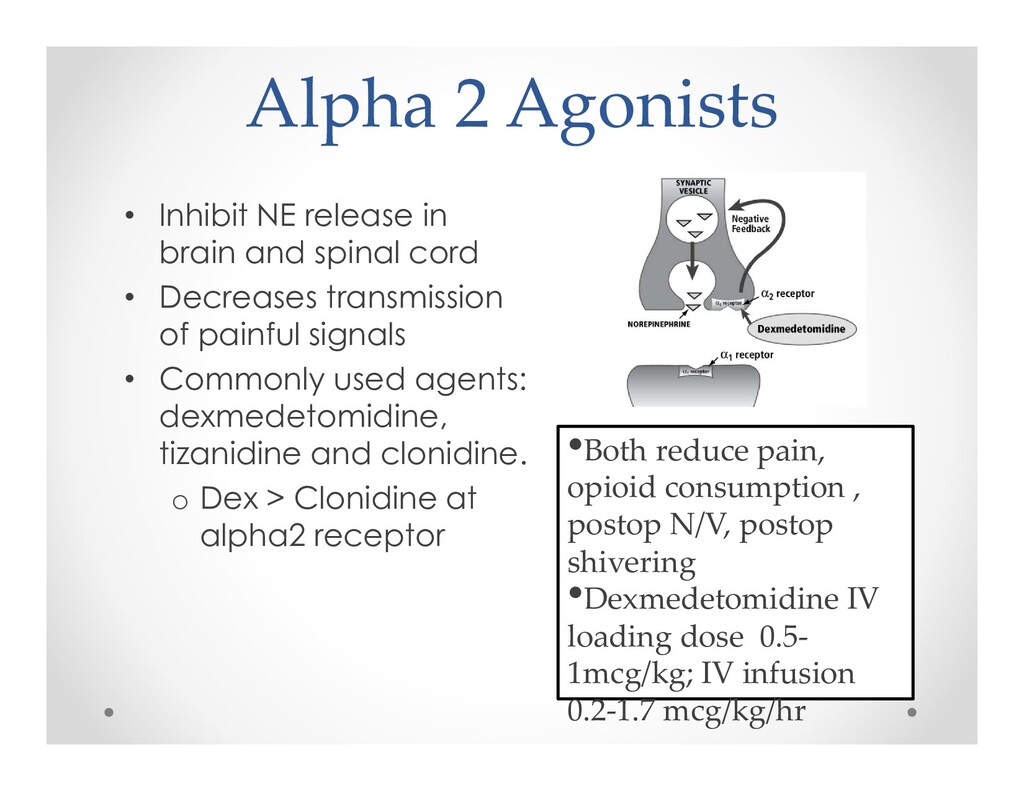
modulate ascending signals (inhibitory) • NE and 5-HT are key neurotransmitters • Central sensitization decreases inhibition of ascending pain pathways
Opioid prescribing and needs in thyroid and parathyroid surgery. JAMA. 2018;12:1098-1103. Education can be used to discuss potential adverse effects of opioids Also shown to reduce postop opioid consumption Expectations
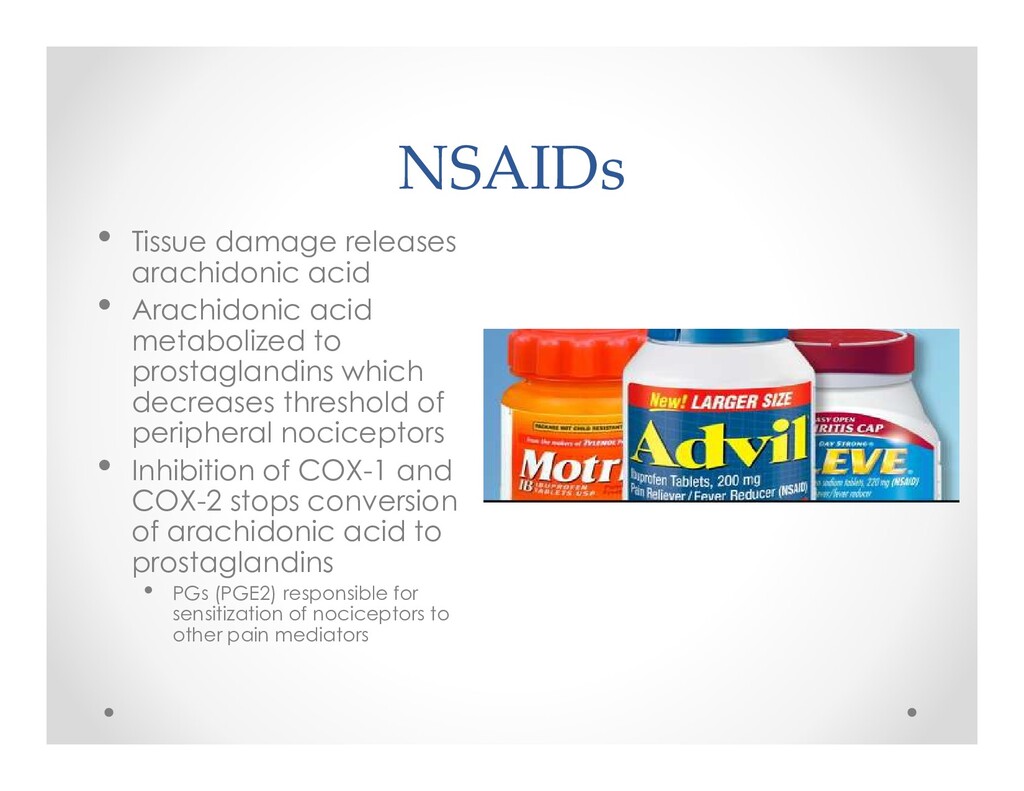
metabolized to prostaglandins which decreases threshold of peripheral nociceptors • Inhibition of COX-1 and COX-2 stops conversion of arachidonic acid to prostaglandins • PGs (PGE2) responsible for sensitization of nociceptors to other pain mediators
primary excitatory neurotransmitter in the CNS • Dose is sub-anesthetic (hallucinations uncommon) • Single doses 0.2-0.5 mg/kg IV given incrementally • Continuous IV infusions 0.1-0.2 mg/kg/hr.
in ortho and abdominal procedures • IV dose 0.1mg/kg, given preoperatively or shortly after induction seems optimal • Even single dose 4mg can increase blood sugar • Delayed wound healing with chronic usage • Can increase serum glucose levels by 50g/dL
impairment • Surgeon can administer • Depot forms may be beneficial? • IV Lidocaine – anti- inflammatory effects o Reduces pain scores and opioid usage, earlier return of bowel function o Mechanism of action is unclear
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}