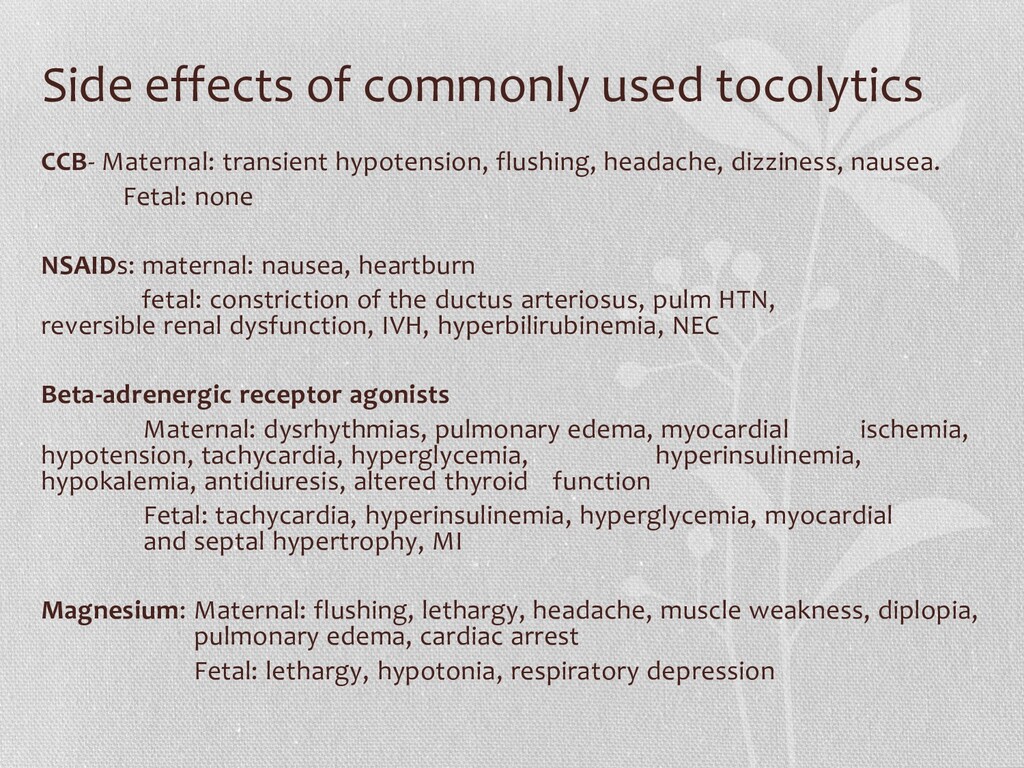
flushing, headache, dizziness, nausea. Fetal: none NSAIDs: maternal: nausea, heartburn fetal: constriction of the ductus arteriosus, pulm HTN, reversible renal dysfunction, IVH, hyperbilirubinemia, NEC Beta-adrenergic receptor agonists Maternal: dysrhythmias, pulmonary edema, myocardial ischemia, hypotension, tachycardia, hyperglycemia, hyperinsulinemia, hypokalemia, antidiuresis, altered thyroid function Fetal: tachycardia, hyperinsulinemia, hyperglycemia, myocardial and septal hypertrophy, MI Magnesium: Maternal: flushing, lethargy, headache, muscle weakness, diplopia, pulmonary edema, cardiac arrest Fetal: lethargy, hypotonia, respiratory depression
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}