This presentation explains the membranes of the fetus during pregnancy including Chorion and placenta, Amnion , Umbilical cord , & Yolk sac.
As well as the explanation of twins development and all the fetal periods
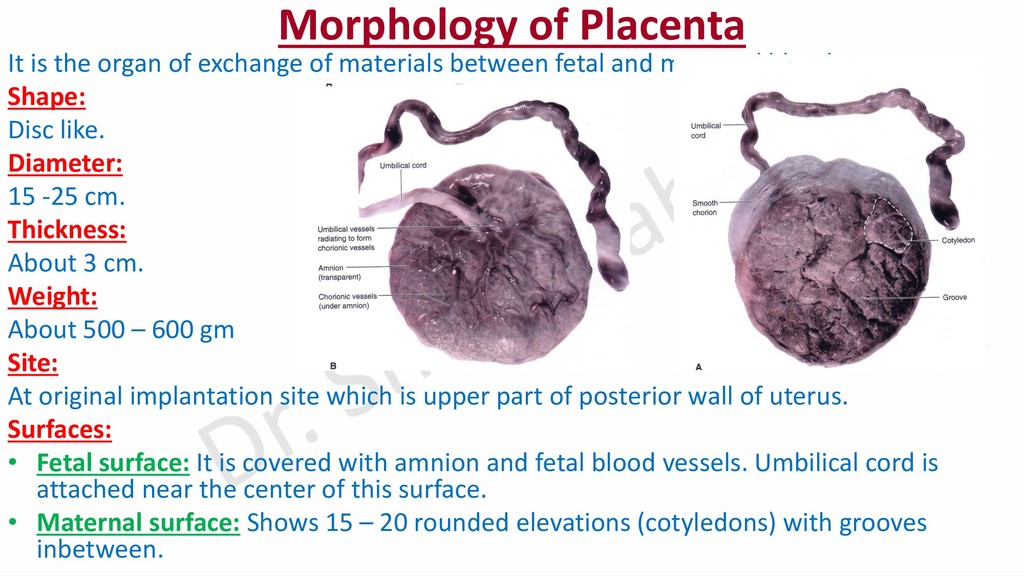
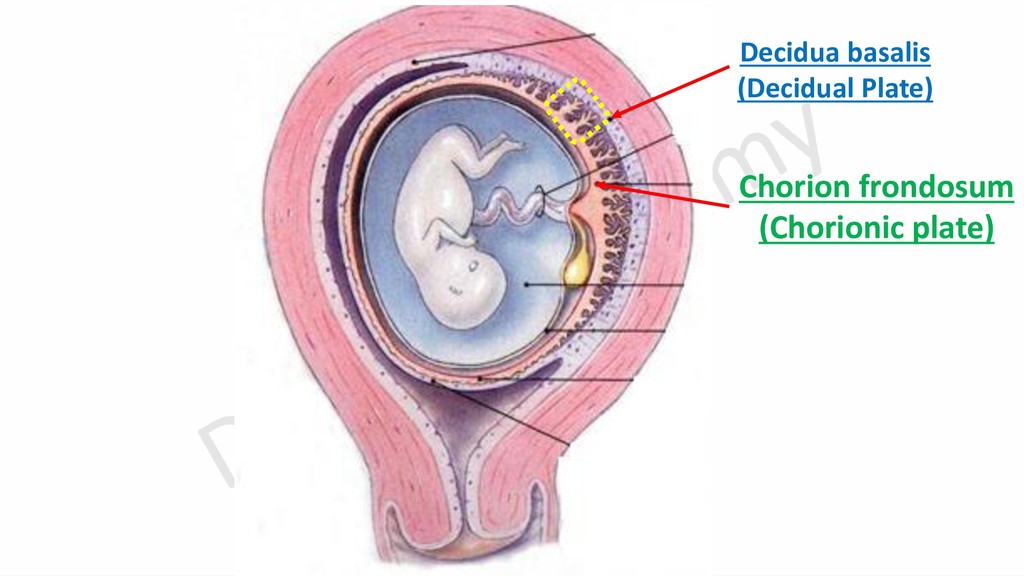
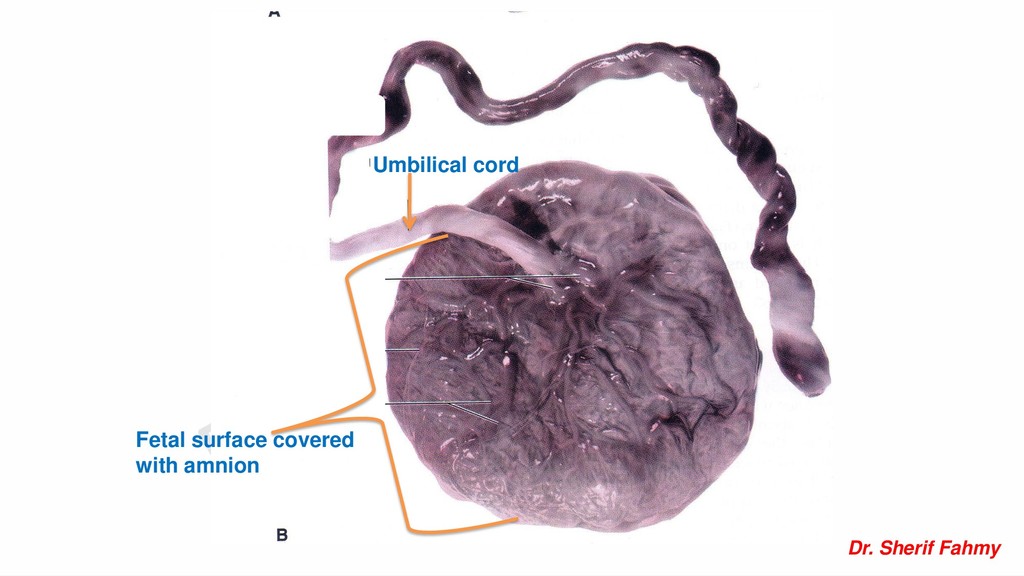
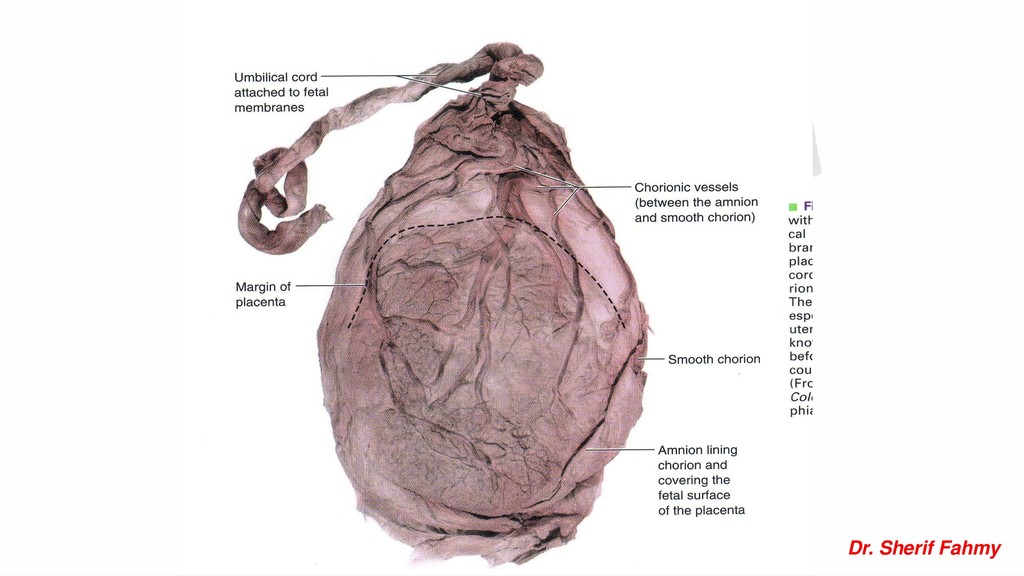
materials between fetal and maternal blood. Shape: Disc like. Diameter: 15 -25 cm. Thickness: About 3 cm. Weight: About 500 – 600 gm Site: At original implantation site which is upper part of posterior wall of uterus. Surfaces: • Fetal surface: It is covered with amnion and fetal blood vessels. Umbilical cord is attached near the center of this surface. • Maternal surface: Shows 15 – 20 rounded elevations (cotyledons) with grooves inbetween.
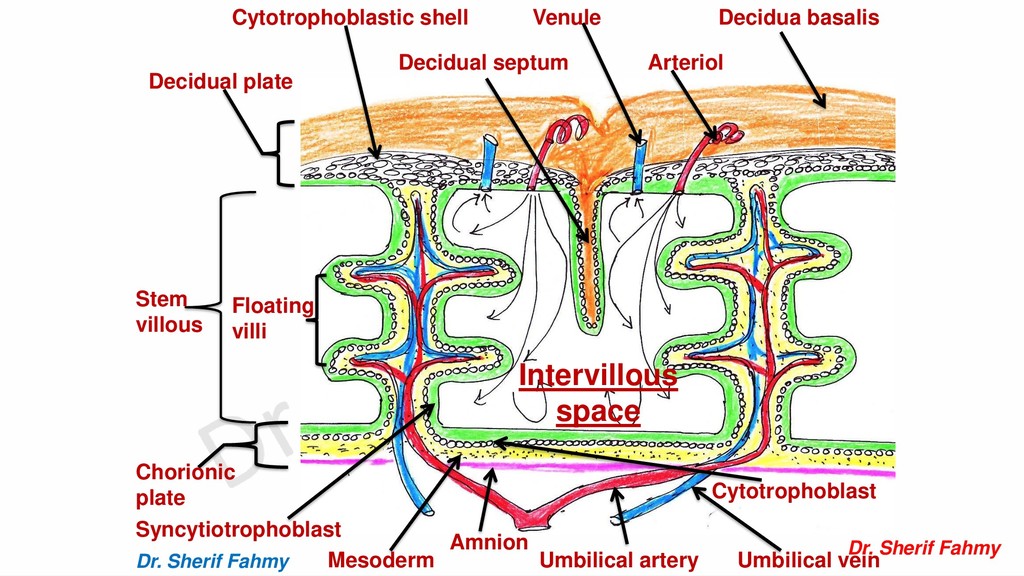
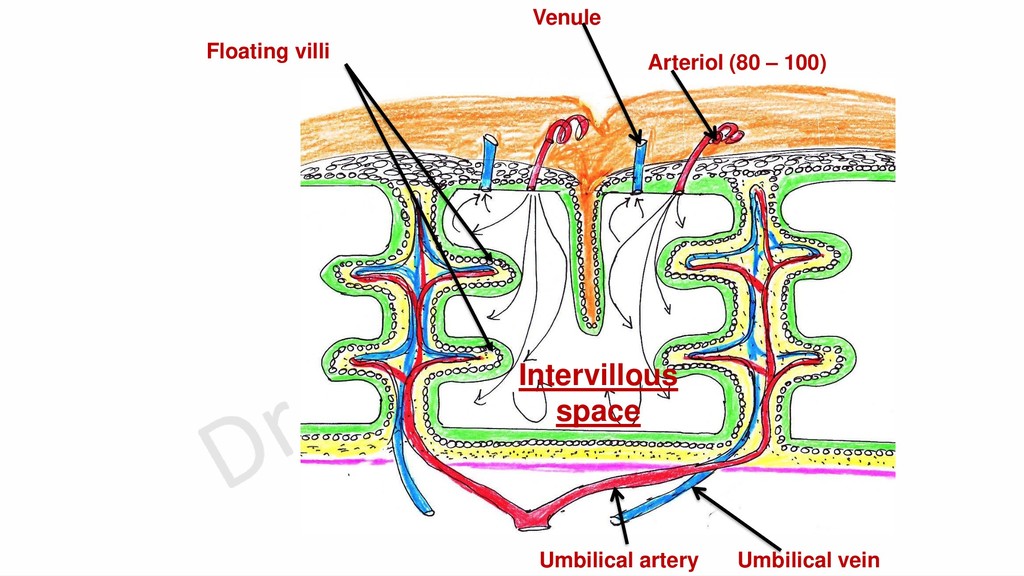
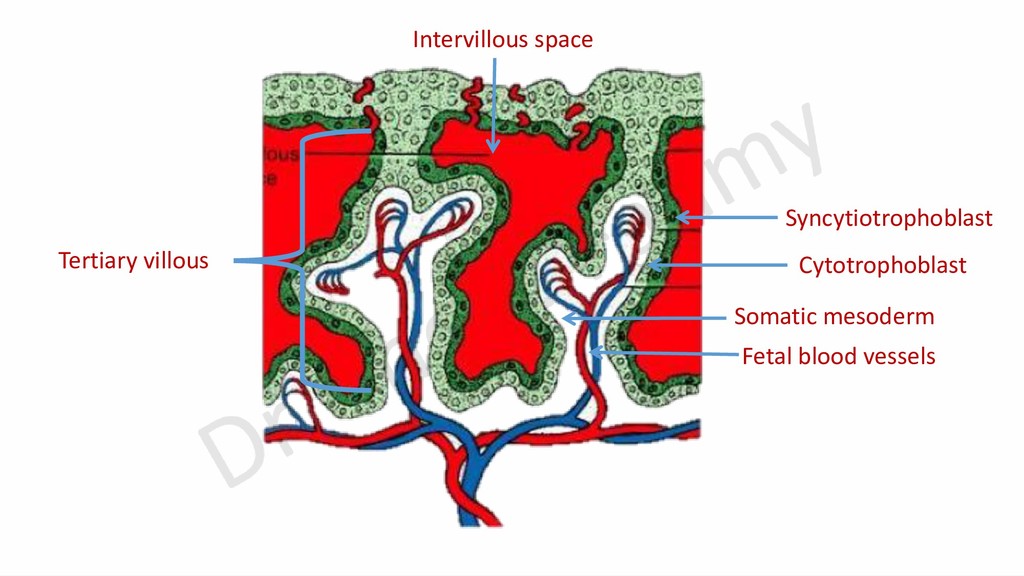
blood. Structure: 1- Syncytiotrophoblast. 2- Cytotrophoblast. 3- Extraembryonic mesoderm. 4- Endothelium of fetal blood vessels. Functions of the barrier: 1- Separates between fetal and maternal blood. 2- Prevents passage of bacteria, most viruses and damaging factors. 3- Permites gaseous and nutritive exchange. Disappear in 2nd ½ of pregnancy
antibodies starting from 14th week. 3- Production of hormones as progesterone, estrogen, HCG and somatomammotropin 4- Barrier against bacteria and most of viruses. 5- Excretory function as it excretes urea and creatinine.
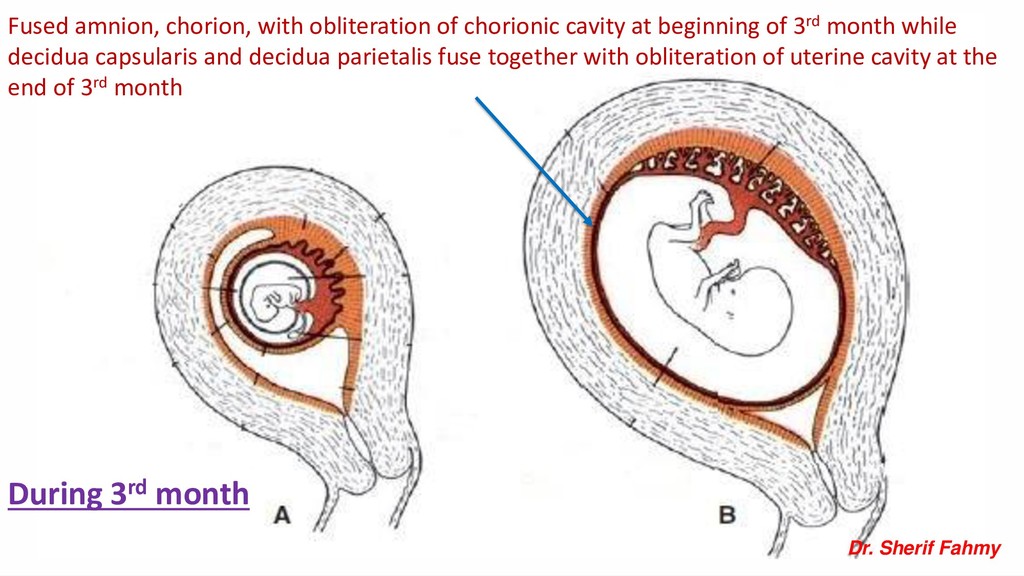
of 3rd month while decidua capsularis and decidua parietalis fuse together with obliteration of uterine cavity at the end of 3rd month During 3rd month Dr. Sherif Fahmy
cc Constituents: - Clear watery fluid, rich with electrolytes, protein, lipids, carbohydrate and stem cells at full term. Source: Starts formation from amnioblast and by osmosis from maternal blood, then from kidney.
as water cushion that absorbs external shocks. 2- Acts as heat insulator. 3- Prevents adhesion of embryo to wall of uterus. 4- Prevents adhesion of fetal parts. 2- At late pregnancy: 1- Give a space to allows fetal movements that help body muscles to develop. 2- Give a space for accumulated urine 3- Help suckling training and development of gut muscles.
of bag of water that gradually dilate the cervix. 3- Rupture of amniotic sac is a sign of start of delivery. 4- Sterile amniotic washes vagina before passage of baby. 4- Amniotic fluid & stem cells: Amniotic fluid is a source of stem cells.
(35 %). 2- Maternal diabetes. 3- Congenital malformation e.g. anencephaly and esophageal atresia. 2- Oligohydramnios. Cause: -Renal agenesis. 3- Premature rupture of amniotic sac: It is a common cause of preterm labor.
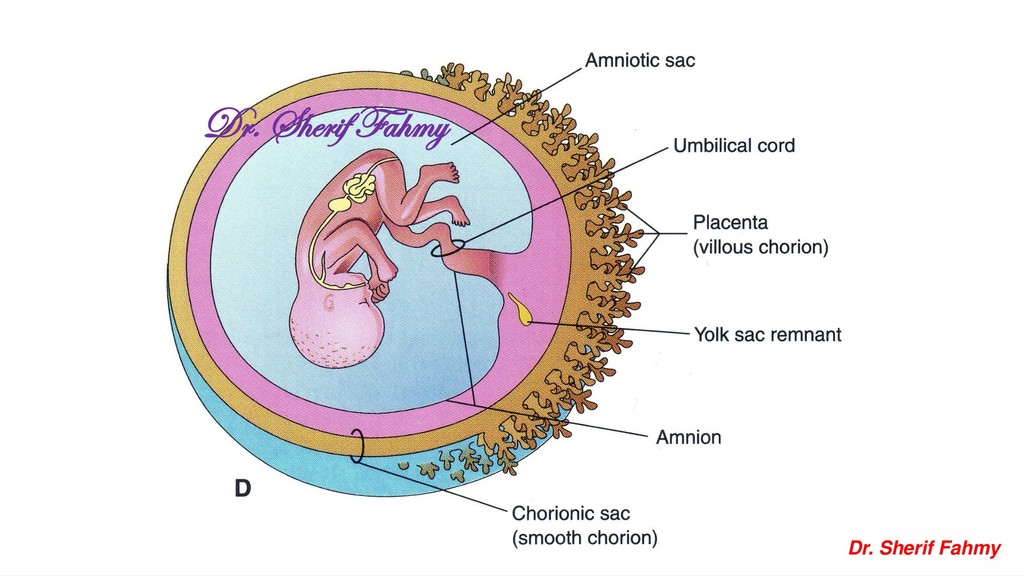
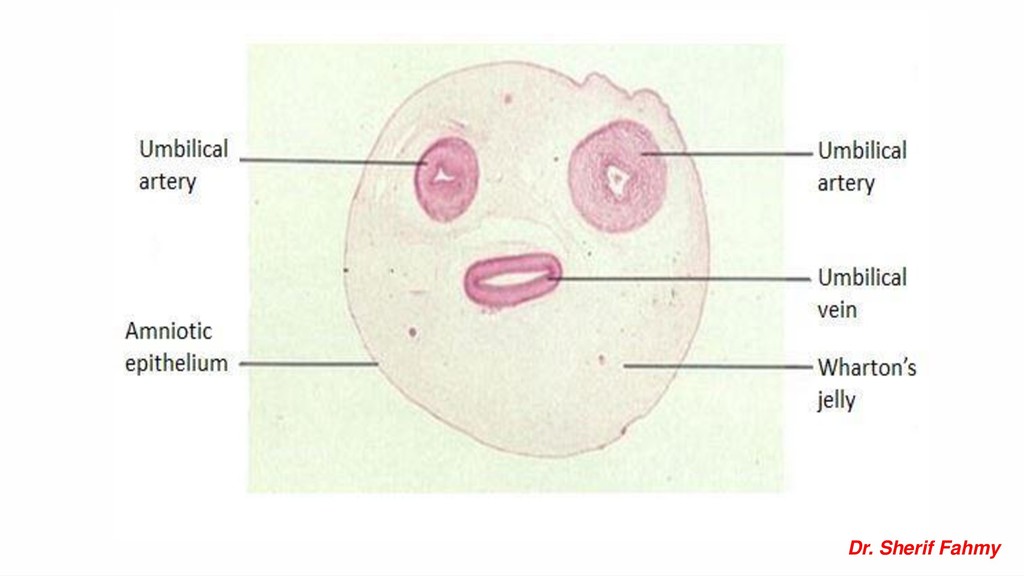
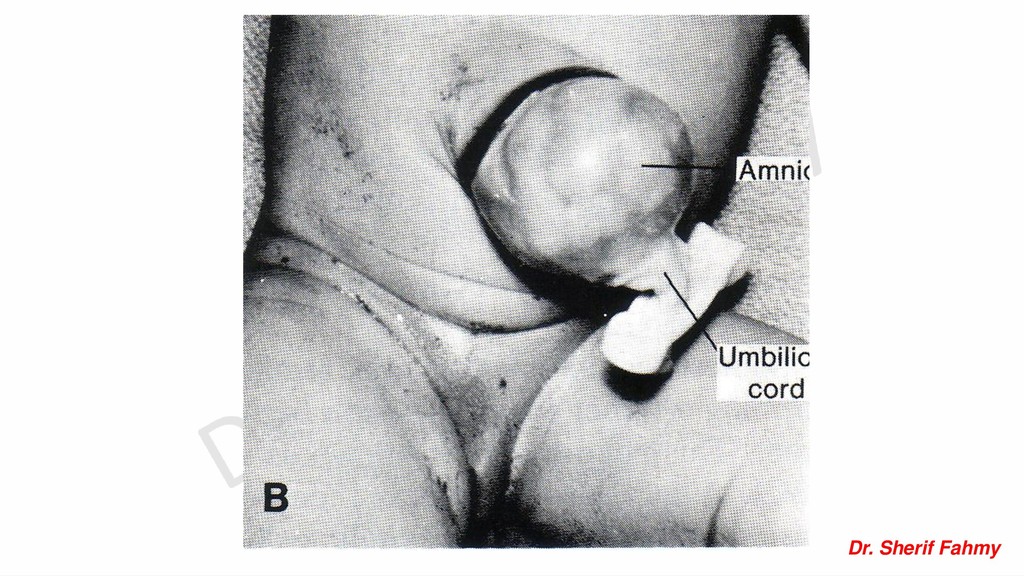
placenta and fetus. Length: 50 – 60 cm Diameter: 2 cm. Shape: Tortous, showing false knots. Contents: 2 umbilical arteries, one umbilical vein embedded in wharton’s jelly and surrounded by amniotic membrane. Attachments: It is attached to fetal surface of placenta near its center, the other attachment is to ventral aspect of fetal abdominal wall. Functions: – It contains umbilical vessels that connect the fetus to the placenta. – Allows free mobility of the fetus.
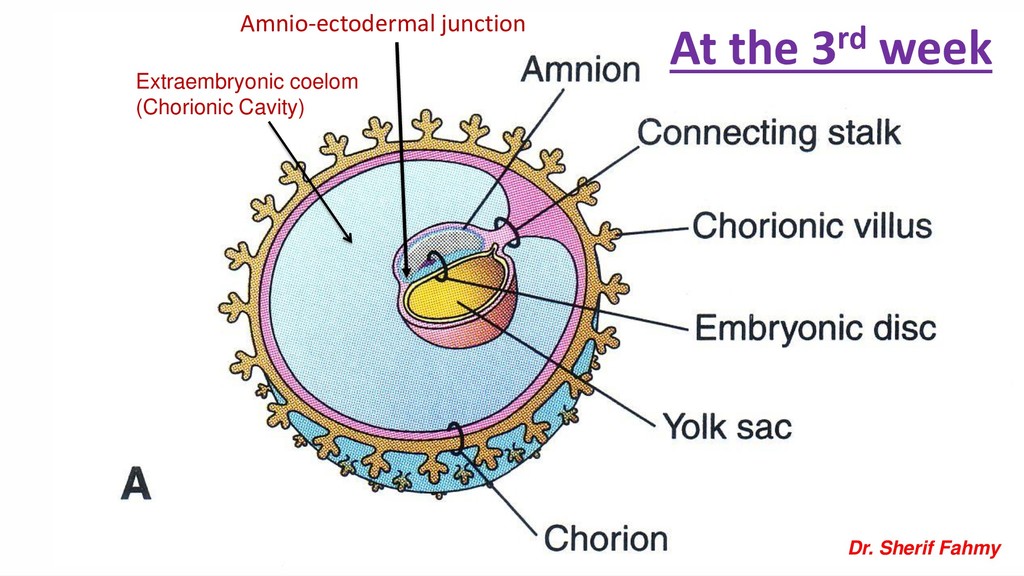
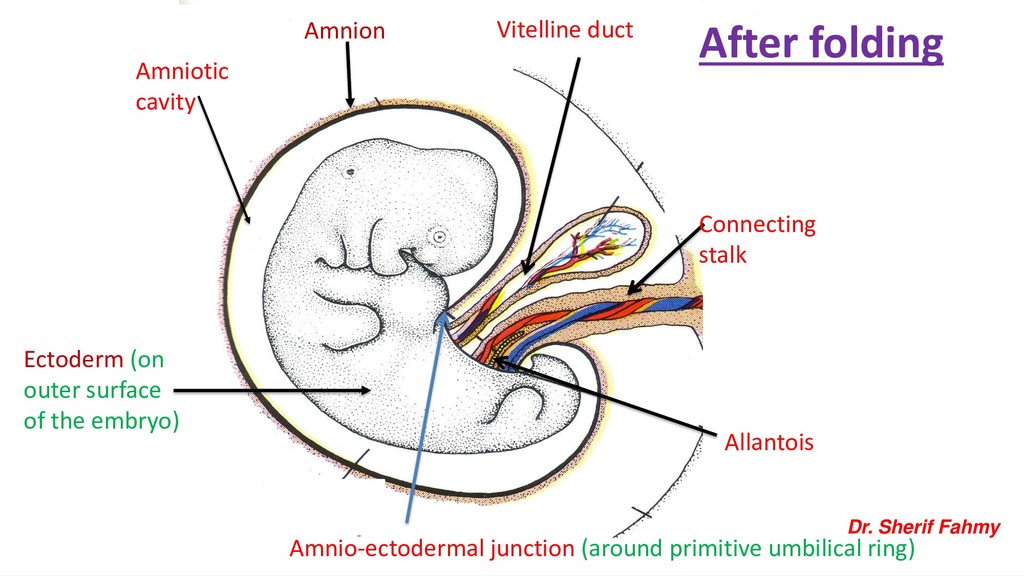
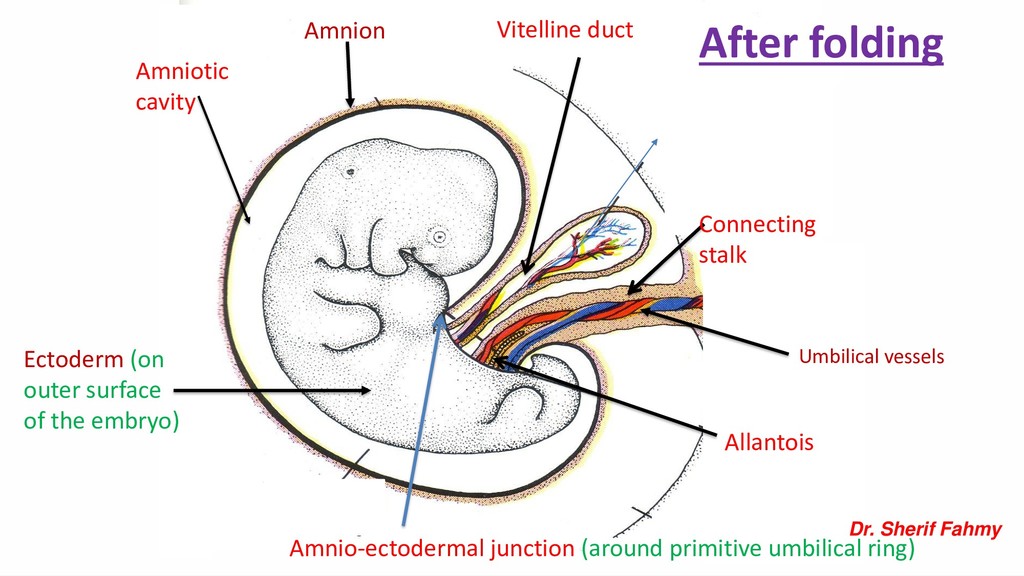
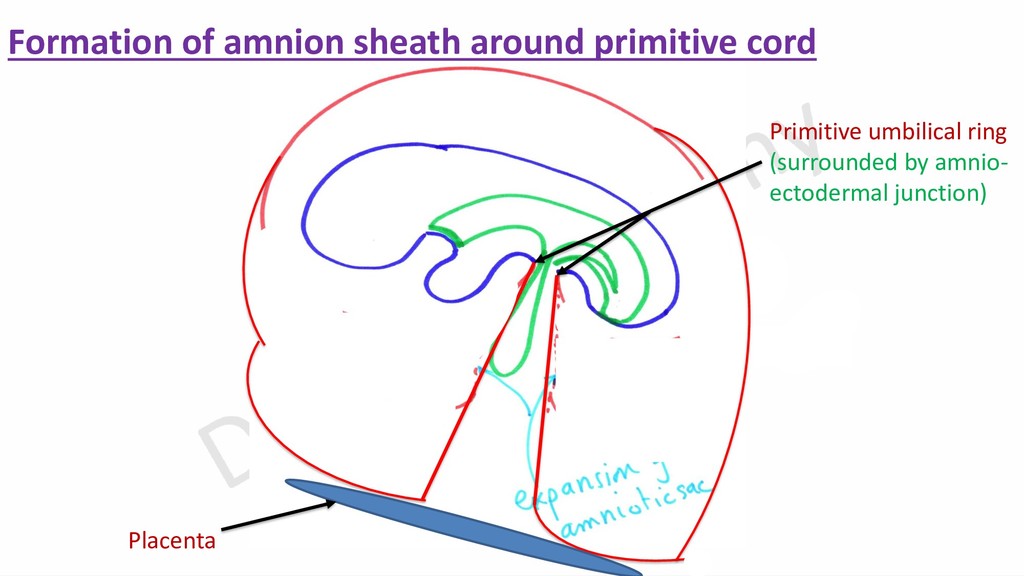
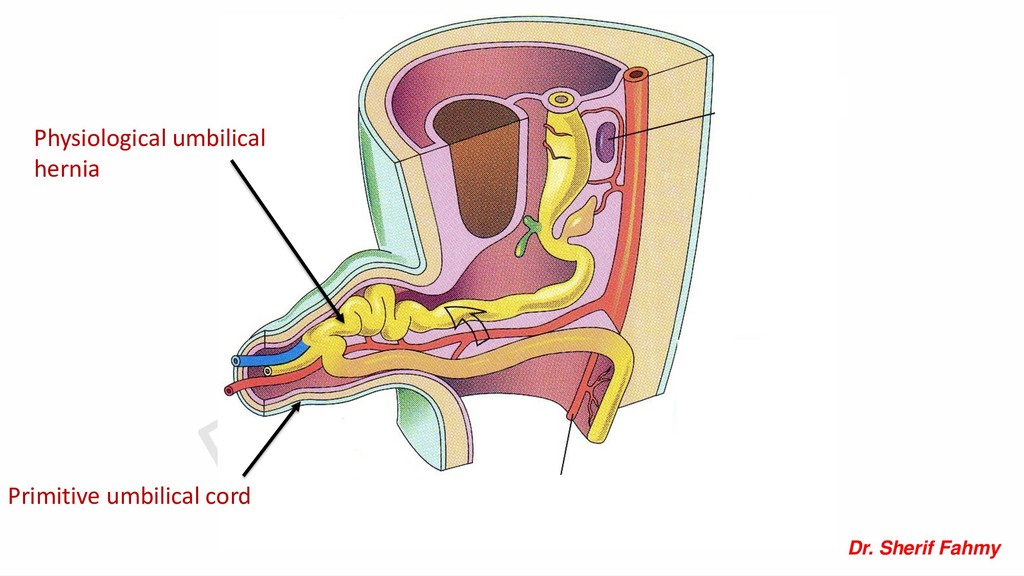
sheath of amnion around the structures that pass through the primitive ring with formation of primitive umbilical cord. Contents: 1- Yolk sac and vitelline duct. 2- Connecting stalk with remnant of allantois. 3- Umbilical and vitelline vessels. 4- Intestinal loop in its proximal part. Primitive umbilical cord
➢Obliteration of extra-embryonic part of vitelline vessels and one umbilical vein with persistence of other vein (left vein) and 2 umbilical arteries. ➢ Degeneration of vitelline duct, yolk sac and most of allantois. ➢ Transformation of mesoderm of connecting stalk into Wharton’s jelly. Definitive Umbilical Cord
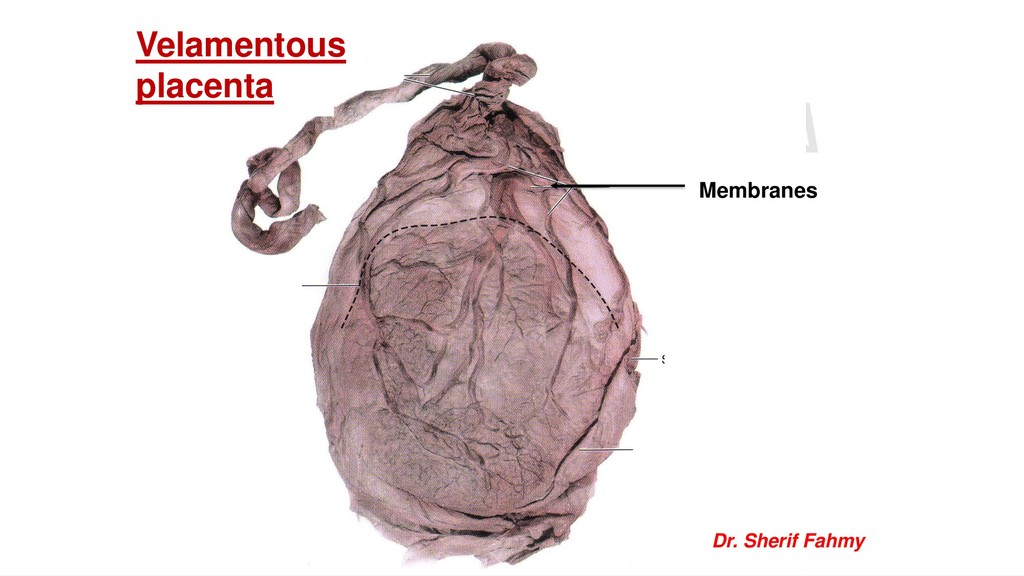
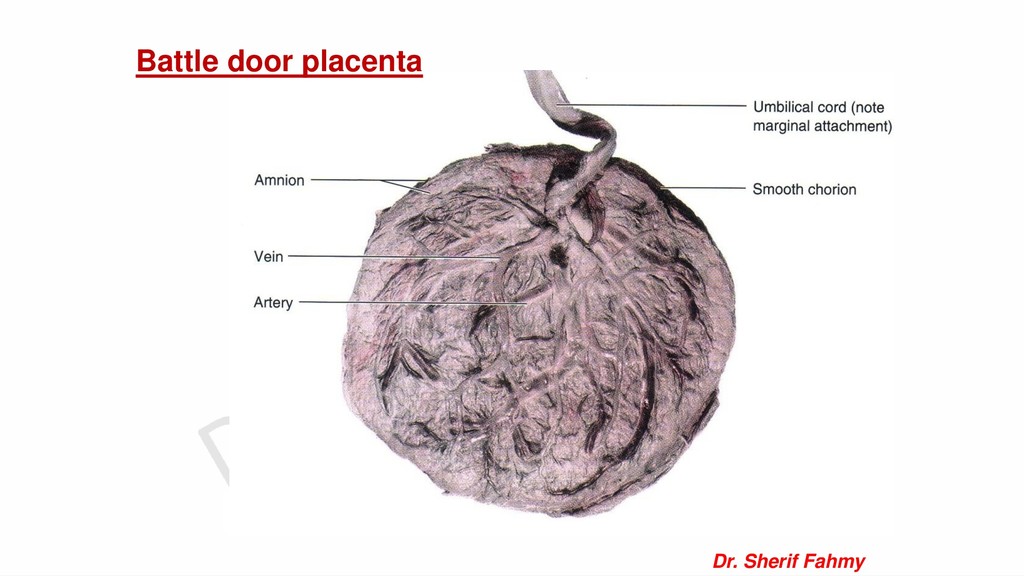
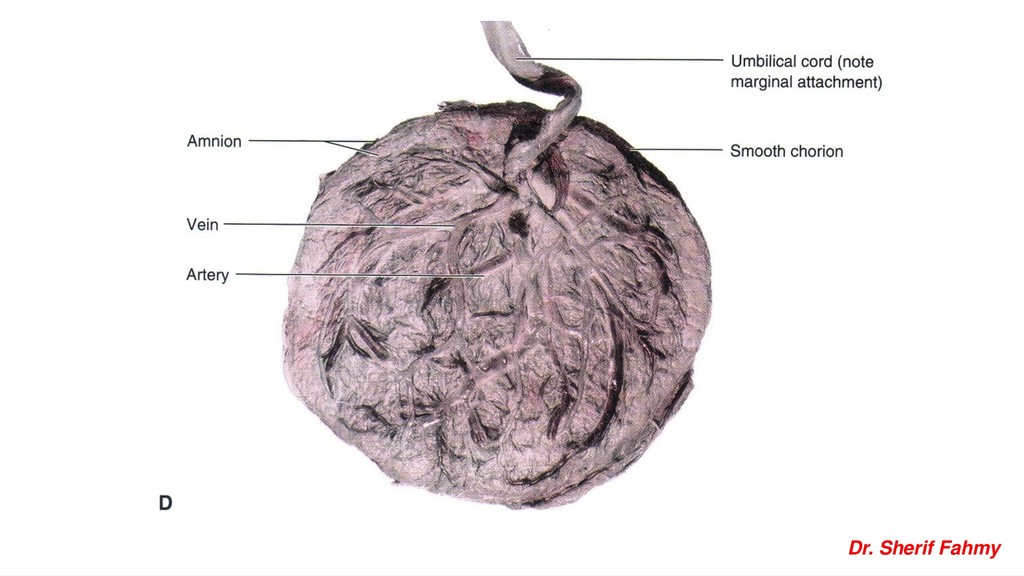
delivery of the baby. 2- Long cord: It may encircle neck of fetus and may form true knots. 3- Congenital umbilical hernia (omphalocele): the cord contains coils of intestine. 4- Presence of one umbilical artery. 5- Abnormal attachment of the cord: –Marginal attachment (battledore) –Through membranes (velamentous).
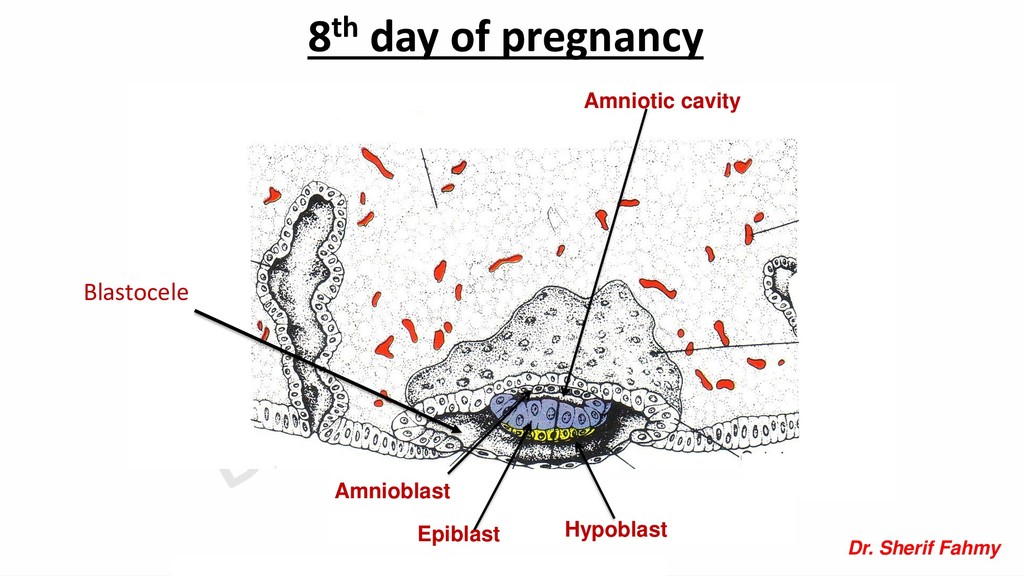
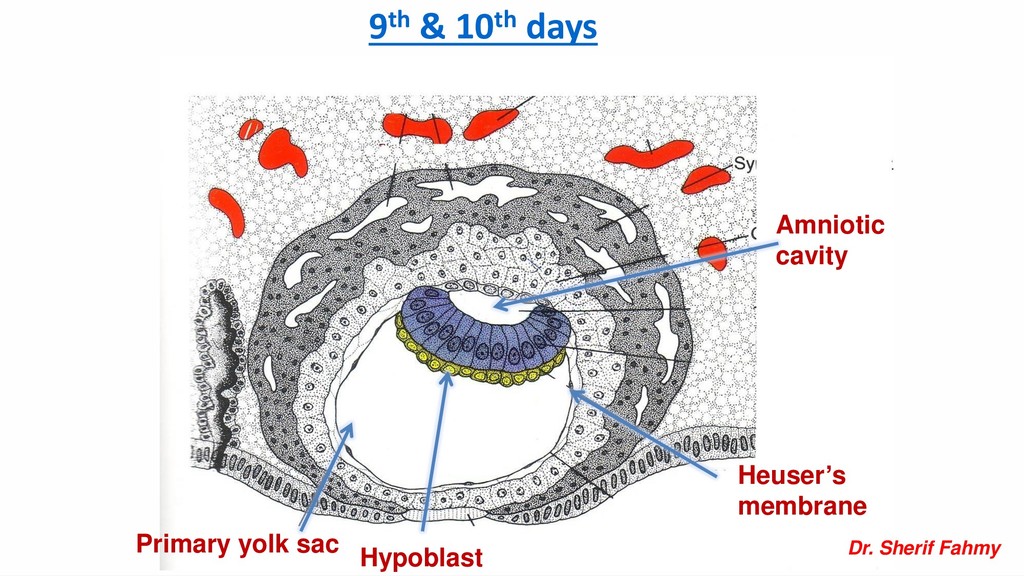
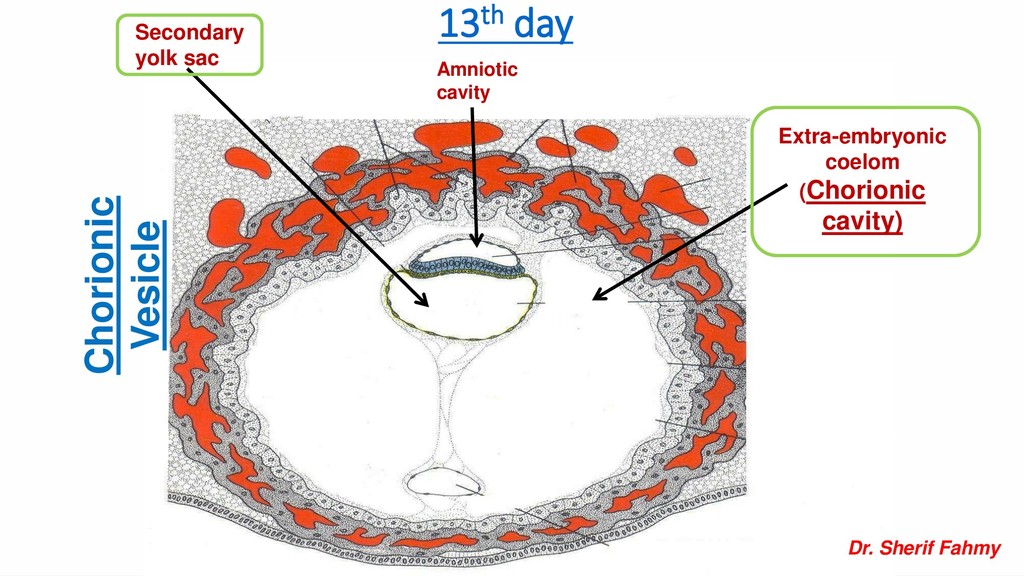
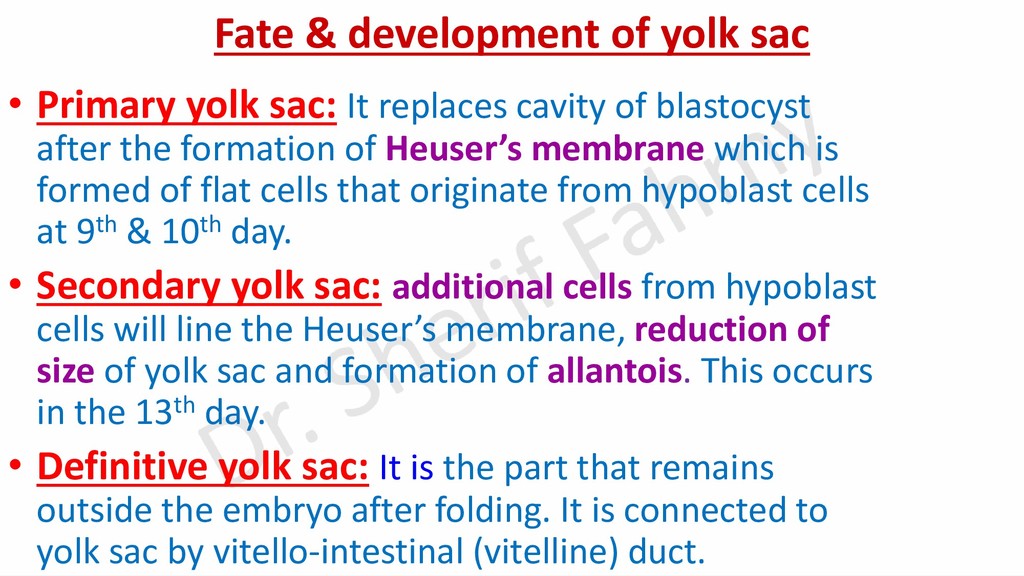
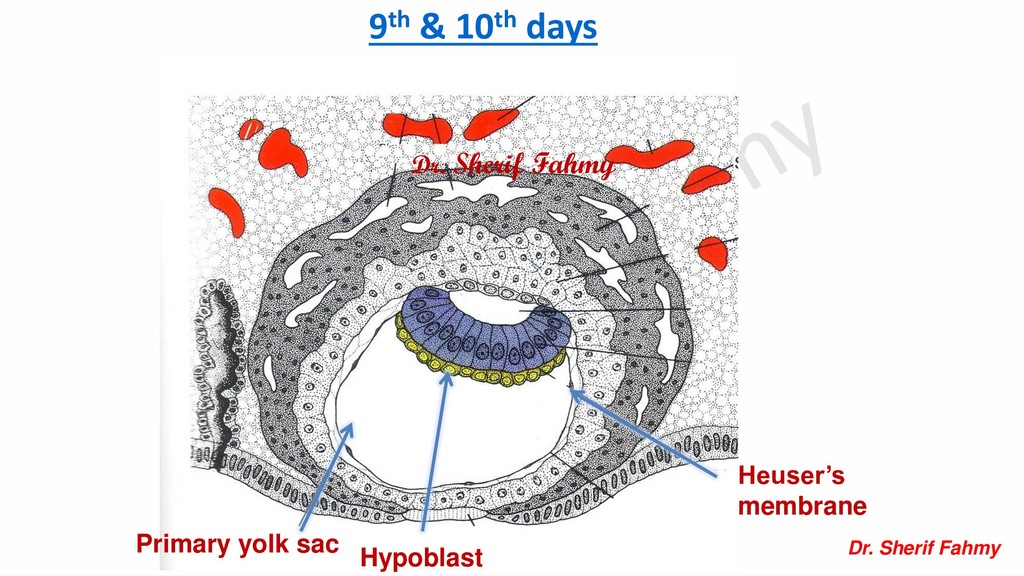
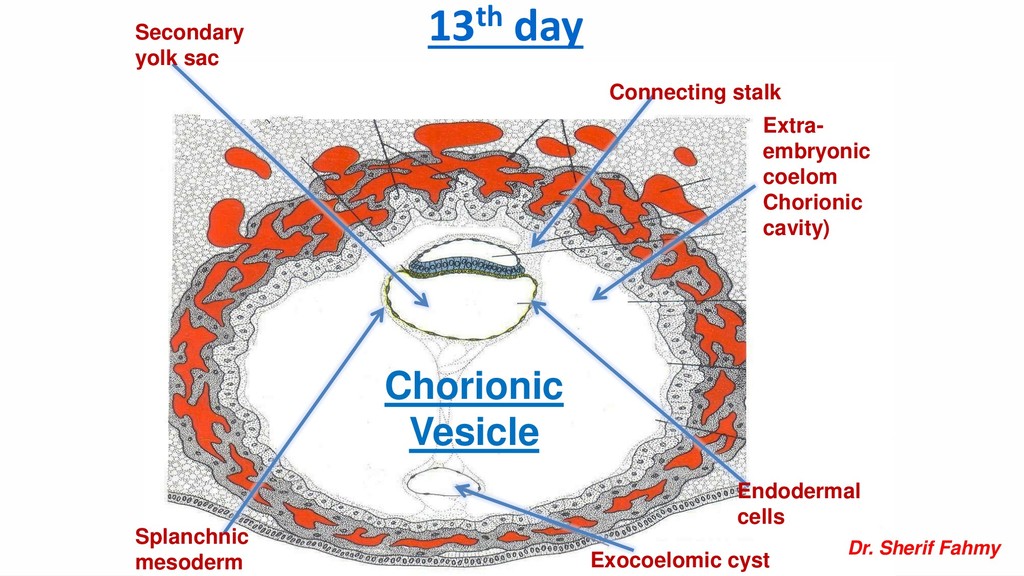
It replaces cavity of blastocyst after the formation of Heuser’s membrane which is formed of flat cells that originate from hypoblast cells at 9th & 10th day. • Secondary yolk sac: additional cells from hypoblast cells will line the Heuser’s membrane, reduction of size of yolk sac and formation of allantois. This occurs in the 13th day. • Definitive yolk sac: It is the part that remains outside the embryo after folding. It is connected to yolk sac by vitello-intestinal (vitelline) duct.
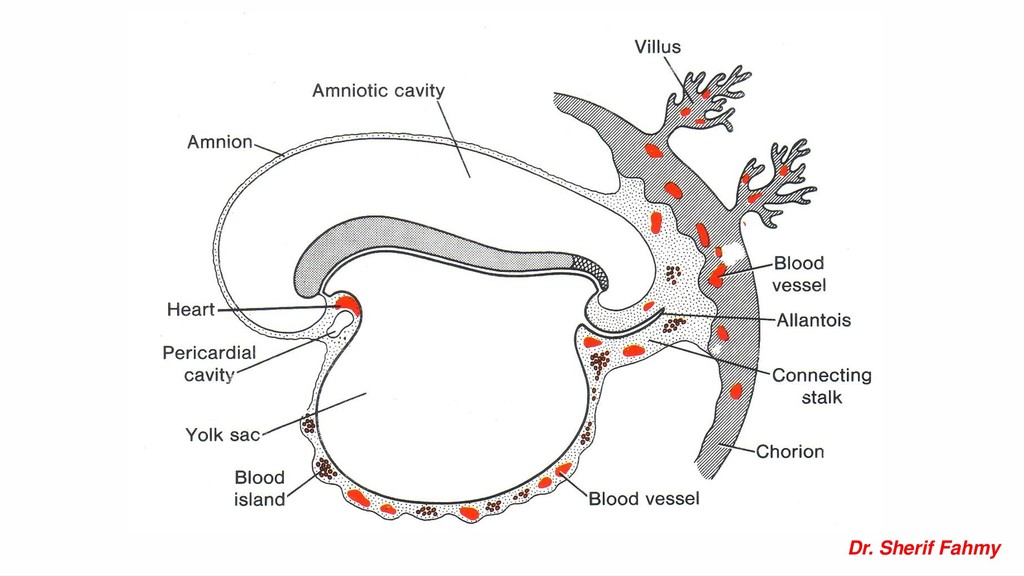
• Allantois: forms part of urinary bladder. • Primordial germ cells: Which are spermatogonia and oogonia which are formed in its caudal part (hind gut). • Vitelline vessels: develop from mesoderm around vitelline duct. Intra-embryonic part form portal vein and arteries of intestine. • Blood cells: develop in the mesoderm around the yolk sac.
type as it represent 2/3 of twins and 7 – 11 / 1000 births. - Fertilization of 2 separate ova. - Each embryo has its own amniotic cavity, chorion and placenta. - Twins are non-identical and may of same sex or different.
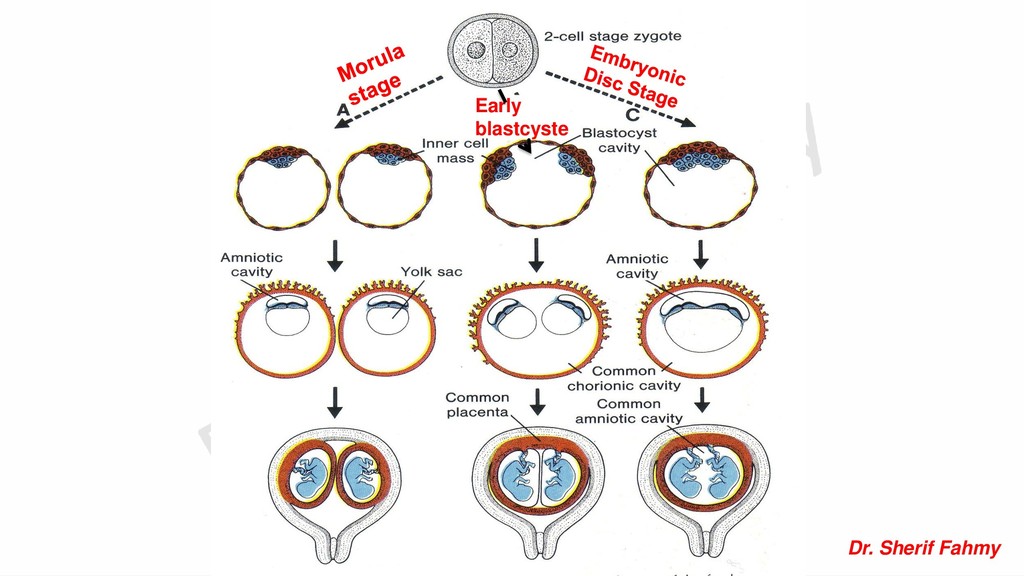
Twins of this type are identical and of same sex. Its incidence is 0.3 – 0.4 % Division may occur at 3 different stages: 1- At morula stage: Twins has separate amnion, chorion and placentae (as in dizygotic). 2- At blastocyst stage: due to division of inner cell mass. Twins has separate amniotic cavity but single chorion and placenta. 3- At embryonic disc: Midline division of the embryonic disc. Twins has common amniotic cavity, common chorion and common placenta .
incomplete separation of embryonic disc. They could be either: Craniopagus: Fusion between 2 heads. Thoracopagus: Fusion at thoracic region. Pygopagus: Fusion at the pelvic region.
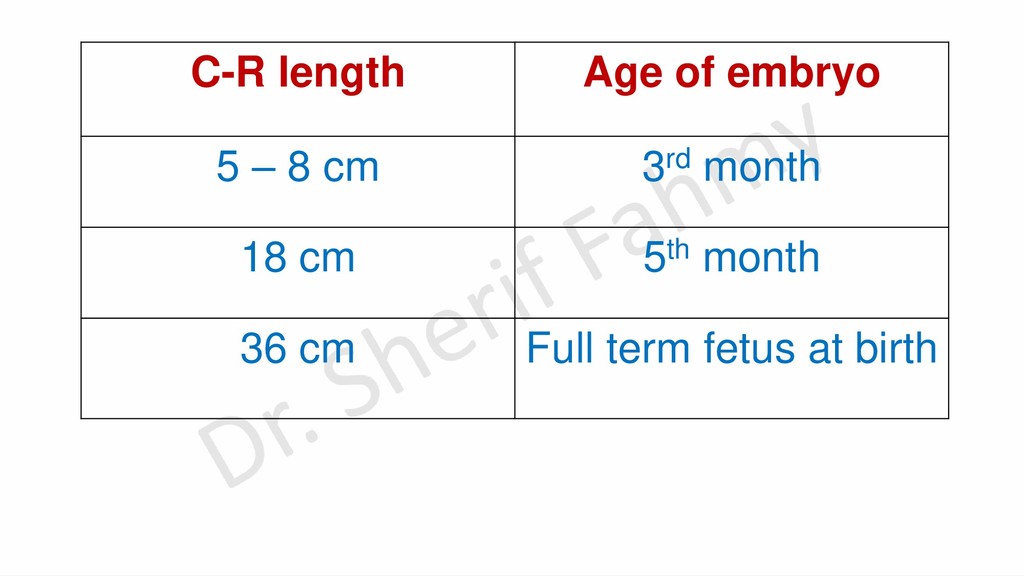
the 3rd month, the head is ½ the CR length. -At the beginning of the 5th month, the head is 1/3 the CH length. -At birth, the head is ¼ of CH length. Weight growth: -At the end of 5th month, the weight is ½ kg. -At the 7th month, the weight is 1.75 kg. -At full term, the weight is 3.5 kg.
longer. -External genitalia are differentiated at 12th week. -Lanugo hair covers the fetus since the 4th month. -The skin is wrinkled till the end of 6th month. -Testes descend to scrotum just before birth. -Skin is covered by fatty substance called Vernix caseosa Fetal movement: It is clearly recognized since the 5th month. Time of birth (expected day of delivery) ➢ 280 days from 1st day of last menstruation. ➢ 266 days from day of fertilization (day of ovulation = 14 days after 1st day of menstruation).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}