2015 Page 21 & Third Quarter 2016 Page 42 Question: A patient with diabetes mellitus was admitted when she was found to be lethargic. Her blood sugar readings were low. Discharge diagnosis was documented as acute encephalopathy secondary to hypoglycemia. What are the diagnosis code assignments for encephalopathy due to hypoglycemia in a diabetic patient? Answer: Assign code E11.649, Type 2 diabetes mellitus with hypoglycemia without coma, as the principal diagnosis. Assign also code G93.41, Metabolic encephalopathy, as an additional diagnosis. Question: The Central Office has received several requests to clarify advice published in Coding Clinic, Third Quarter, 2015, page 21, about encephalopathy due to diabetic hypoglycemia. When the terms "encephalopathy, hypoglycemic" are referenced, the Index directs to code E16.2, Hypoglycemia. Additionally, there was no recommendation to query the provider regarding the underlying cause, which could be due to insulin or another hypoglycemic agent; and there was no mention of metabolic encephalopathy in the question. Answer: Codes E11.649, Type 2 diabetes mellitus with hypoglycemia without coma, and G93.41, Metabolic encephalopathy, are the correct code assignments for metabolic encephalopathy due to diabetic hypoglycemia. The fact that the provider specifically documented "metabolic encephalopathy" in his final diagnostic statement was inadvertently omitted from the published question. Although the Index directs to code E16.2, Hypoglycemia, unspecified, under "encephalopathy, hypoglycemic," code E16.2 is not appropriate as it refers to nondiabetic hypoglycemia. In addition, the patient had taken his antidiabetic medication as prescribed and there was no indication in the health record of adverse effect, underdosing, and/or poisoning.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
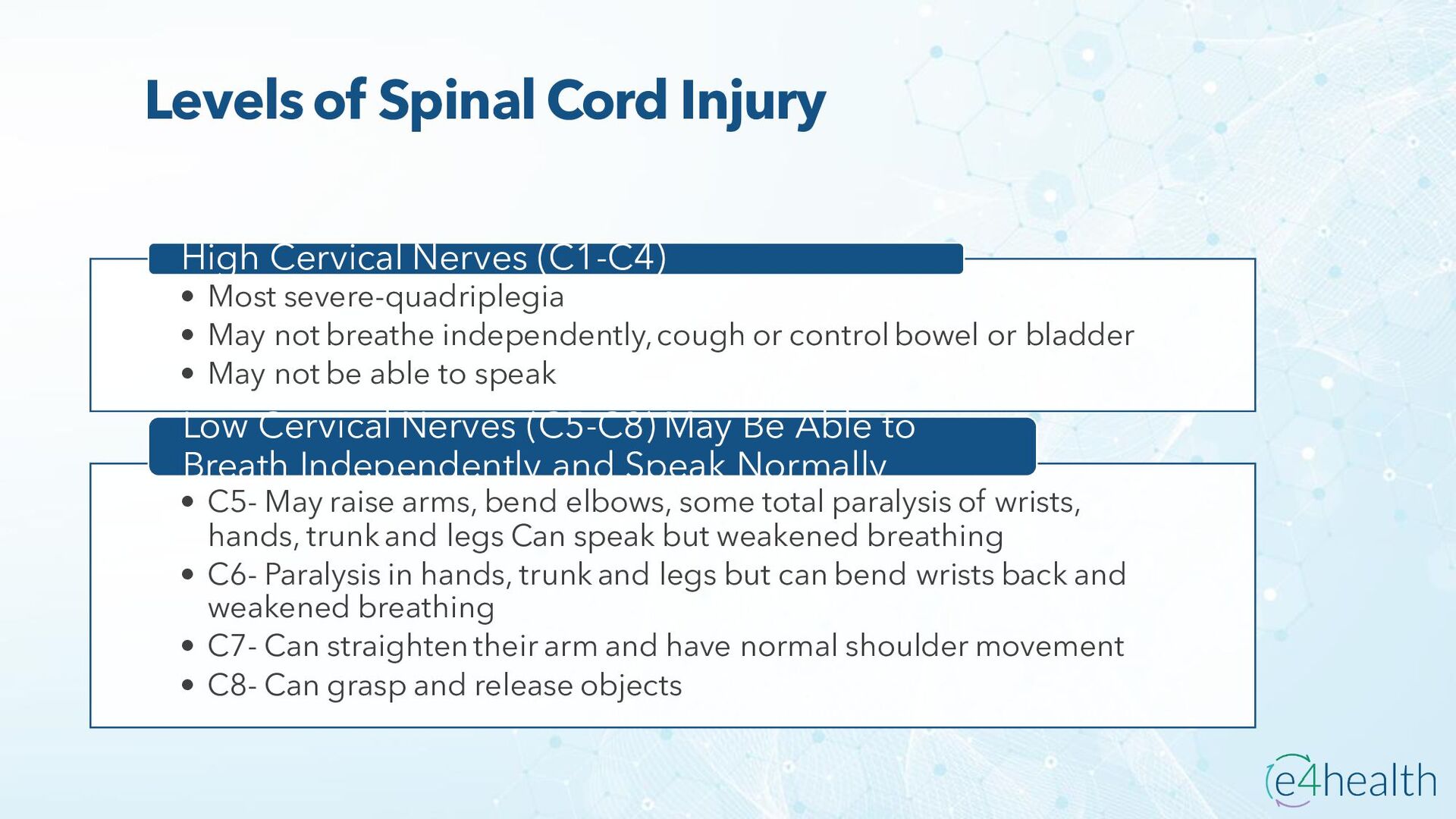
![SPINAL CORD INJURY Figure 1. Neana N. (2014) SlideShare [image]](https://files.speakerdeck.com/presentations/94aa7f505ac14fc391d92483c0ca65f6/slide_23.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}