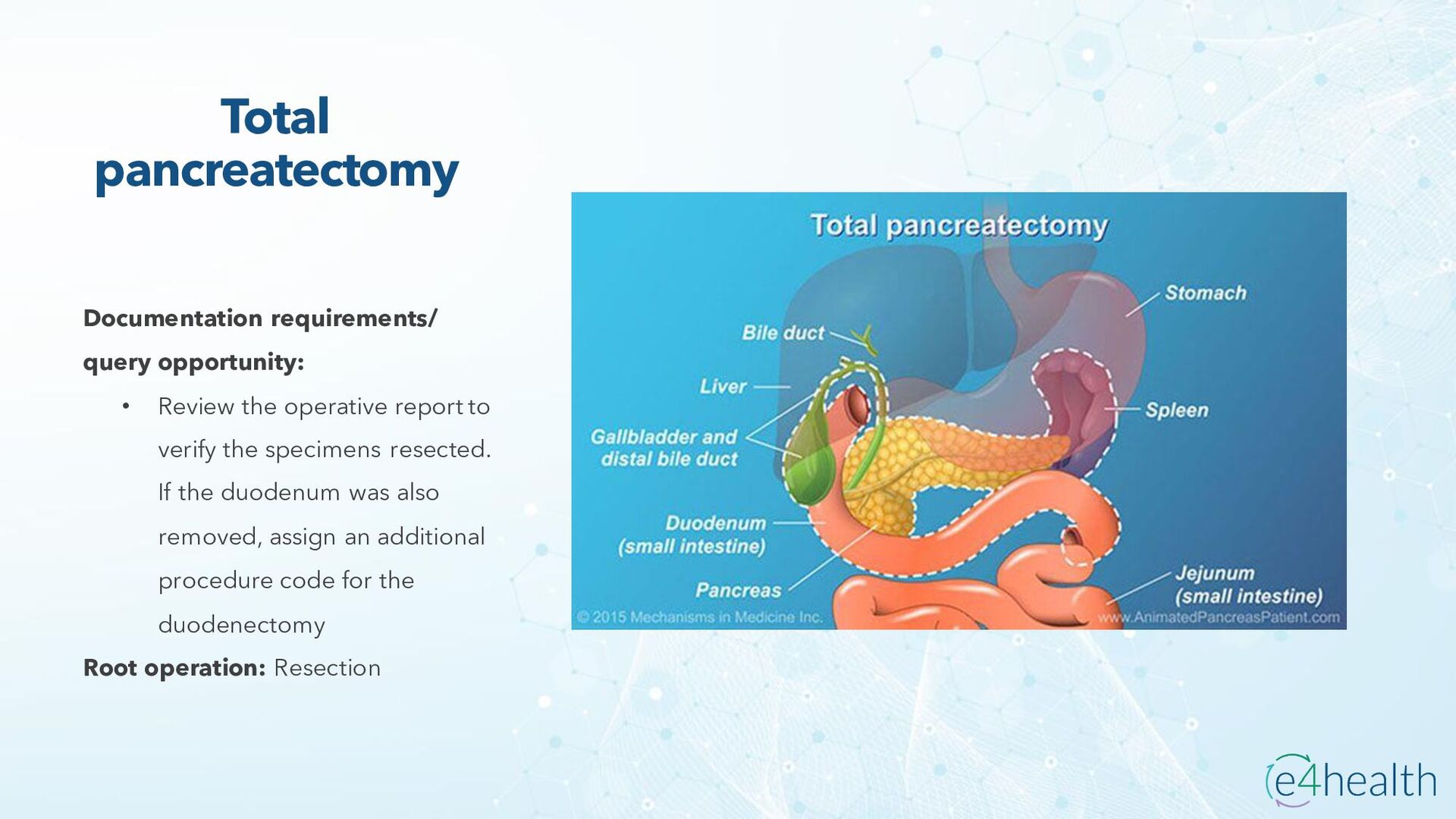
surgery performed as treatment primarily for pancreatic cancer, but may also be performed to treat pancreatitis, ampullary cancer, bile duct cancer, neuroendocrine tumors and/or trauma to the pancreas or small intestine. The intent is to remove the head of the pancreas, where most tumors occur. However, because the pancreas is so integrated with other organs, the duodenum (which includes the ampulla of Vater), gallbladder, a portion of the common bile duct and sometimes a portion of the stomach must also be removed. Anastomosis of the remaining organs to allow for normal digestive function is necessary at the completion of the procedure. The anastomosis performed is inherent o the total surgery and is not coded separately. Whipple procedures may be performed via an open approach (more common), laparoscopically and with or without robotic assistance. There are two general types of Whipple procedures: • Conventional, in which typically the head of the pancreas, entire duodenum, gallbladder, portion of the stomach and portion of the common bile duct are removed. • Pylorus sparing, in which the pylorus is preserved and no portion of the stomach is removed, sustaining the function of the gastric reservoir and allowing more normal gastric emptying. The main advantage is the likelihood of better nutritional status postoperatively, and less complicated surgical reconstruction. • When documentation supports a liver biopsy was performed, the operative report should be reviewed thoroughly to determine if a liver incision was done (hepatotomy), closure of a laceration was required, or a wedge resection was done rather than punch biopsy. All these procedures will result in assignment here (MS-DRGs 405/406/407). Punch, open and closed biopsy only are assigned to MS-DRGs 420/421/422.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}