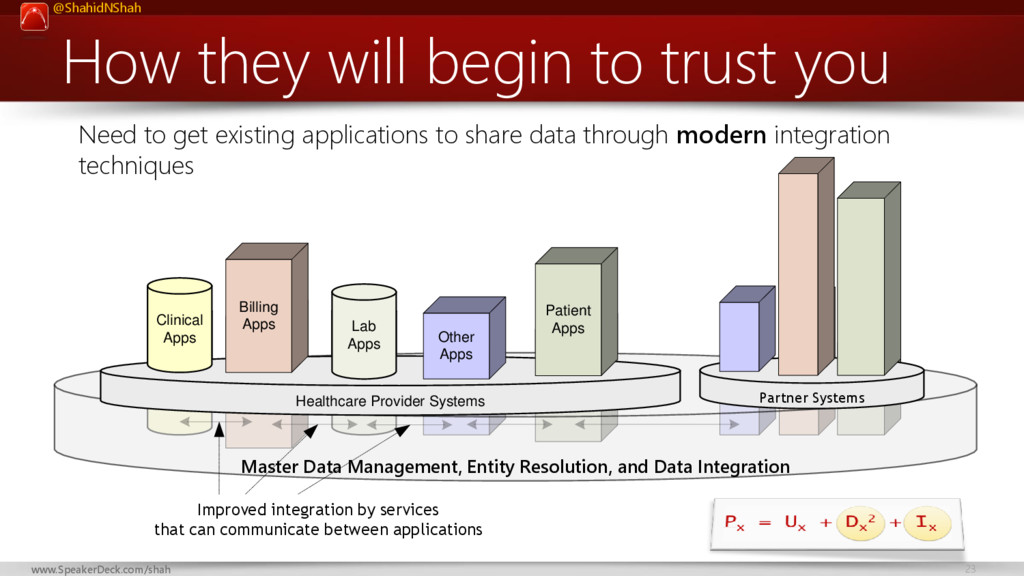
At HxRefactored 2016 Shahid presented the following formula:
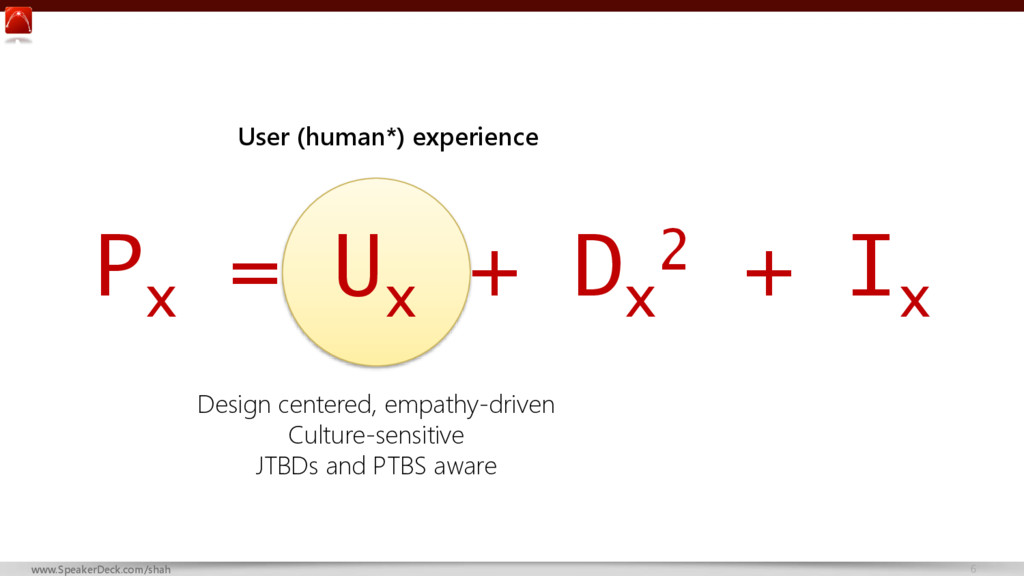
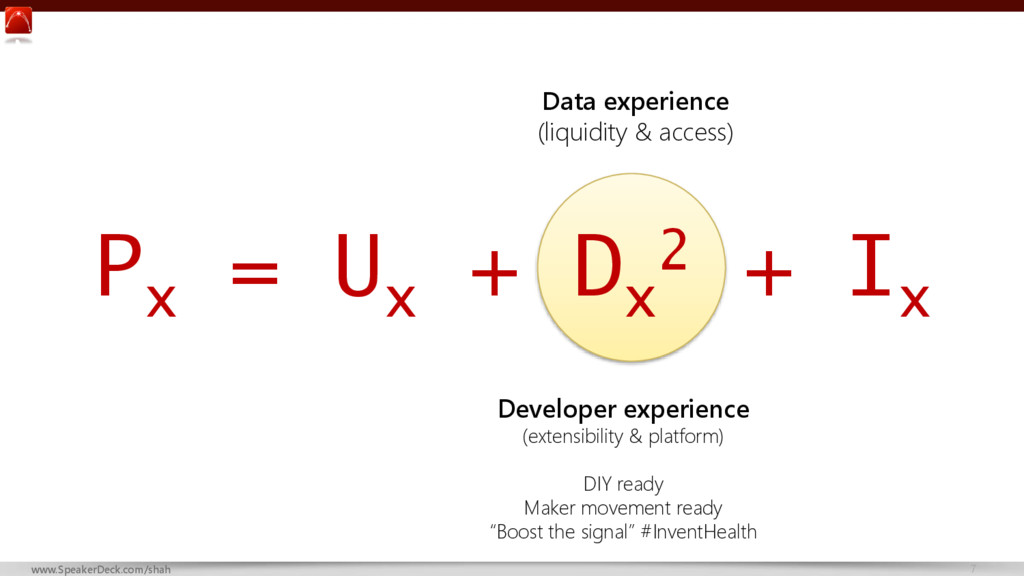
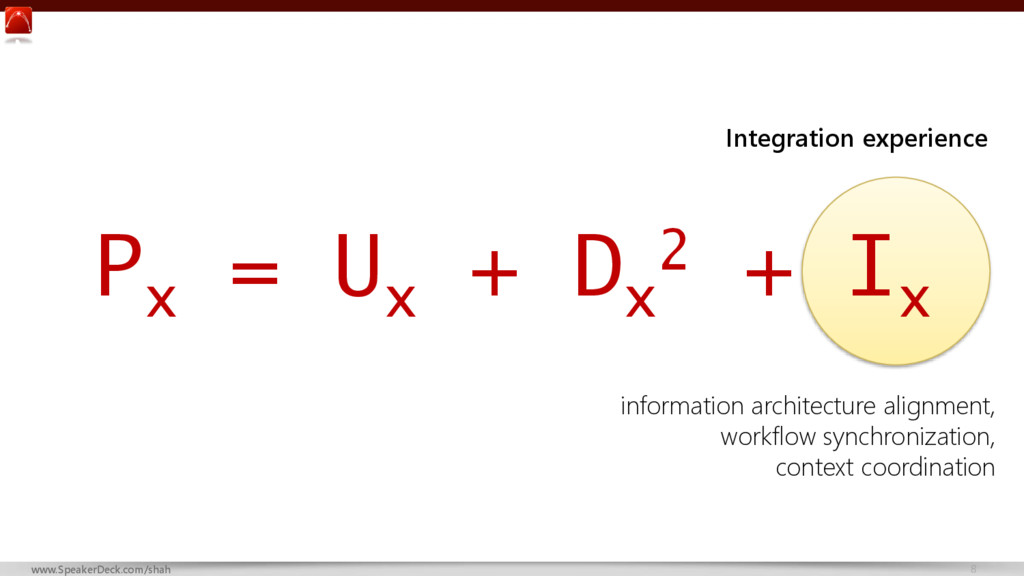
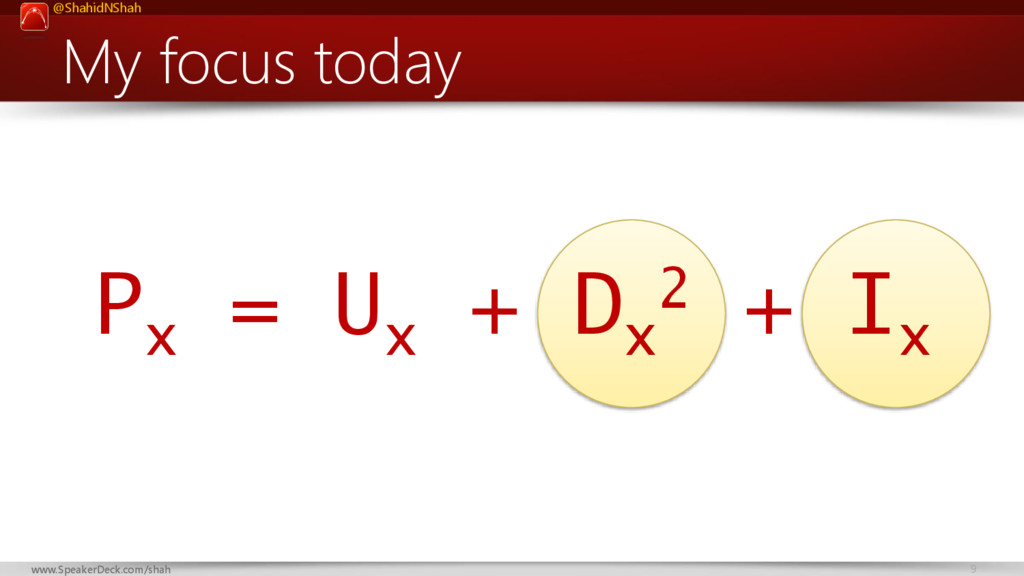
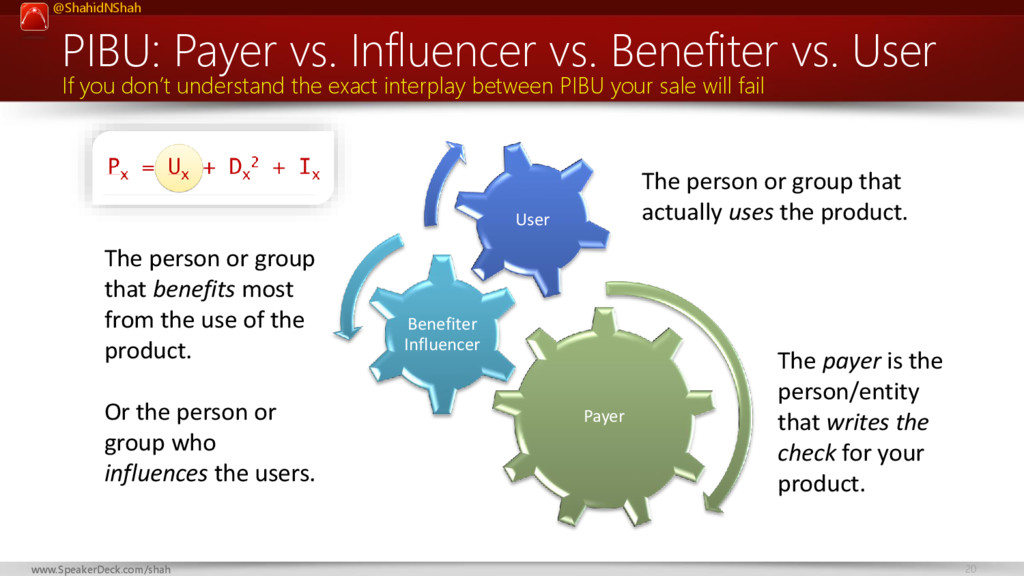
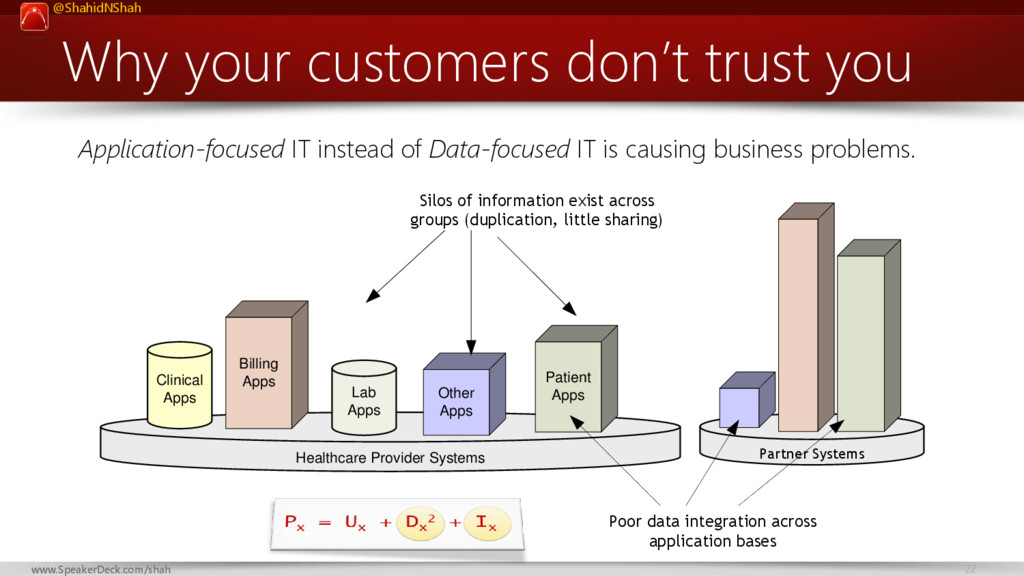
Px = Ux + Dx2 + Ix
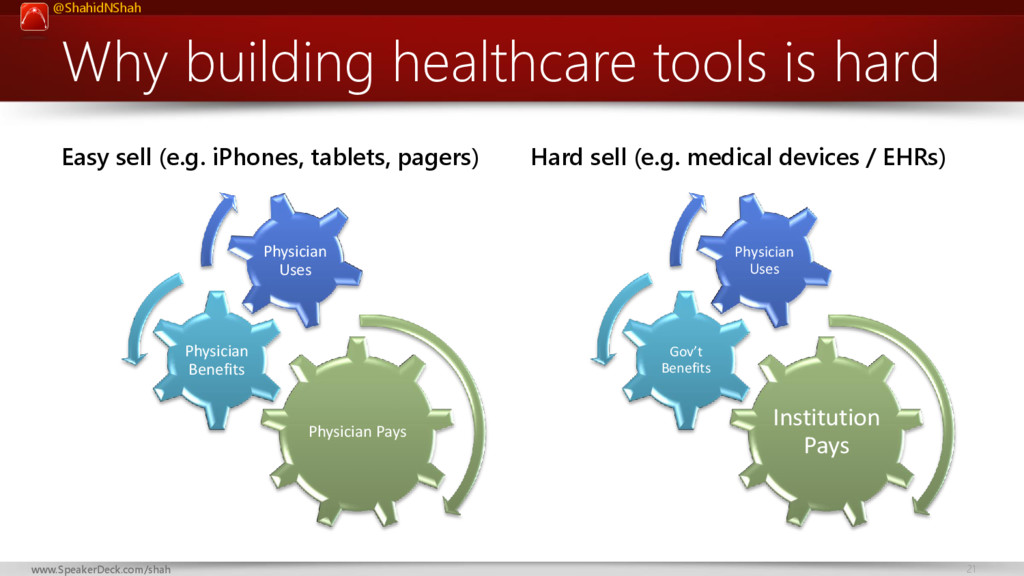
It's the "digital health product success formula" that describes the main ingredients of a healthcare IT development approach that is most likely to succeed in a competitive market.
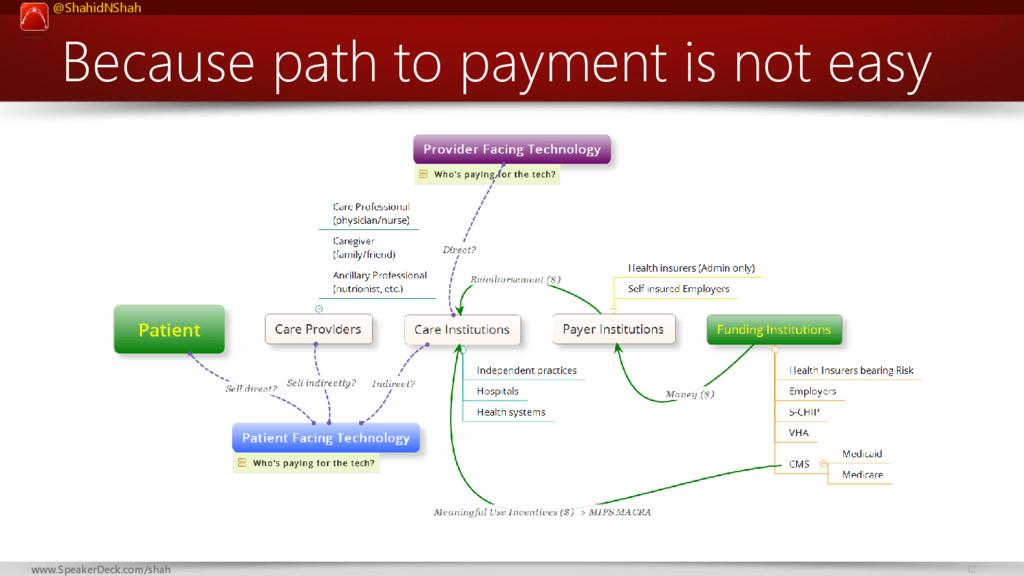
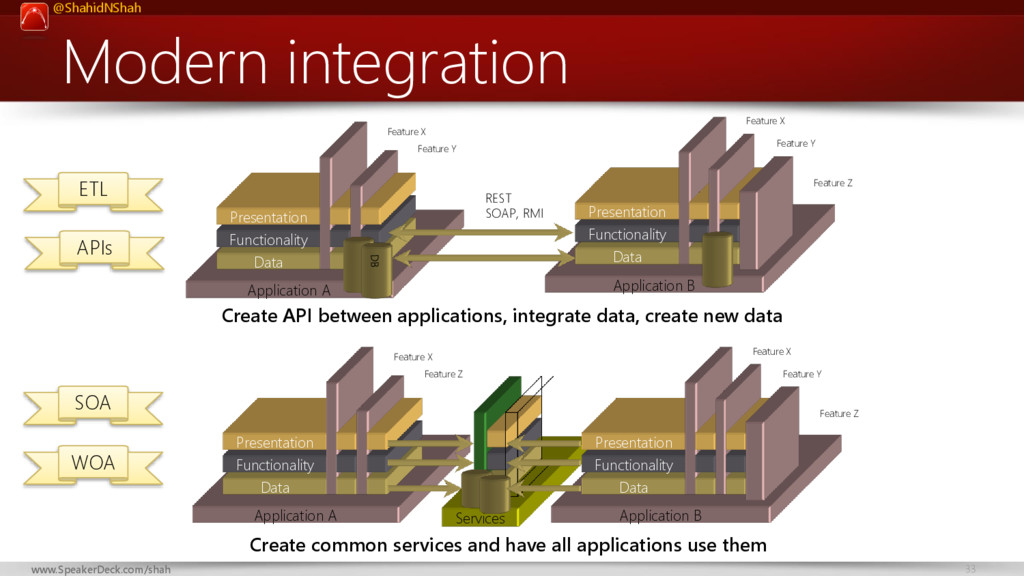
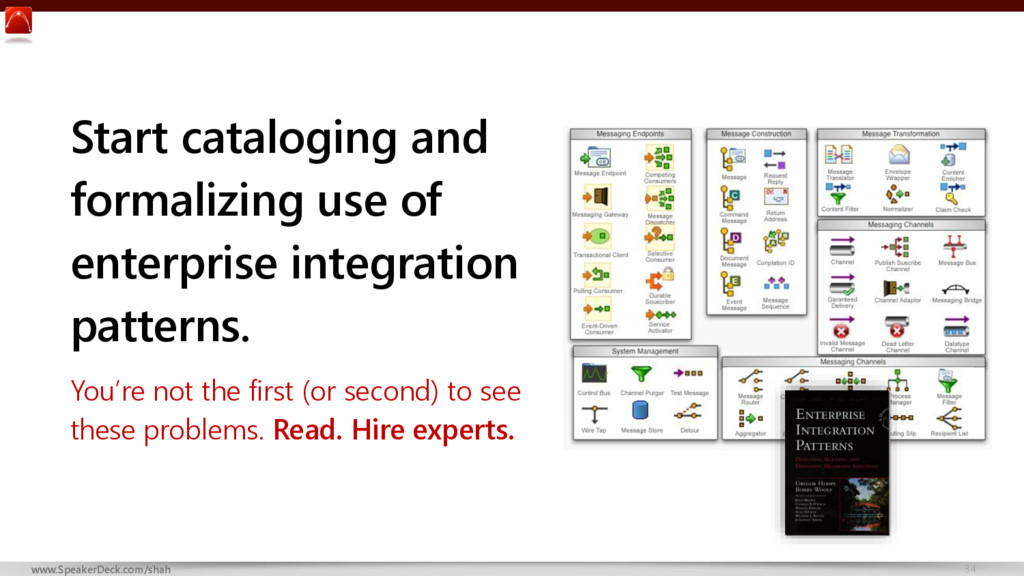
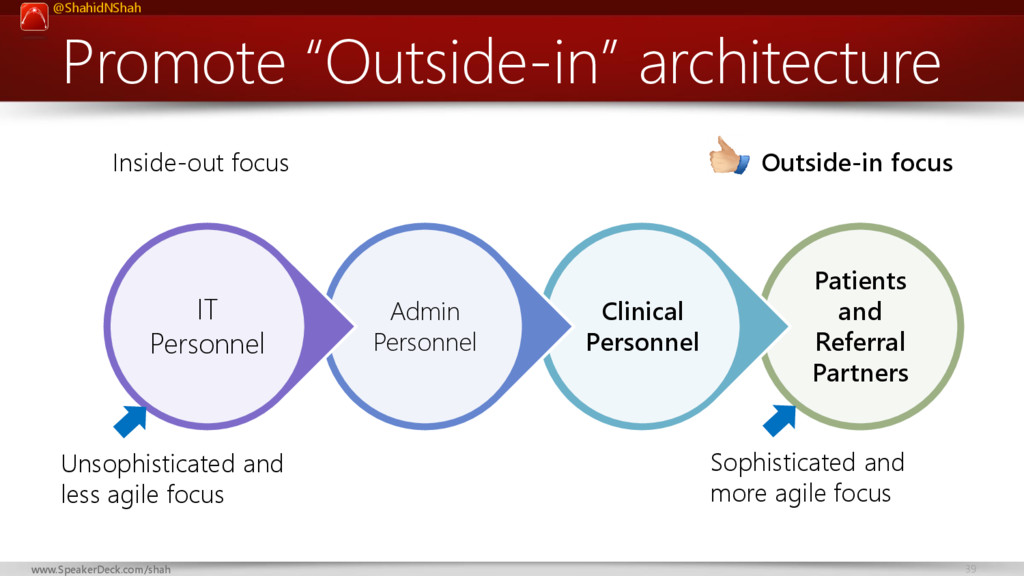
Many enterprise apps are being built these days, most are designed to work as a stand alone system similar to consumer apps. Any enterprise app which acts like a consumer app that doesn’t integrate well into hospital or ambulatory systems and workflows is doomed long term.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Thank You Visit http://www.netspective.com http://www.healthcareguy.com E-mail [email protected] Follow @ShahidNShah Call](https://files.speakerdeck.com/presentations/e5ea9c656b4c43ba8dbd1e70c7388bcf/slide_54.jpg){kind=link}