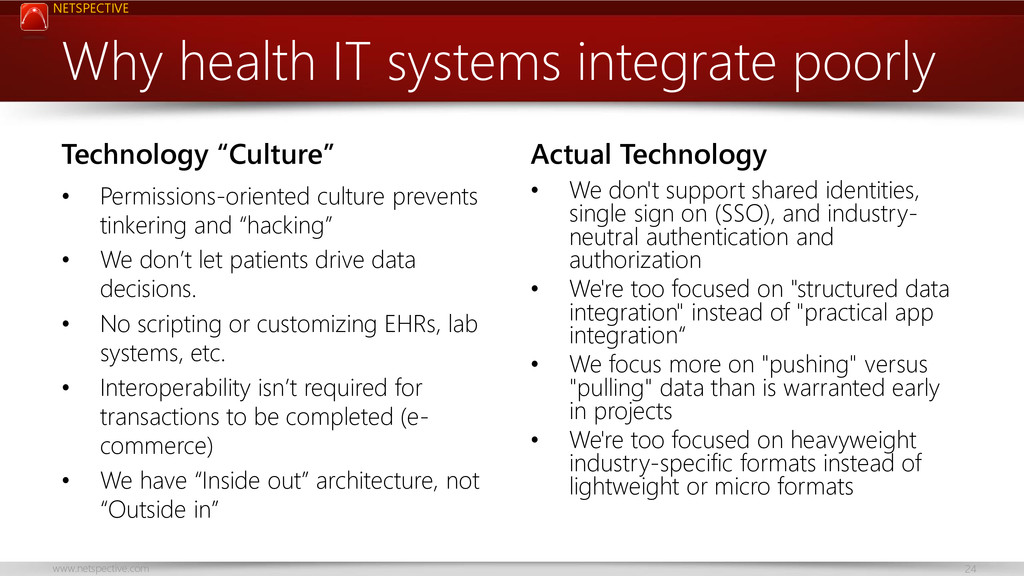
OSEHRA Summit 2012 Lunch Keynote - The Myth of Health Data Integration Complexity. This is an opinionated look at why current health IT systems integrate poorly and how it’s a big opportunity for the OSEHRA Community.
Background:
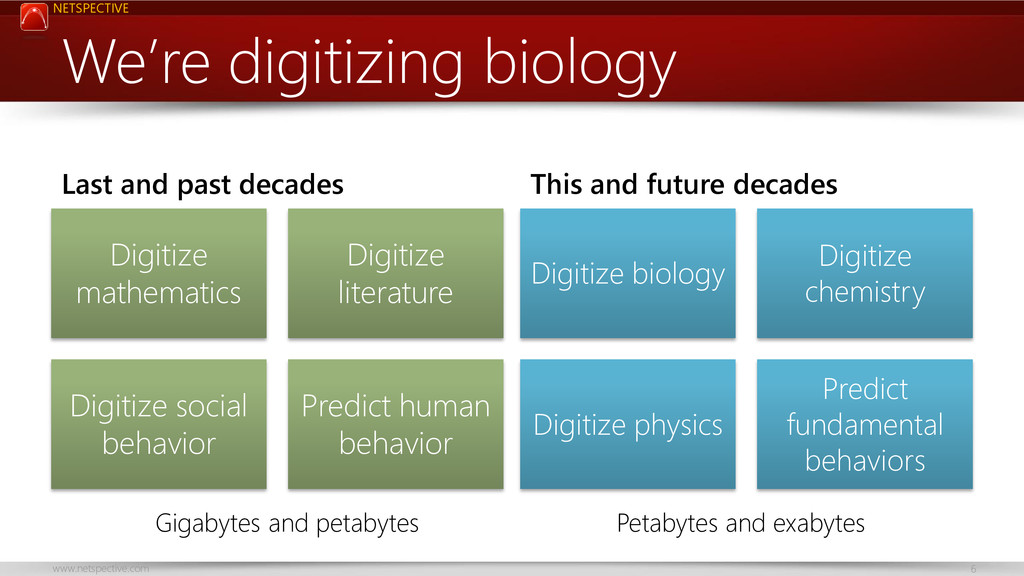
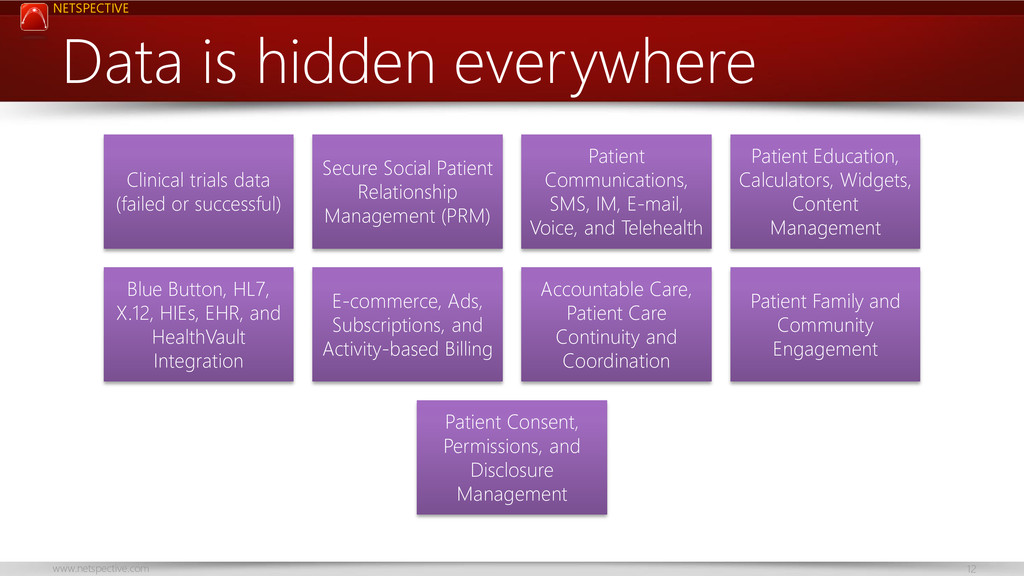
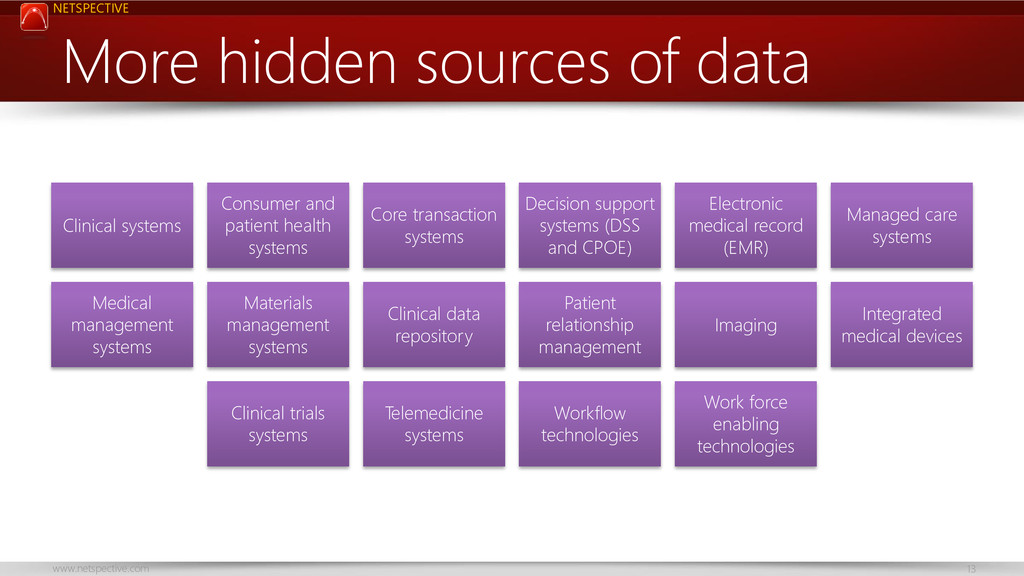
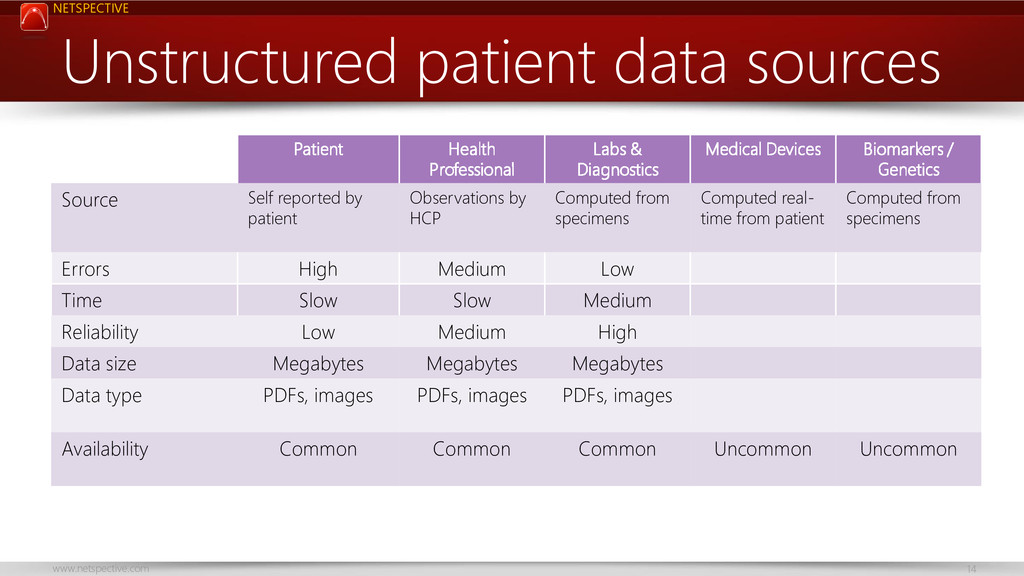
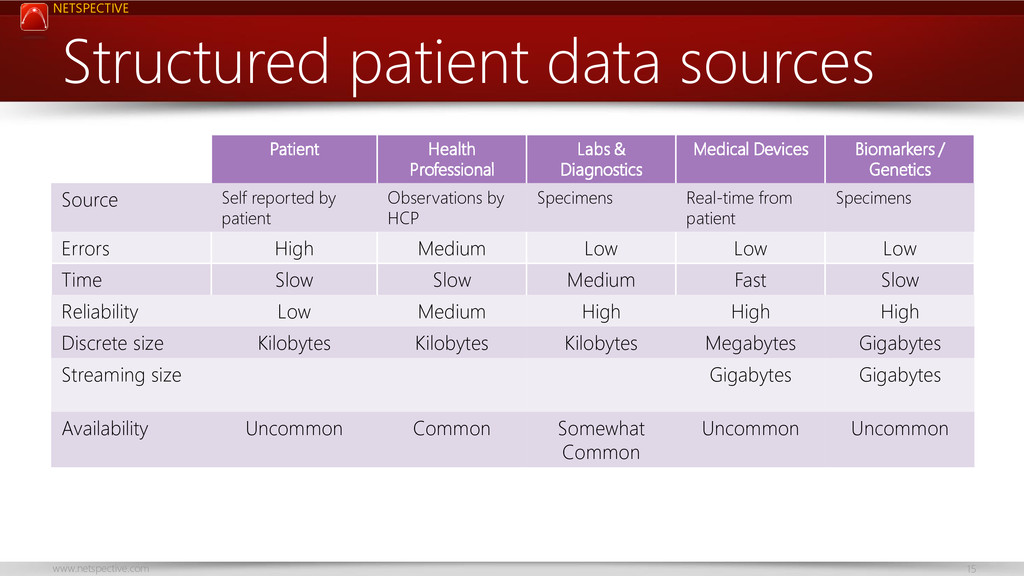
* A deluge of healthcare data is being created as we digitize biology, chemistry, and physics.
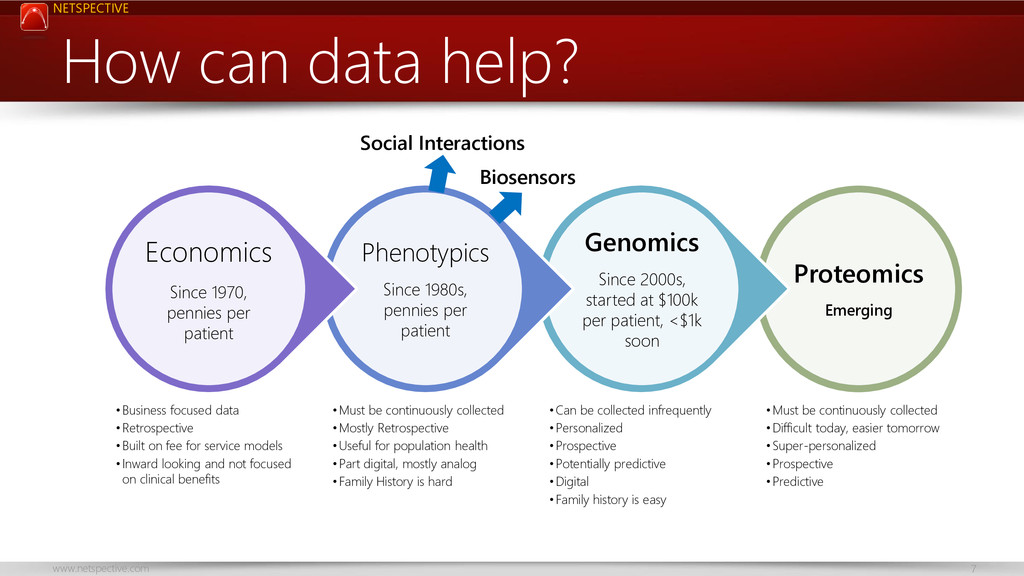
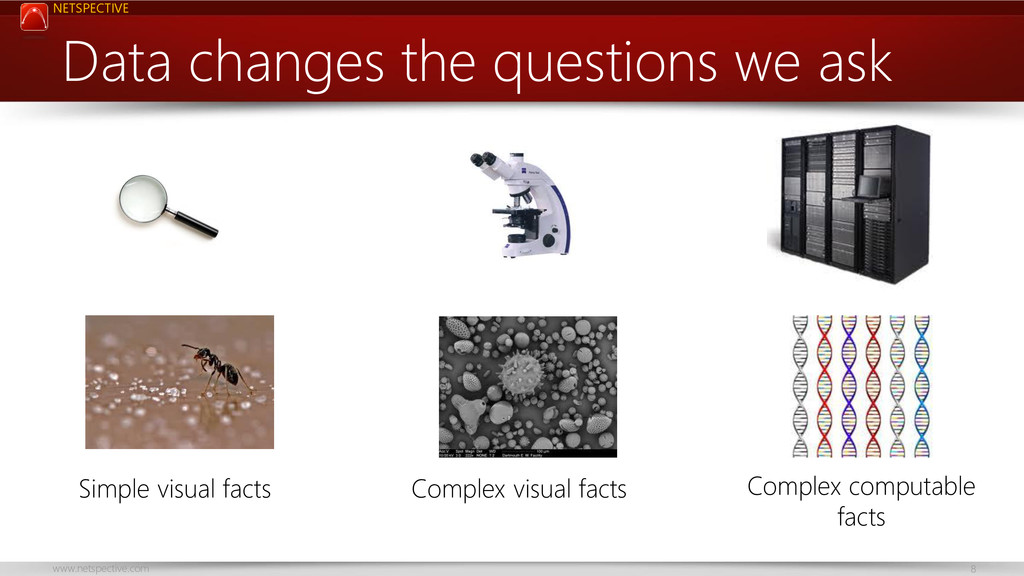
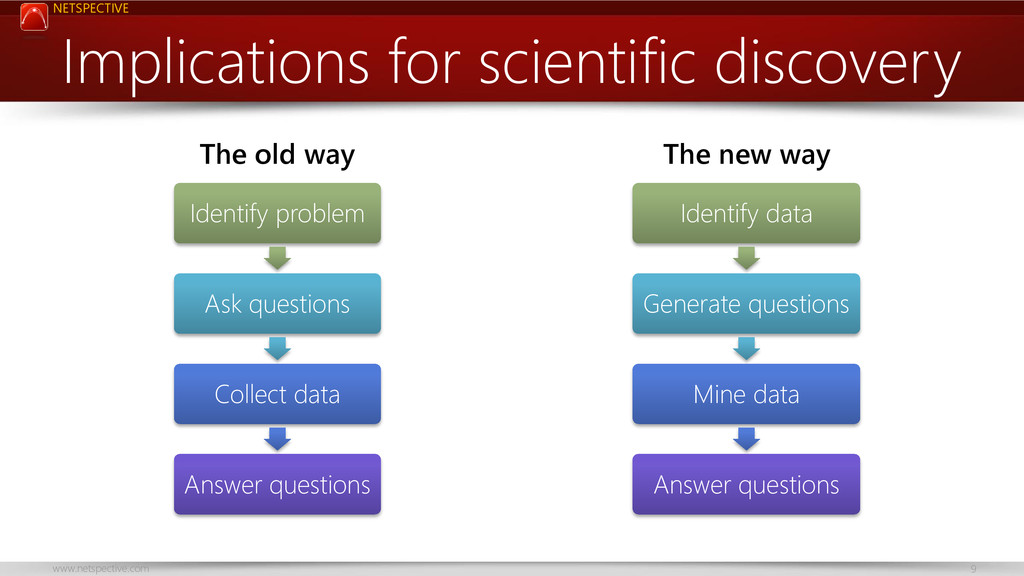
* Data changes the questions we ask and it can actually democratize and improve the science of medicine, if we let it.
* While cures are the only real miracles of medicine, big data can help solve intractable problems and lead to more cures.
* Healthcare-focused software engineering is going to do more harm than good (industry-neutral is better).
Key takeaways:
* Major opportunity for systems integrators
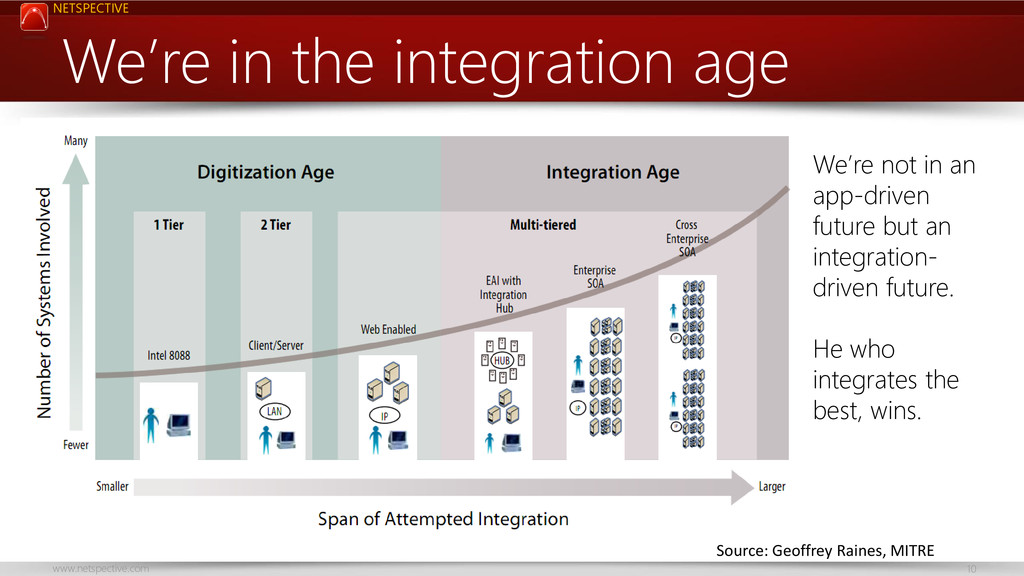
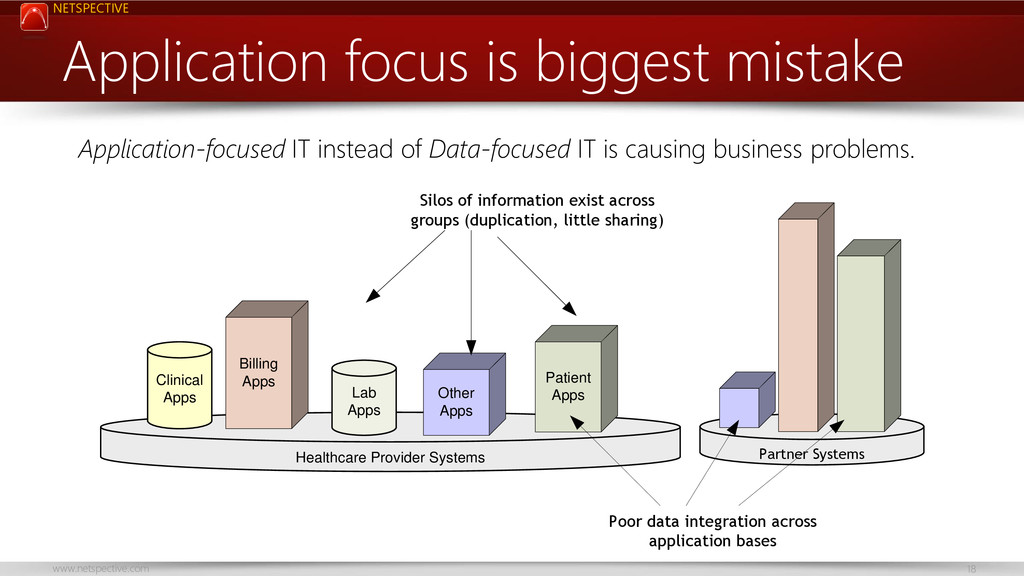
* Applications come and go, data lives forever. He who owns, integrates, and uses data wins in the end.
* Never leave your data in the hands of an application/system vendor.
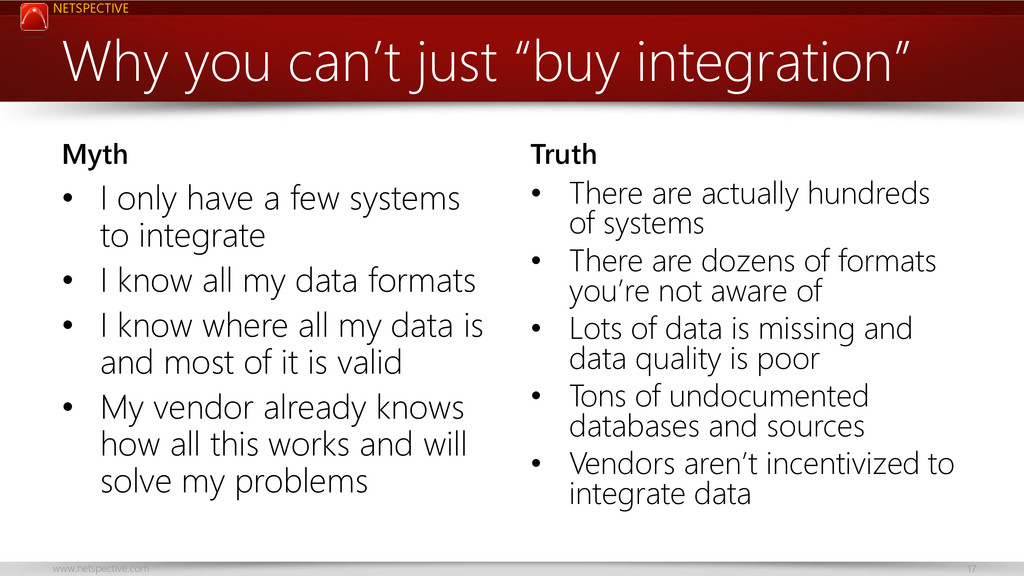
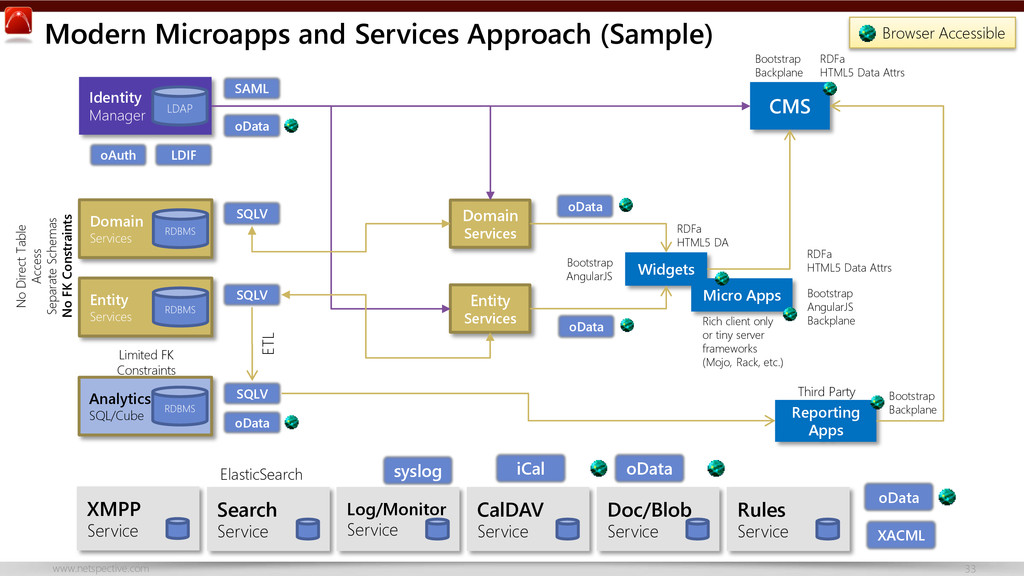
* There’s nothing special about health IT data that justifies complex, expensive, or special technology.
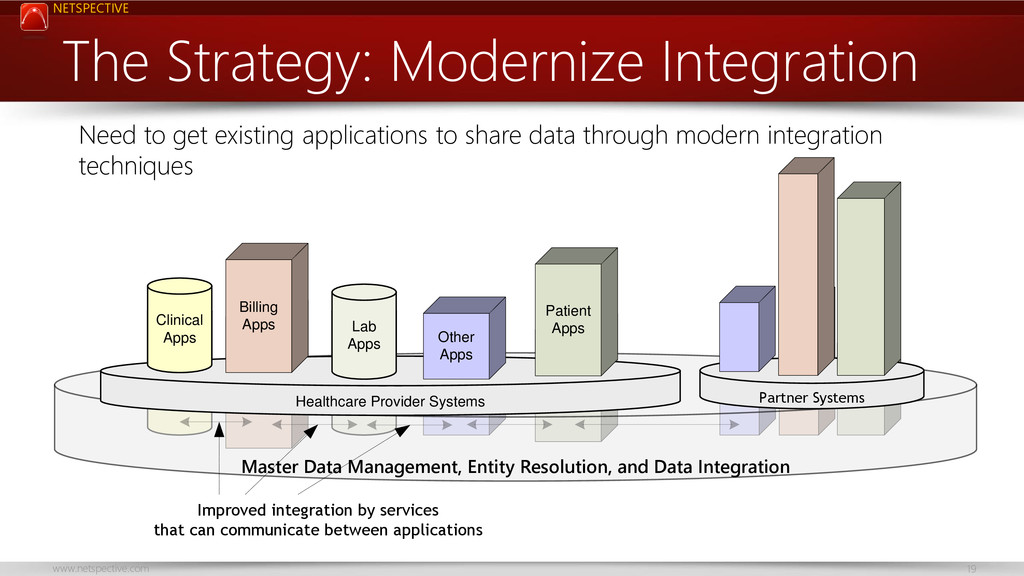
* Spend freely on multiple systems and integration-friendly solutions.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Thank You Visit http://www.netspective.com http://www.healthcareguy.com E-mail [email protected] Follow @ShahidNShah Call](https://files.speakerdeck.com/presentations/d2eb505017b3013037b422000a9e2d10/slide_34.jpg){kind=link}