OF CANCER PAIN • DISCUSS PHARMACOLOGIC TREATMENT OPTIONS, INCLUDING ANTI-INFLAMMATORIES, ANTICONVULSANTS, ANTIDEPRESSANTS • DISCUSS NEURO-AUGMENTATION • DISCUSS INTRATHECAL DELIVERY SYSTEM • DISCUSS NEUROLYSIS FOR CANCER PAIN, INCLUDING ALCOHOL AND PHENOL • DISCUSS NEUROSURGICAL OPTIONS FOR CANCER PAIN
IS 65 • 60-90% OF PTS WILL HAVE PAIN • PAIN FROM DISEASE OR TREATMENT? IN PEDS, TENDS TO BE FROM TX • PAIN AS FIRST SX OF CANCER TENDS TO INDICATE ADVANCED DISEASE AND IS AN INDEPENDENT PREDICTOR OF POOR PROGNOSIS
TX • IN GERIATRIC POPULATION, COMORBIDITIES AND DRUG-DRUG INTERACTIONS NEED TO BE TAKEN INTO EFFECT • PRESENT PAIN IS MOST RELIABLE IN SETTING OF COGNITIVE IMPAIRMENT • IN PATIENTS WITH SUBSTANCE ABUSE HX, THERE IS GREATER RELIANCE ON DIAGNOSTIC IMAGING • INMATES HAVE HIGHER RATES OF CANCER, INCREASED MORTALITY, AND UNDERTREATED SYMPTOMS
GROWTH FACTOR, CYTOKINES, ATP, PROTONS FROM DYING CELLS • THESE SUBSTANCES ACTIVATE PRIMARY AFFERENT AND AWAKEN SILENT NOCICEPTORS (FEED FORWARD LOOP) • PRIMARY AFFERENT DISCHARGE LEADS TO DORSAL HORN HYPEREXCITATION AND THE ACTIVATION OF MICROGLIA. • PERIPHERAL INHIBITION VIA ACTIVATION OF PERIPHERAL AND CENTRAL OPIOID RECEPTORS, COX PATHWAYS AND DESCENDING MODULATION.
(VIA COMPRESSION OR ISCHEMIA/ HEMORRHAGE, CHEMICAL OR TRANSECTION). • PERIPHERAL DAMAGE ACCUMULATION OF ABNORMAL SODIUM AND CALCIUM CHANNELS AT THE SITE OF INJURY • ALTERATIONS TO GENE EXPRESSION OF RECEPTORS • DAMAGED NEURONS DISCHARGE SPONTANEOUSLY AND THERE IS CROSS-TALK TO NORMAL FIBERS AND RECRUITMENT OF SILENT NOCICEPTORS • EXCESSIVE OR ABSENT DISCHARGE FROM PRIMARY AFFERENTS WITHIN THE DORSAL HORN RESULTS IN OVERALL EXCITATION AN ALTERATION IN EXPRESSION OF NMDA RECEPTORS AND FUNCTIONAL LOSS OF OPIOID AND GABAMINERGIC SYSTEMS • THERE IS RESULTANT HYPEREXCITATION WITH INCREASED RECEPTIVE FIELDS PRIMARY AND SECONDARY HYPERALGESIA, AND ALLODYNIA • DORSAL COLUMNS RELAY PREDOMINATELY TO THALAMUS, GIVING RISE TO STRONG AUTONOMIC RESPONSES AND EFFERENT RESPONSES
IBUPROFEN - NON SPECIFIC - SULINDAC -CYCLOOXYGENASE II SPECIFIC CELECOXIB AND MELOXICAM • ANTICONVULSANT AGENTS • ANTIDEPRESSANTS • MIXED MU AGONISTS • MU AGONISTS • ALPHA 2 AGONISTS
ANIMAL MODELS OF INFLAMMATION AND NERVE PAIN (LITTLE TO NO EFFECT ON ACUTE PAIN) • B L OCK THE AL PHA 2 DE LTA S UB UNIT OF THE L TYPE CAL CIUM CHANNE L • ACT IN THE OUTER LAYERS OF THE DORSAL HORN • DECREASE THE RELEASE OF GLUTAMATE NOREPINEPHRINE SUBSTANCE P
EFFICACY AT 2 WEEKS VS 2 MONTHS • FEWER SIDE EFFECTS, BUT STILL CAUTION IN RENAL DX. • DOSED : 25 - 75 QHS IN ELDERLY TO MAX OF 150 PO/DAY • IN DIABETIC NEUROPATHY: NNT =6.3
FIBERS WITH NO EFFECT ON NORMAL FUNCTIONING A- DELTA AND C-FIBERS • DOSE INITIAL 100MG PO BID TO TID • SIDE EFFECTS: PANCYTOPE NIA - AGRANULOCYTOSIS AND APLASTIC ANEMIA; CBC NECESSARY EVERY THREE WEEKS (BLOOD TESTS 2-4 MONTHS) STEVEN JOHNSON SYNDROME TOXIC EPIDERMAL NECROSIS DIZZINESS AND GAIT DISTURBANCE • TREATMENT MODELS TG NEURALGIA- NNT<2, NNH 24 POST CVA PAIN
• DOSE: 100MG BID • SIDE EFFECTS: CHANGE IN FACIAL FEATURES (COARSENING) GINGIVAL HYPERPLASIA SEDATION CHANGES IN MOTION STABILITY • TREATMENT MODELS: STILL USED IN RECALCITRANT ONCOLOGY RELATED PAIN • INCREASES ACTIVITY OF CP450, DECREASING EFFICACY OF METHADONE, FENTANYL, TRAMADOL, MEXILETINE, LAMOTRIGINE, CARBAMAZEPINE • WHEN CO-ADMINISTERED WITH ANTIDEPRESSANTS, AND VALPROIC ACID, THE DECREASED ACTIVITY OF P450 WILL PRODUCE INCREASED CONCENTRATION OF PHENYTOIN
INHIBITS AMPA-TYPE EXCITATORY GLUTAMATE RECEPTOR • DOSE START 25MG QHS • SIDE EFFECTS: SEDATION KIDNE Y S TONE S (TOPIRAMATE INHIB ITS CARB ONIC ANYHYDRAS E ) GLAUCOMA
LEVELS APPROXIMATING 50-100 MCG/ML BUT THESE DOSES ARE NEVER USED WHEN TREATING CHRONIC PAIN • MECH: GABA–A RECEPTOR AGONIST • SIDE EFFECTS: CNS DEPRESSION • TARGET TREATMENT GROUPS: CHANGE IN MIGRAINE THERAPY, SUPPRESS CNS COMPRESSION BY TUMOR
• 12ON/12OFF, ROTATE PATCH • GREAT NEAR DRAIN SITES, CHEST TUBES, RECENT LARGE INCISIONS • SIDE EFFECTS INCLUDE DIZZINESS AND BLURRED VISION AND AT CONCENTRATIONS OF 10MCG/ML, SEIZURE AND 25 MCG/ML CARDIAC DEPRESSION, BUT THE S E PL AS MA L E VE L S HAVE NE VE R RE S ULTE D FROM THE PATCHE S
ASSOCIATED WITH CHRONIC PAIN OR RESULTING FROM THE CHRONIC PAINFUL CONDITION • THERE ARE THREE BASIC CATEGORIES: • TCA - EXAMPLE ELAVIL • SSRI - EXAMPLE PROZAC (RARELY USED IN ONCOLOGY PATIENTS WHY DUE TO SEROTONIN SYNDROME) • SNRI – EXAMPLE CYMBALTA
INCREASING SYNAPTIC LEVELS OF THESE MEDS • THEY HAVE INDEPENDENT ANALGESIC PROPERTIES AT LOWER DOSES • DIFFER IN TERMS OF SIDE EFFECTS: • ANTICHOLINERGIC, (DRY MOUTH, CONSTIPATION, BLURRED VISION, URINARY RETENTION) • ANTIHISTAMINE EFFECTS (SEDATION)
TCA PROLONG THE QT INTERVAL, GET AN EKG • TCA DECREASE SEIZURE THRESHOLD • SOME TCA HAVE DOCUMENTED ANALGESIC PROPERTIES • ALL TCA CAUSE URINARY RETENTION, DRY MOUTH, POSTURAL HYPOTENSION, WEIGHT GAIN • HEPATIC CLEARANCE INVOLVES THE P450 SYSTEM MEDS WHICH COMPETE FOR THE ENZYME WILL INCREASE LEVELS WHEN CO-ADMINISTERED (SSRI, CIMETIDINE, METHYLPHENIDATE) • P450 ENZYME INDUCERS WILL DECREASE SERUM TCA LEVELS (PHENOBARBITAL, CARBAMAZEPINE, CIGARETTE SMOKING)
SEIZURE THRESHOLD • ASSOCIATED WITH EASY BRUISING AND OSTEOPOROSIS • SIDE EFFECTS INCLUDE DECREASED LIBIDO, IMPOTENCE, DYSTONIA, AKATHISIA, RARE SIADH • FEW INDEPENDENT PAIN PROPERTIES • NEVER PROVEN TO BE OPIOID SPARING WHEN COMPARED TO TCA • TAPER OFF SLOWLY
COMPLAIN OF CRAMPING AND SPASMS, SILENT NOCICEPTORS BECOME ACTIVATED BY INFLAMMATION • ALSO STIMULATED BY: ISCHEMIA, DISTENTION/CONTRACTION, AND COMPRESSION • KEY TRANSMITTERS: SEROTONIN (PERIPHERAL AND CENTRAL) CALCITONIN-GENE-RELATED PEPTIDE, VASOACTIVE INTESTINAL, PEPTIDE, KININS. • DORSAL HORN MODULATION IS TRANSMITTED CENTRALLY VIA SPINOTHALAMIC TO VISCERO- SENSORY CORTEX
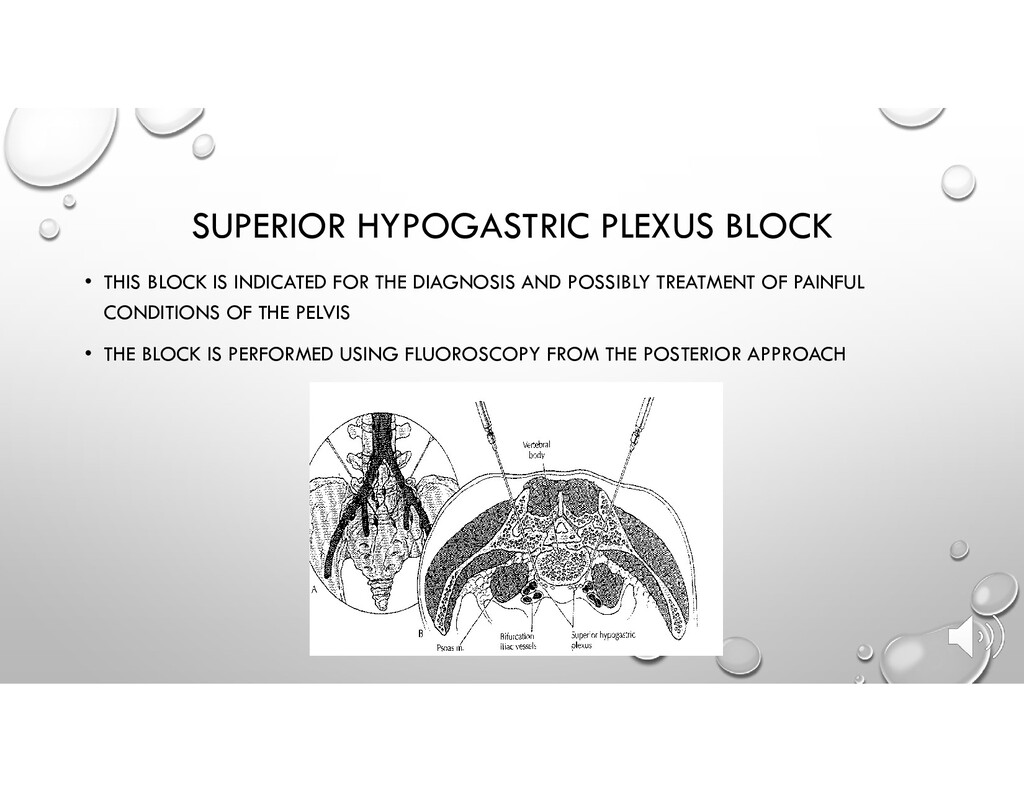
CHRONIC • DIAGNOSTIC • TREATMENT OF ABDOMINAL ISCHEMIA • TREATMENT OF ACUTE PAIN AFTER ARTERIAL EMBOLIZATION FOR CANCER PAIN • TREATMENT OF PAIN SECONDARY TO UPPER ABDOMINAL MALIGNANCY
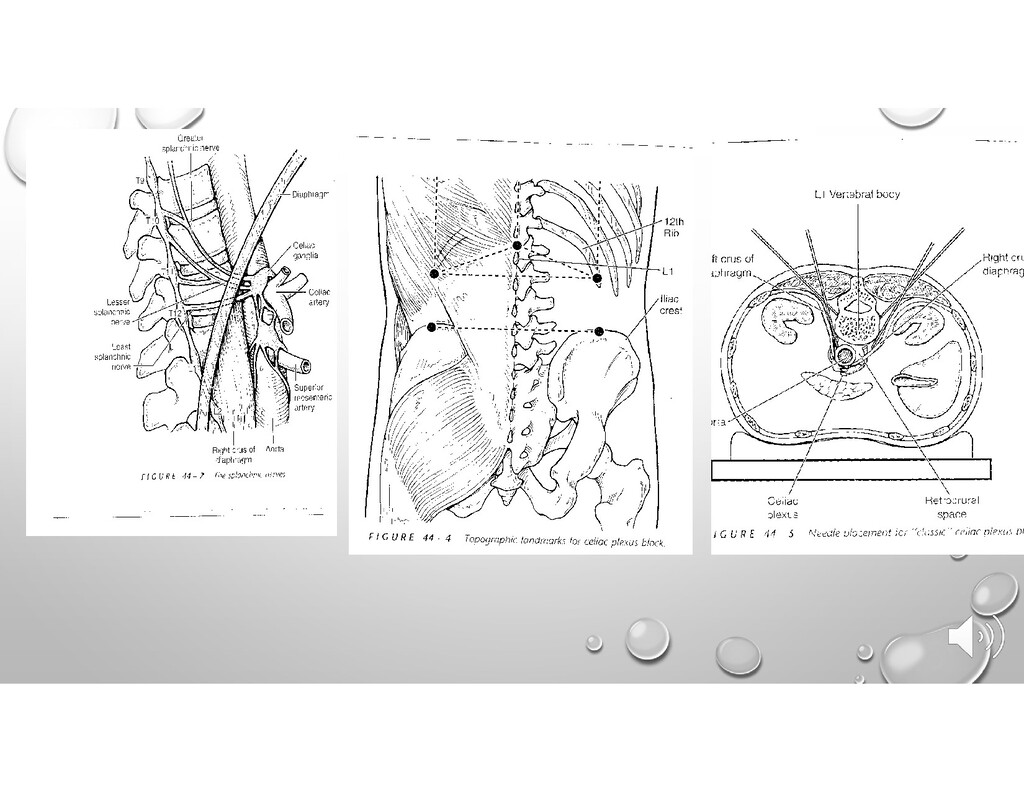
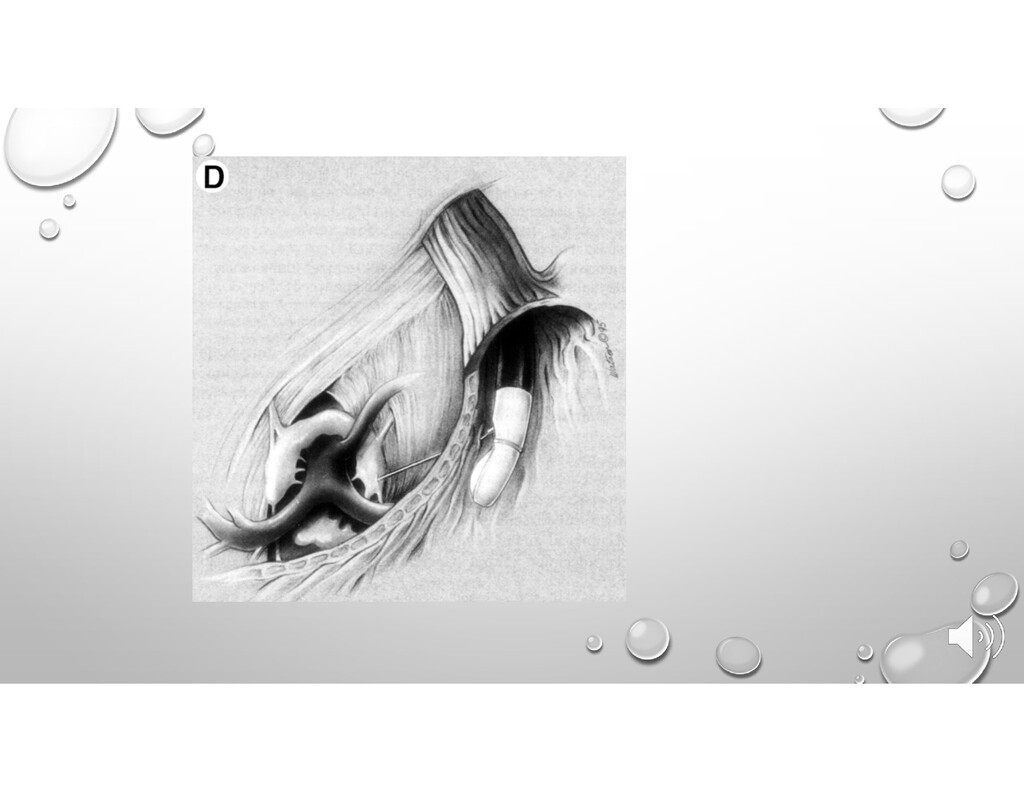
BUT ANTERIOR TO THE CRUS OF THE DIAPHRAGM • THIS IS IMPORTANT : AS AN ANTEROCRURAL BLOCK, THE NEEDLE IS APPRX 1 CM ANTERIOR TO THE LOWER BORDER OF L1; WILL GO THROUGH THE AORTA ON THE LEFT SIDE, DEPOSITING DYE ANTERIOR TO THE AORTA ON THAT SIDE • CONTRIBUTING GANGLIA INCLUDE AORTICO-RENAL AND MESENTERIC • COVERS ENTIRE ASCENDING AND TRANSVERSE COLON, THE DESCENDING COLON AND RECTUM ARE NOT COVERED. • CURRENT LITERATURE REVIEW SUGGESTS THAT THE ADRENAL AND POSSIBLY THE NERVE SUPPLY TO THE OVARY IS COVERED BY THE CPB
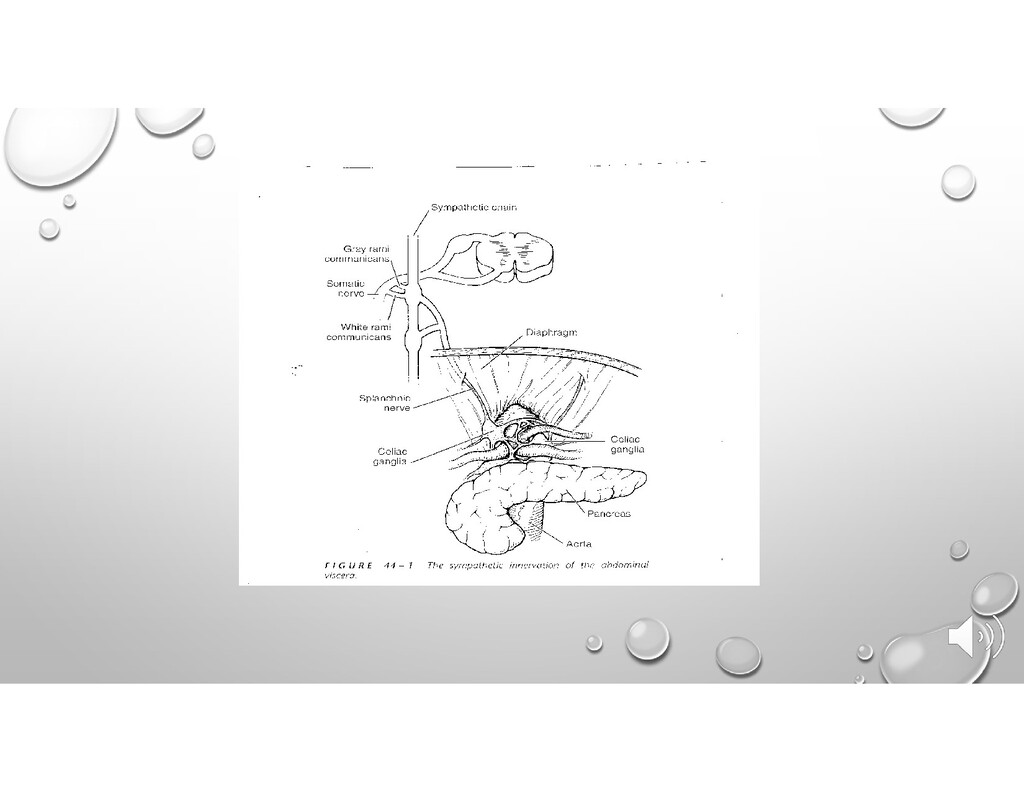
BECOMING THE SPLANCHNIC NERVES • AFFERENT SENSORY FIBERS - C TYPE SILENT NOCICEPTORS WHICH RUN WITH THE ABOVE FIBERS • PARASYMPATHETIC FIBERS FROM THE VAGUS NERVE • SYMPATHETIC AFFERENTS
SEDATION, MONITORING INCLUDING EKG, PULSE OX, ABP • S/PREP BETADINE X3 WITH STERILE DRAPE • LOWER BORDER SPINES OF T12 AND L1 • DISTAL END OF RIB 12, 45° TOWARD MIDLINE • NEEDLE ADVANCED 15° CEPHALAD, SLOWLY UNDER THE LATERAL ASPECT OF THE L1 VERTEBRAL TRANSVERSE PROCESS TO ANTERIOR BODY L1
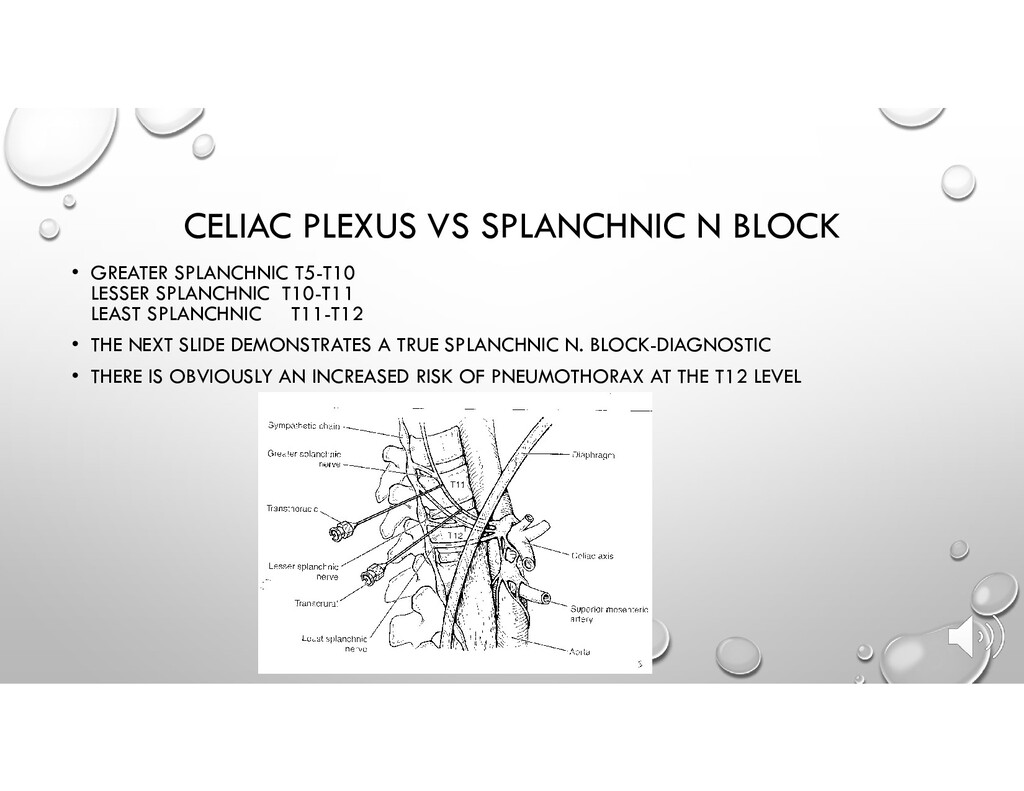
LESSER SPLANCHNIC T10-T11 LEAST SPLANCHNIC T11-T12 • THE NEXT SLIDE DEMONSTRATES A TRUE SPLANCHNIC N. BLOCK-DIAGNOSTIC • THERE IS OBVIOUSLY AN INCREASED RISK OF PNEUMOTHORAX AT THE T12 LEVEL
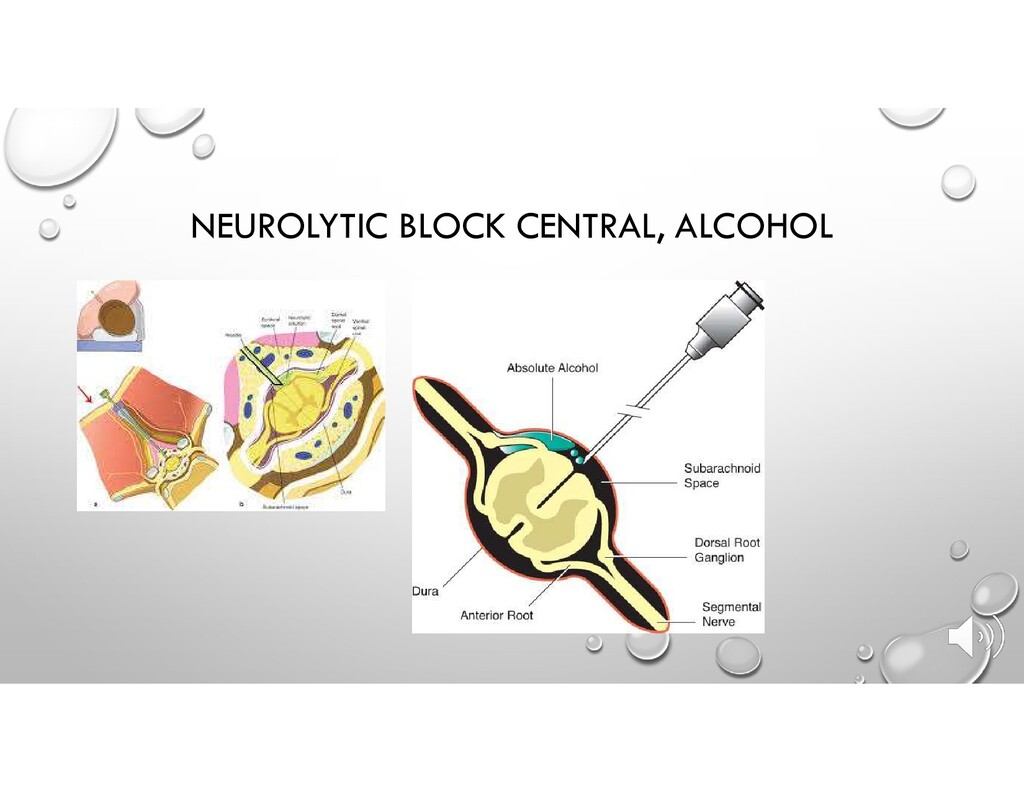
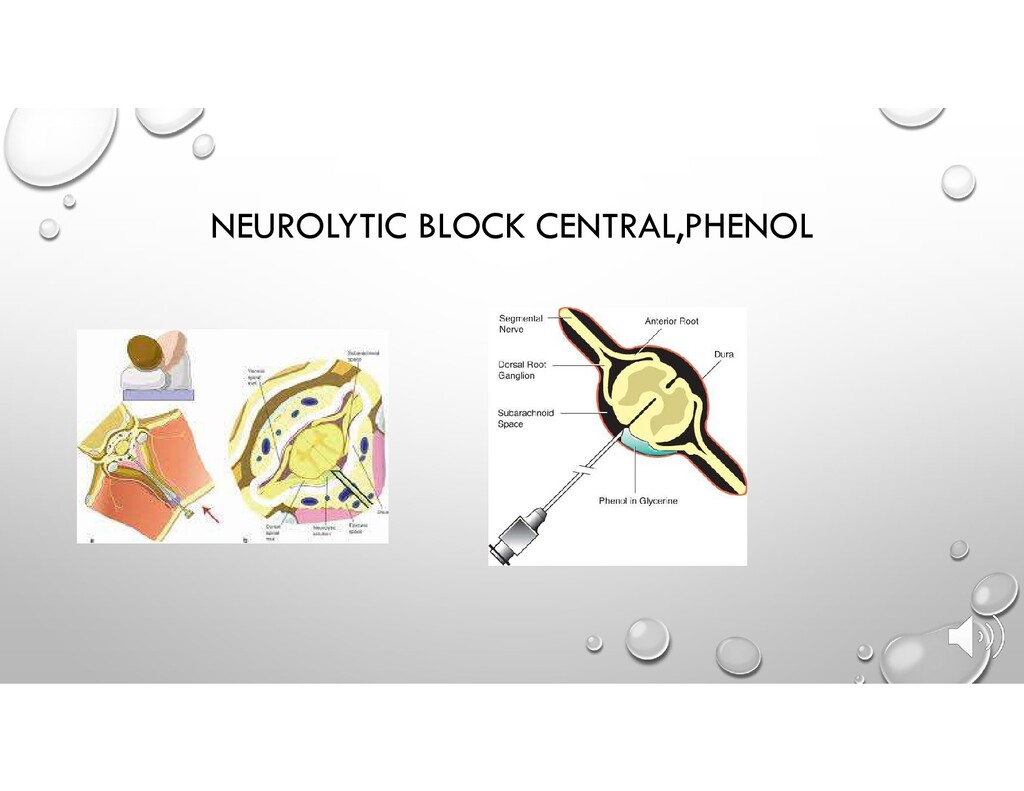
ANESTHETIC + STEROID • NEUROLYTIC- SAME VOLUME OF PHENOL OR ALCOHOL AFTER SUCCESSFUL BLOCK FOLLOWED BY CONTRAST DYE STUDY • PHENOL 6%-12% ANESTHETIC HYPERBARIC DELAYED EFFECTS • ALCOHOL PAINFUL ON INJECTION HYPOBARIC IMMEDIATE EFFECTS • ALCOHOL HAS BEEN ASSOCIATED WITH SPASM OF THE MAJOR SPINAL ARTERIES CAUSING TRANSIENT PARALYSIS
DECOMPRESSION FOR SPINAL TUMORS • NON SURGICAL DECOMPRESSION- CRYOTHERAPY, RFA • CHEMICAL DENERVATION OF TUMOR INVOLVED AREAS • AUGMENTATION OF TUMOR INVOLVED AREAS • SCS • INTRATHECAL NARCOTIC INFUSIONS
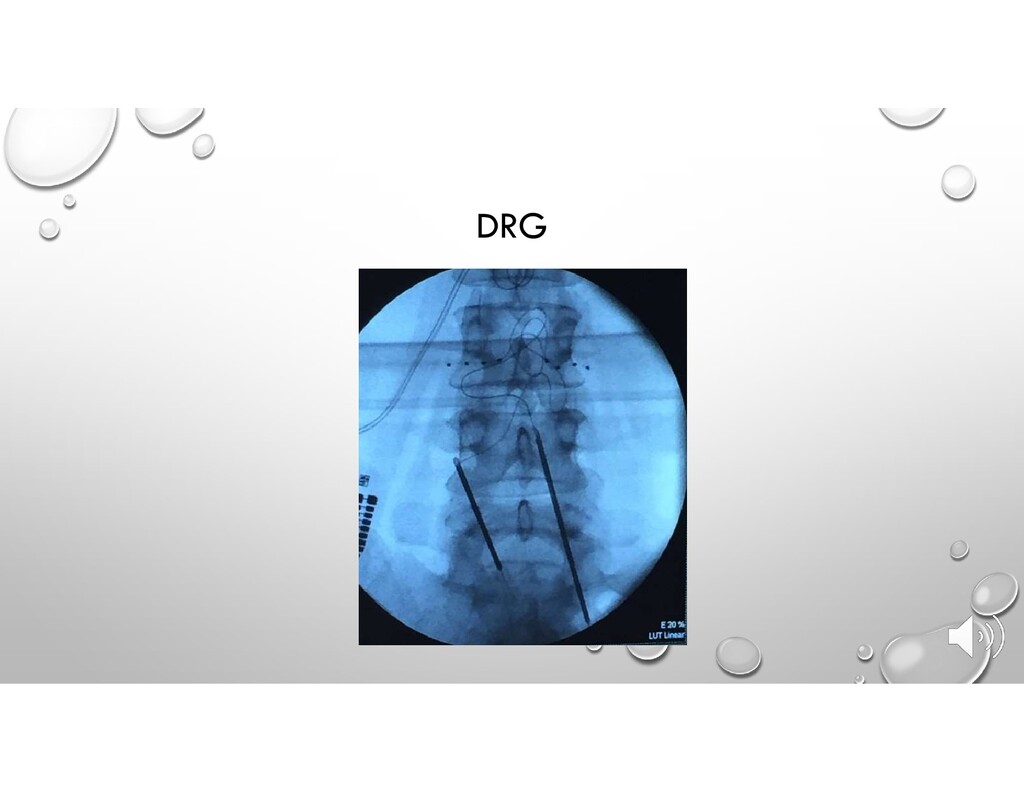
OF MORE DISCRETE AND LOCALIZED STIMULATION PLACEMENT, A ONCOLOGY PAIN GENERATOR CAN BE TREATED BY OVERRIDING THE PAIN SIGNAL WITH A STIM PATTERN • DRG • MRI COMPATIBLE
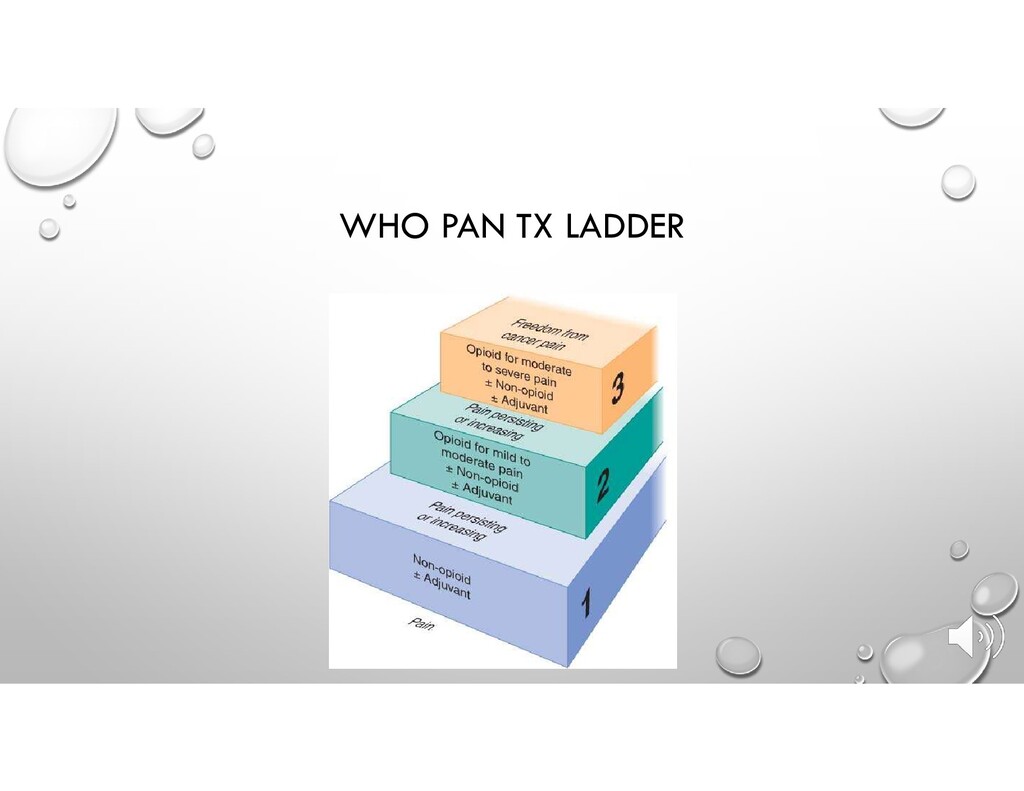
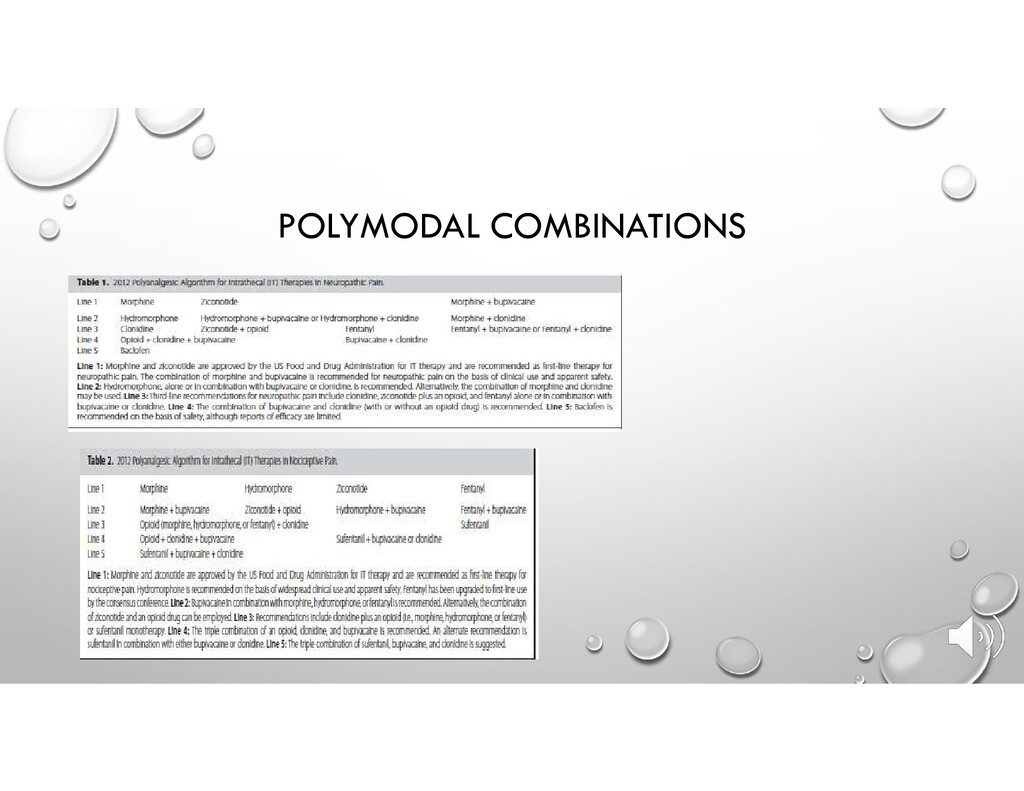
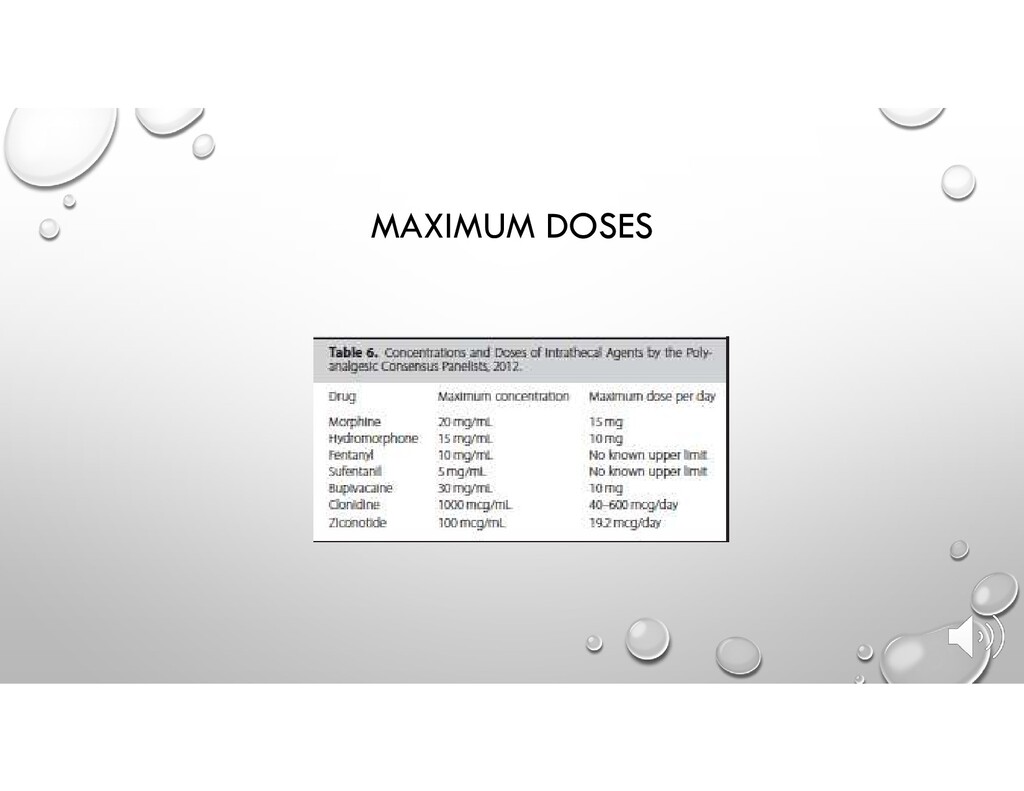
IT IS ESTIMATED THAT UP TO 20% OF PATIENTS HAVE SUBOPTIMAL PAIN CONTROL DESPITE APPROPRIATE WHO ANALGESIC LADDER. • PARADIGM SHIFT: INTERVENTIONAL PAIN MANAGEMENT NO LONGER LAST RESORT • MORPHINE: INTRATHECAL DAILY DOSE COULD BE REDUCED BY A FACTOR 12 TO 300, COMPARED WITH THE ORAL DAILY DOSE
OF INFUSION WITH BOLUS OPTION FOR BREAKTHROUGH PAIN • LOWER DOSES OF DRUG GENERALLY PRODUCE FEWER ADVERSE EFFECTS (SEDATION, COGNITIVE DEFICITS, FATIGUE, AND CONSTIPATION) • INTRATHECAL DRUG ADMINISTRATION CAN PROVIDE MORE EFFECTIVE ANALGESIA THAN SYSTEMICALLY ADMINISTERED • EARLY IMPLEMENTATION MAY LEAD TO IMPROVED SURVIVIAL (SMITH, T.J. ET AL. 2002. JOURNAL OF CLINICAL ONCOLOGY) • MINIMIZE DIVERGENCE OF MEDICATIONS
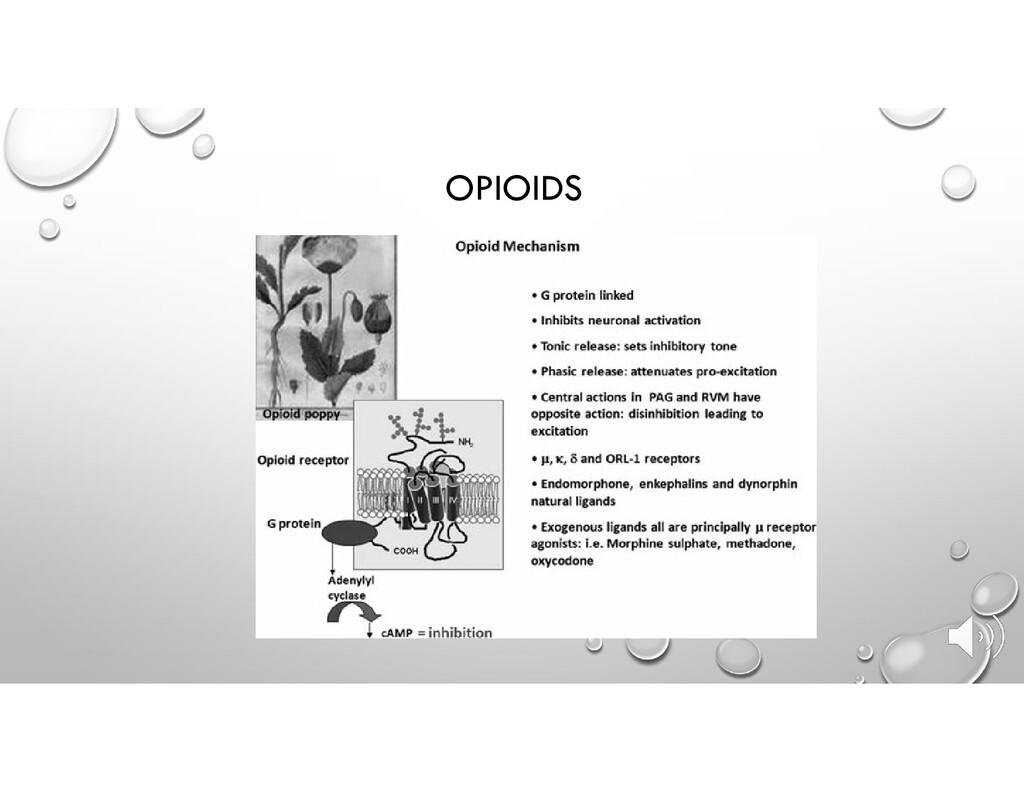
ACTS AT THE SUBSTANTIA GELATINOSA OF THE SPINAL CORD • ANTAGONIZES PRESYNAPTIC N TYPE CALCIUM CHANNELS WITHIN THE DORSAL ROOT GANGLION AND THE REXED LAMINA I AND II • MORPHINE • CENTRAL MU AGONIST
OF CRANIAL NERVE NEURALGIAS TRIGEMINAL GLOSSOPHARYNGEAL • RF LESIONING, GLYCEROL, BALLOON COMPRESSION • STERIOTACTIC RADIOSURGERY FOR TREATMENT OF TRIGEMINAL NEURALGIA IS ALSO POSSIBLE, BUT PAIN RELIEF CAN TAKE TWO WEEKS TO MATURE
• INDICATION: -BRACHIAL PLEXUS INJURY/MALIGNANCY -TRIGEMINAL CEPHALIC NUCLEUS • TARGET IS LISSAUERS TRACT, INFEROLATERAL ASPECT, WHERE THE DORSAL SENSORY SYSTEM ENTERS THE DORSAL HORN OF SPINAL TRACT • DISRUPTS INFLOW AND OUTFLOW FROM THE SUPERFICIAL LAYERS OF SPINAL CORD DORSAL HORN • PRESERVES PROPRIOCEPTION
• WHERE –SURG ACCESS UPPER POSTERIOR SPINE • WHY – TREAT PAIN OF MALIGNANCY, CUTS THE CENTRAL PROCESSES ON NOCICEPTORS AFTER THEY CROSS IN ANTERIOR COMMISSURE, THEN ASCEND, LANCINATING PAIN THERAPY • RESULTS: CONTRALATERAL DEFECT IN PAIN AND TEMPERATURE 2-5 LEVELS BELOW THE LESION • CONCERNS/COMPLICATIONS: THERE IS A HIGHER RISK OF PULMONARY COMPLICATIONS ON THE TREATED SIDE
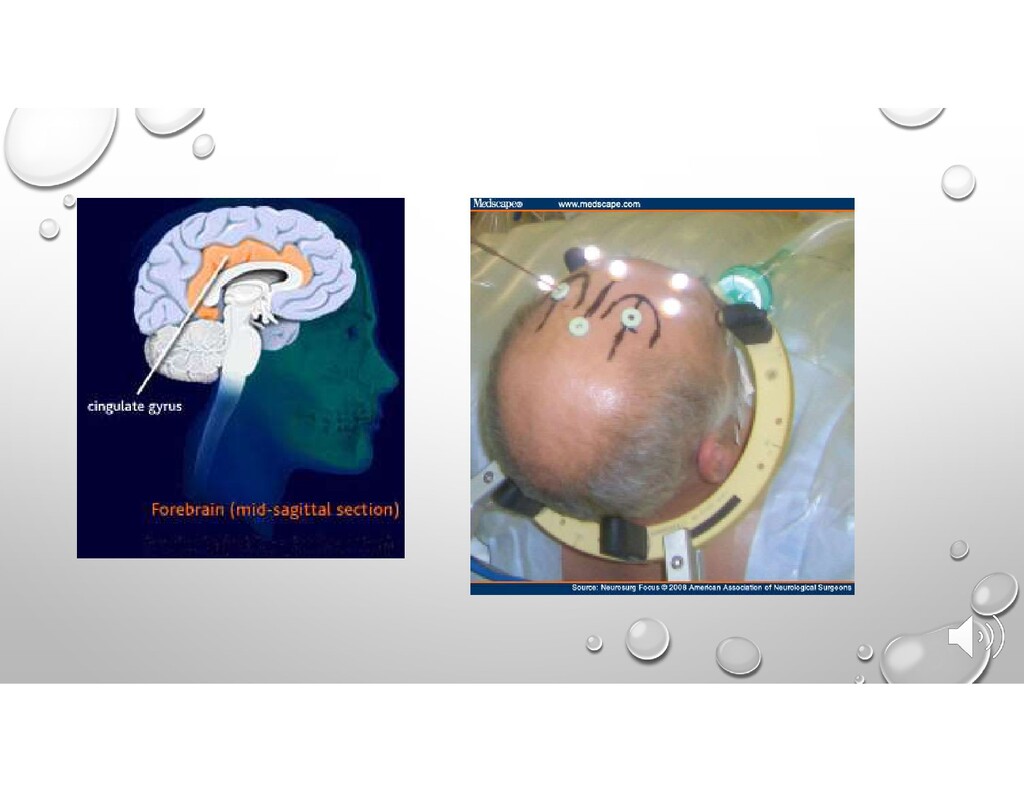
LOBOTOMY PROCEDURE THAT WAS PERFECTED BY FREEMAN AND WATTS • WHERE-RF LESIONS OF BILATERAL ANTERIOR CINGULATE GYRUS • INDICATED FOR INTRACTABLE PAIN OF MALIGNANT ORIGIN • ALL OTHER TREATMENT FAILED “PSYCOSURGERY”
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}