different for most surgeries ◦ Exceptions are AV fistulas and phantom limb pain • Advantages ◦ Attenuation of surgical stress ◦ Increased tissue perfusion ◦ DVT prophylaxis ◦ Less PONV ◦ Decreased PACU time ◦ Decreased narcotic use ◦ Earlier feeding, earlier bowel function ◦ Earlier mobilization
block ◦ Patient refusal ◦ Skin infection at the site of injection (sepsis?) ◦ Coagulopathy ◦ Surgery specific contraindications • Failed block? ◦ Probably not ◦ Does the patient have to pee? ◦ Is the intern leaning on their head? ◦ Low back pain on a flat table? ◦ Many hours of the same position? ◦ Generally disinhibited?
limb, the vein is filled with local anesthetic ◦ Has direct contact with nerve endings near blood vessels and additional spread is via the vasa nervorum • Good for short, distal extremity surgery • CRPS • Chemical sympathectomy • Complications: ◦ Large bolus of local anesthetic ◦ Nerve damage ◦ Thrombophlebitis ◦ Compartment syndrome • Contraindications ◦ Crush injuries ◦ “Hard stick” ◦ Overlying skin infections ◦ Compound fractures ◦ Allergy to local anesthetic ◦ Severe or unknown vascular injuries to extremity ◦ AVF or AVM precluding tourniquet use ◦ Sickle cell disease ◦ Surgery planned for longer than one hour
◦ At level or distal to the site of surgery • Double pneumatic Tourniquet placed as close to site of surgery as possible • Arm is elevated and wrapped in Esmarch • Proximal cuff is inflated to suprasystolic pressures • Inject 30-50 mL of 0.5% lidocaine into IV catheter • IV catheter is removed • Surgeon may proceed • When tourniquet pain begins, the distal cuff can be inflated and the proximal cuff is deflated
scheduled for transposition of the ulnar nerve. A Bier block is successfully performed for surgical anesthesia. Which of the following most accurately corresponds to the maximum duration of the surgical anesthesia? A. Concentration of local anesthetic B. Volume of local anesthetic C. Duration of tourniquet inflation D. Duration of binding of sodium channels by local anesthetic • What happens when the surgery is over?
to cause it to fire in order to locate the nerve itself. • Can be used as primary means of localization or with ultrasound • Two primary uses for nerve stimulation: ◦ Can be used to locate the nerve by starting high and decreasing ▪ Starting at 1.5 mA, current is turned down until twitch disappears ▪ If there is a twitch <0.3 mA (approx), needle should be withdrawn ◦ Can be used to demonstrate safety by starting low and increasing ▪ After positioning using ultrasound, current is turned up to approx 0.3 mA ▪ If no twitch, likely not intraneural
• Two techniques for one block ◦ Deep or superficial to the SCM • Indications: Carotid endarterectomy, Thyroid surgery, Cutaneous surgeries, Proximal ⅓ of the clavicle • Complications: Arterial/intrathecal injection • Deep vs superficial describe the technique used ◦ Landmarks for deep: Mastoid process, Chassaignac Tubercle, posterior border of SCM ◦ Landmarks for superficial: SCM • Volume: 10-15 mL (total) Dee
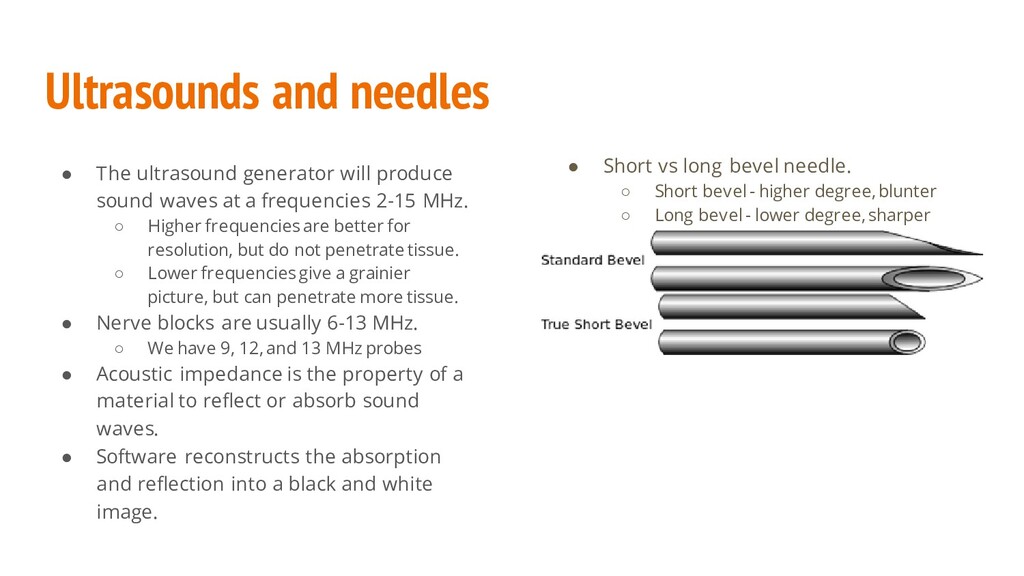
waves at a frequencies 2-15 MHz. ◦ Higher frequencies are better for resolution, but do not penetrate tissue. ◦ Lower frequencies give a grainier picture, but can penetrate more tissue. • Nerve blocks are usually 6-13 MHz. ◦ We have 9, 12, and 13 MHz probes • Acoustic impedance is the property of a material to reflect or absorb sound waves. • Software reconstructs the absorption and reflection into a black and white image. • Short vs long bevel needle. ◦ Short bevel - higher degree, blunter ◦ Long bevel - lower degree, sharper
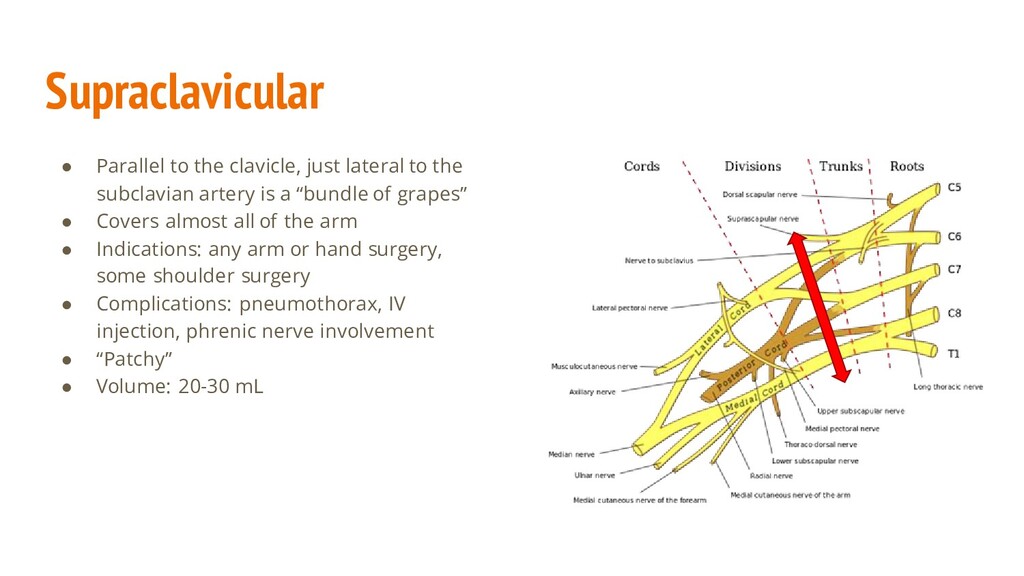
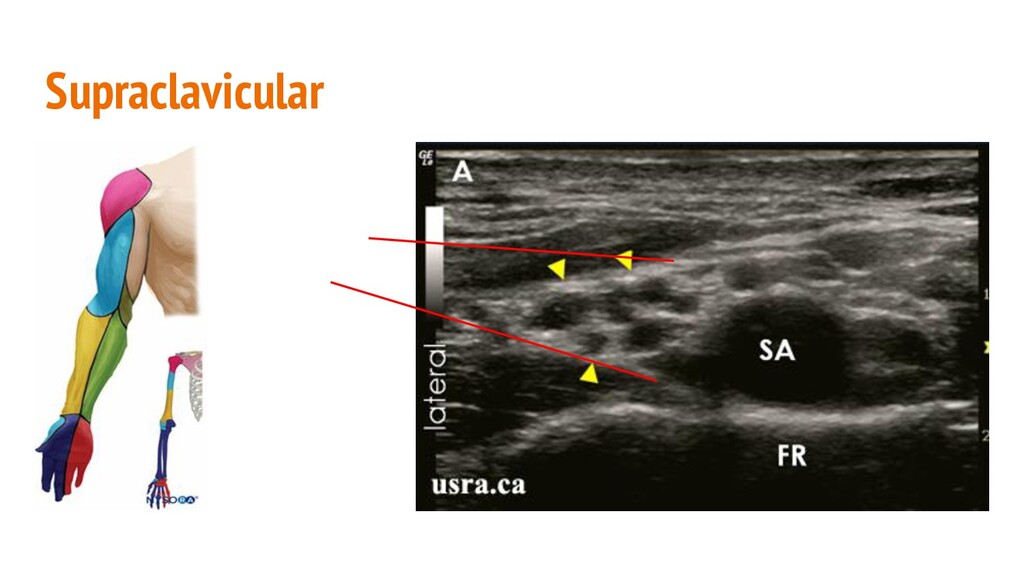
subclavian artery is a “bundle of grapes” • Covers almost all of the arm • Indications: any arm or hand surgery, some shoulder surgery • Complications: pneumothorax, IV injection, phrenic nerve involvement • “Patchy” • Volume: 20-30 mL
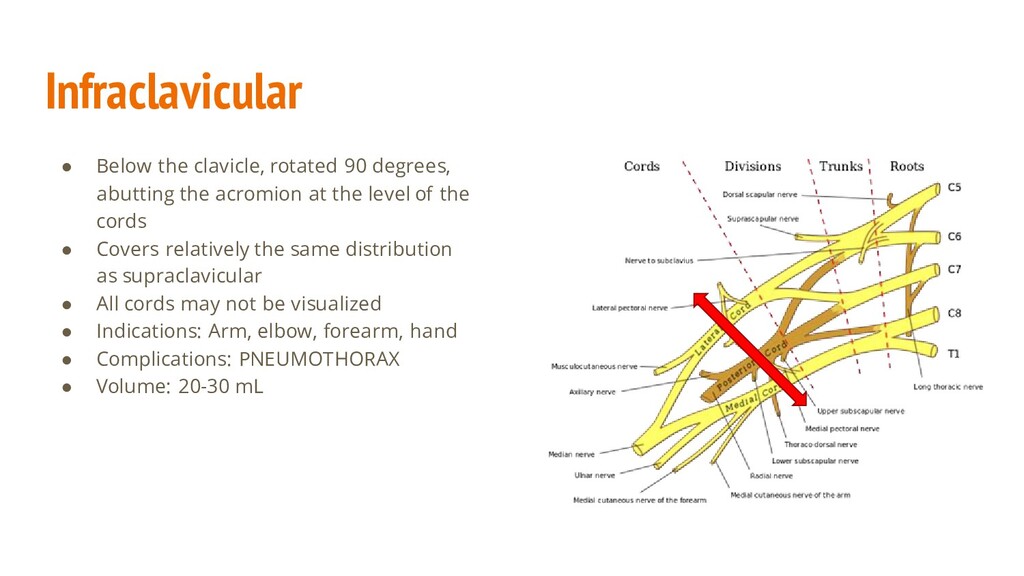
acromion at the level of the cords • Covers relatively the same distribution as supraclavicular • All cords may not be visualized • Indications: Arm, elbow, forearm, hand • Complications: PNEUMOTHORAX • Volume: 20-30 mL
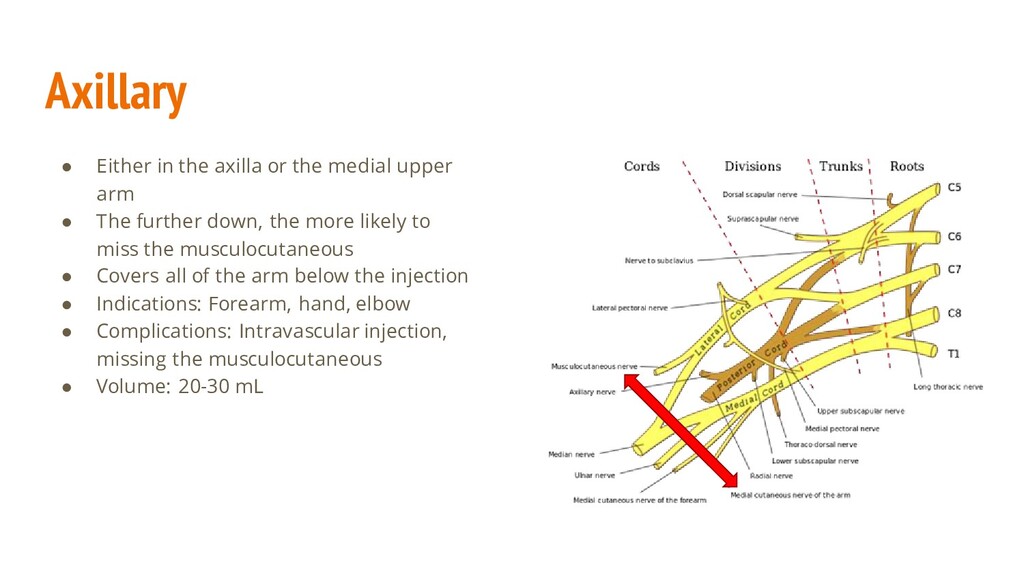
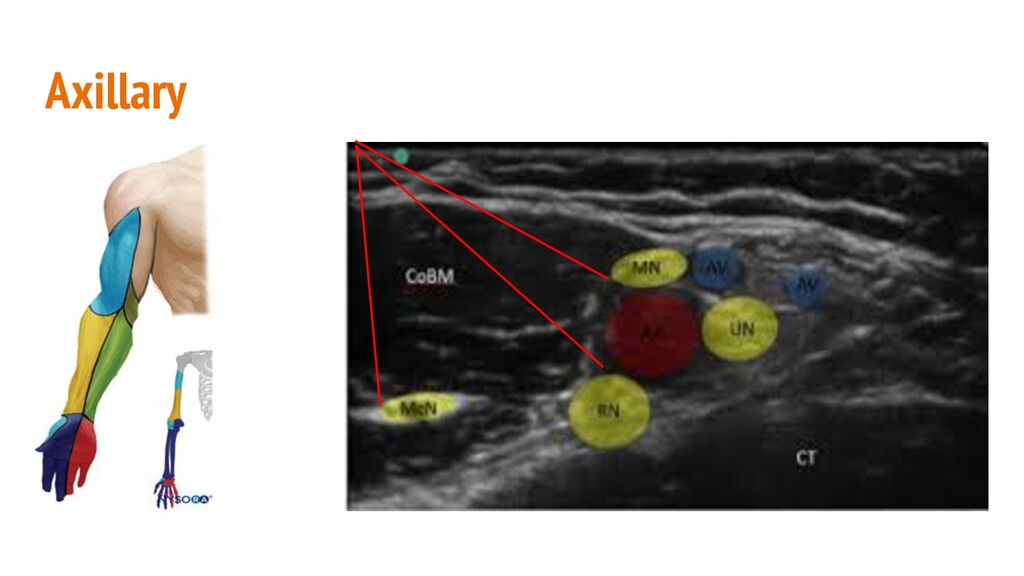
arm • The further down, the more likely to miss the musculocutaneous • Covers all of the arm below the injection • Indications: Forearm, hand, elbow • Complications: Intravascular injection, missing the musculocutaneous • Volume: 20-30 mL
Orthopedic population • Surgical anesthesia ◦ Orthopedics ◦ Vascular ◦ Podiatry • Increased hemodynamic stability compared to neuraxial • Unilateral • Lumbosacral plexus ◦ Sciatic and femoral nerves ◦ All joints innervated by both • May alter patient’s dispo plan ◦ Motor weakness ◦ Rehab vs home ◦ Overnight admission
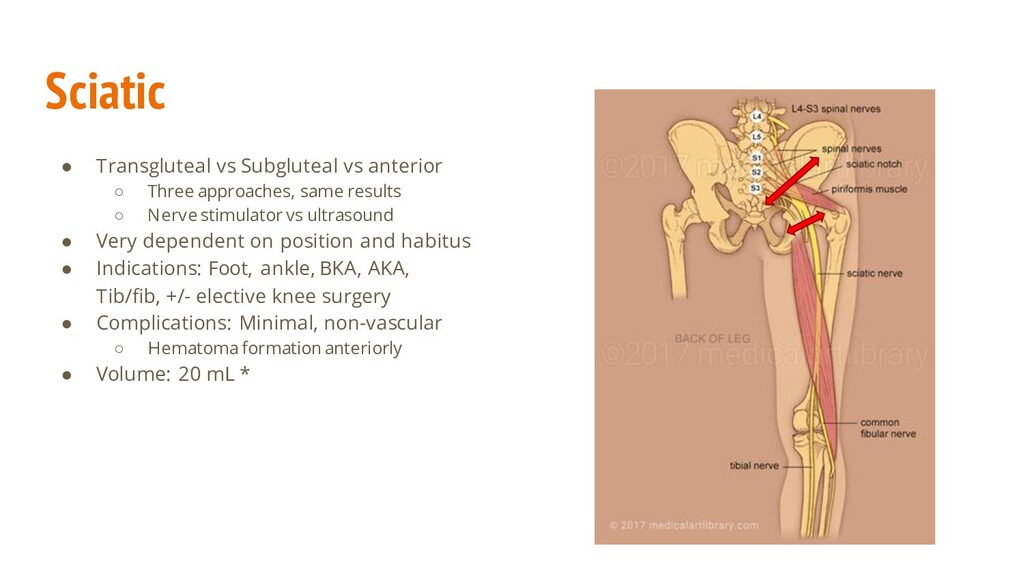
same results ◦ Nerve stimulator vs ultrasound • Very dependent on position and habitus • Indications: Foot, ankle, BKA, AKA, Tib/fib, +/- elective knee surgery • Complications: Minimal, non-vascular ◦ Hematoma formation anteriorly • Volume: 20 mL *
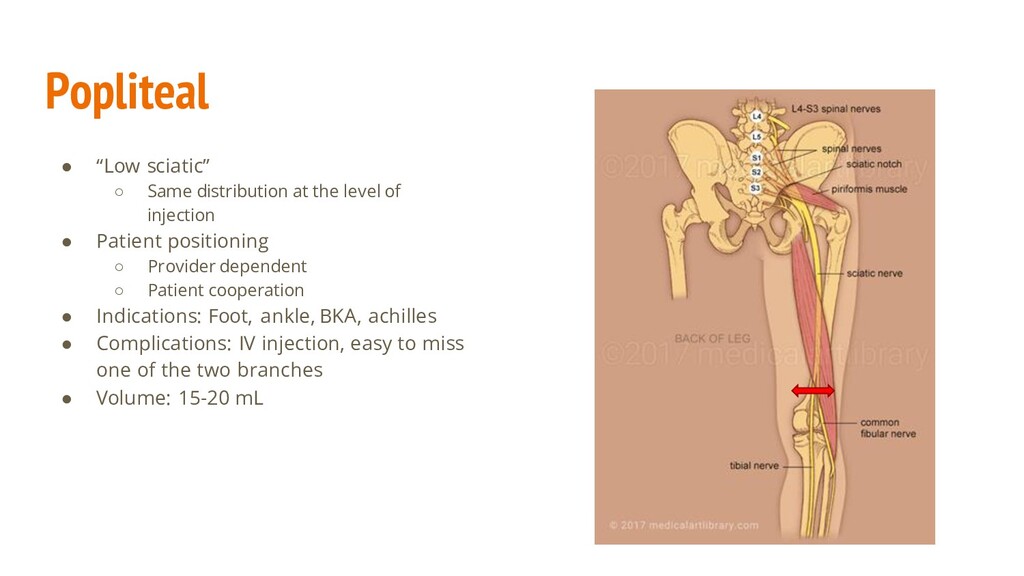
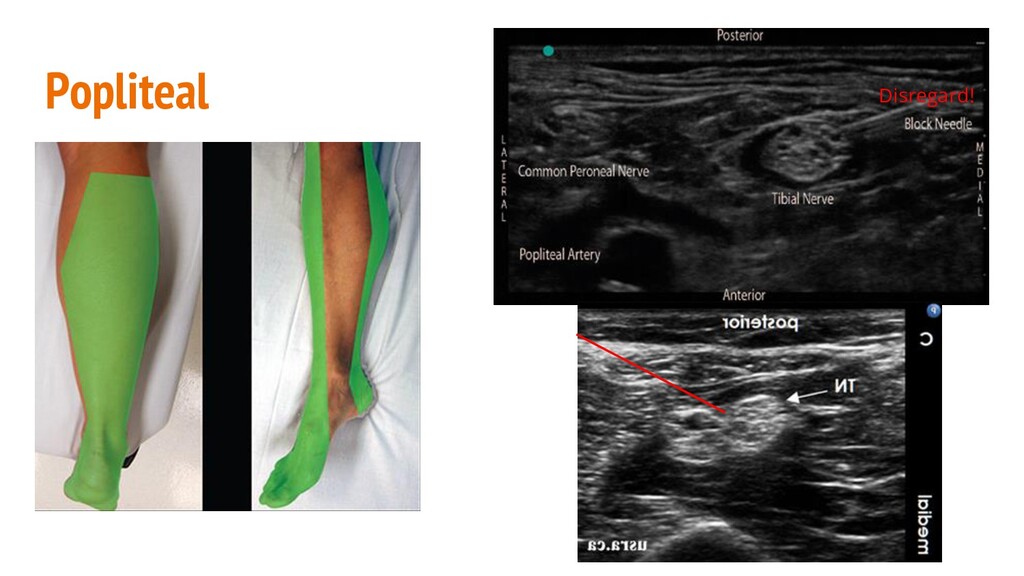
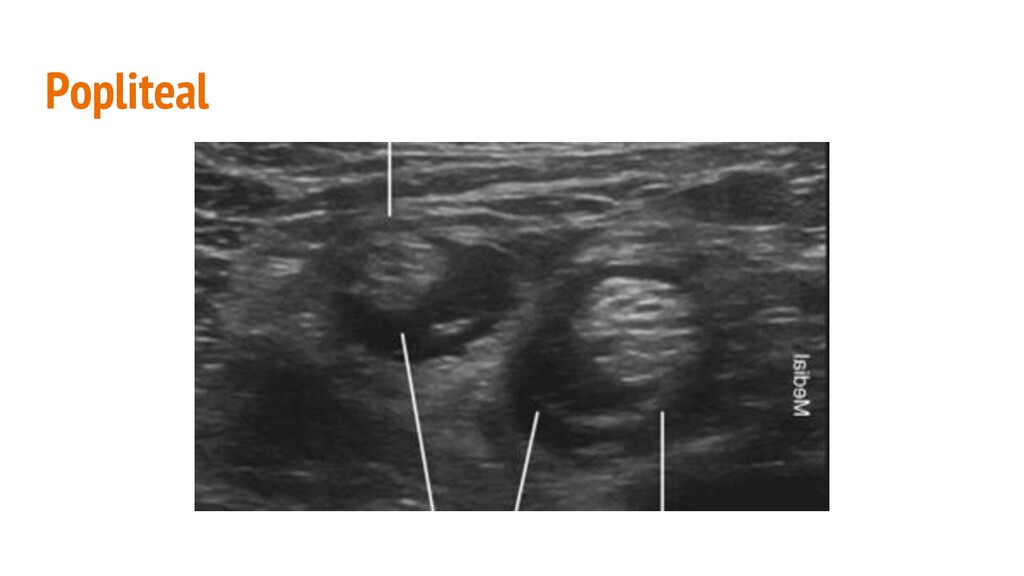
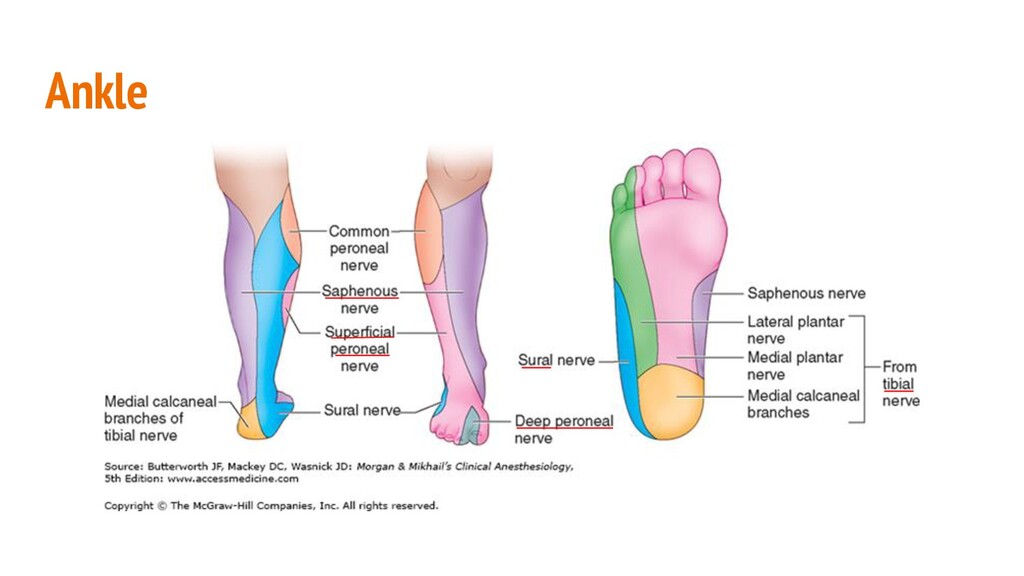
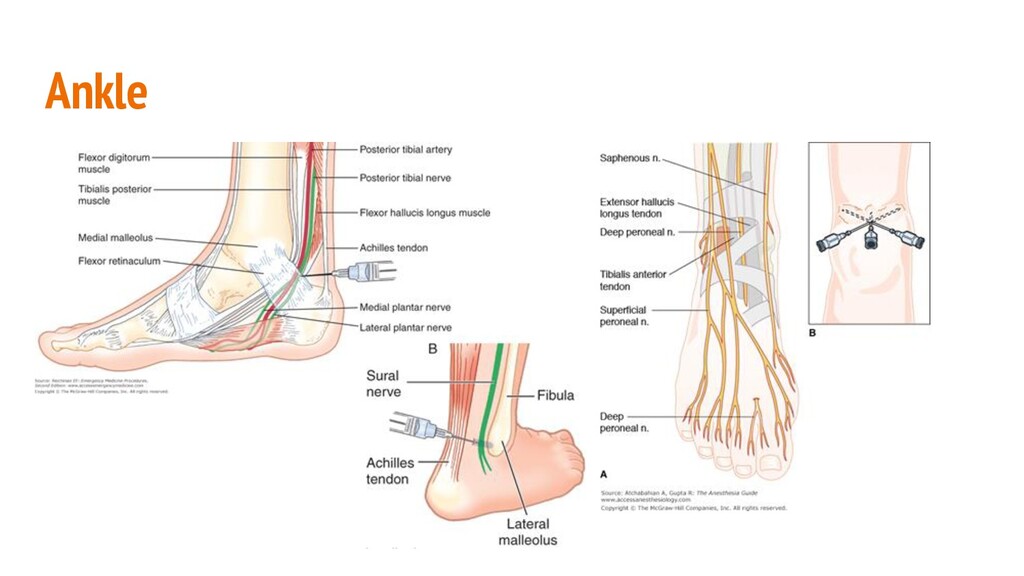
of injection • Patient positioning ◦ Provider dependent ◦ Patient cooperation • Indications: Foot, ankle, BKA, achilles • Complications: IV injection, easy to miss one of the two branches • Volume: 15-20 mL
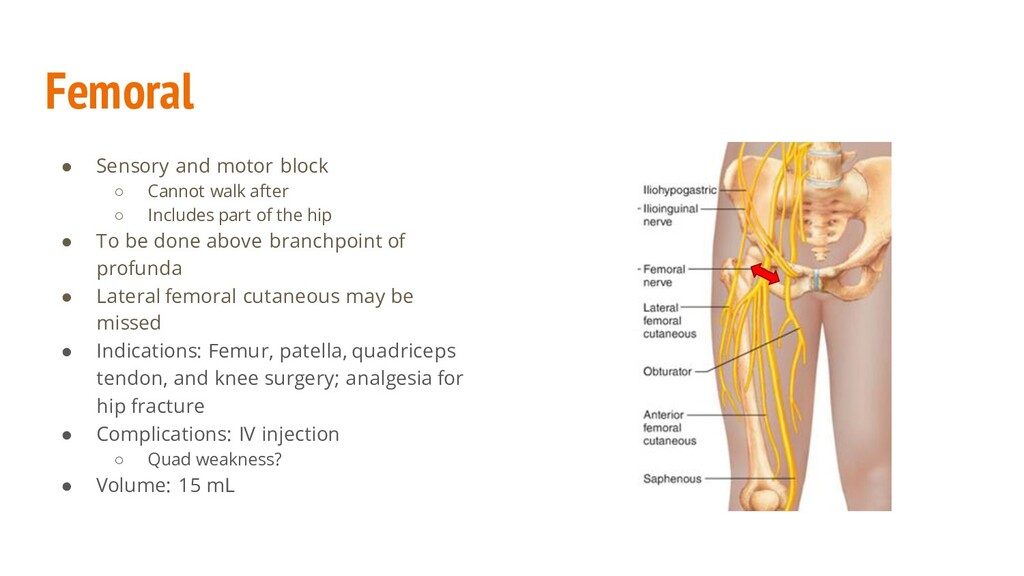
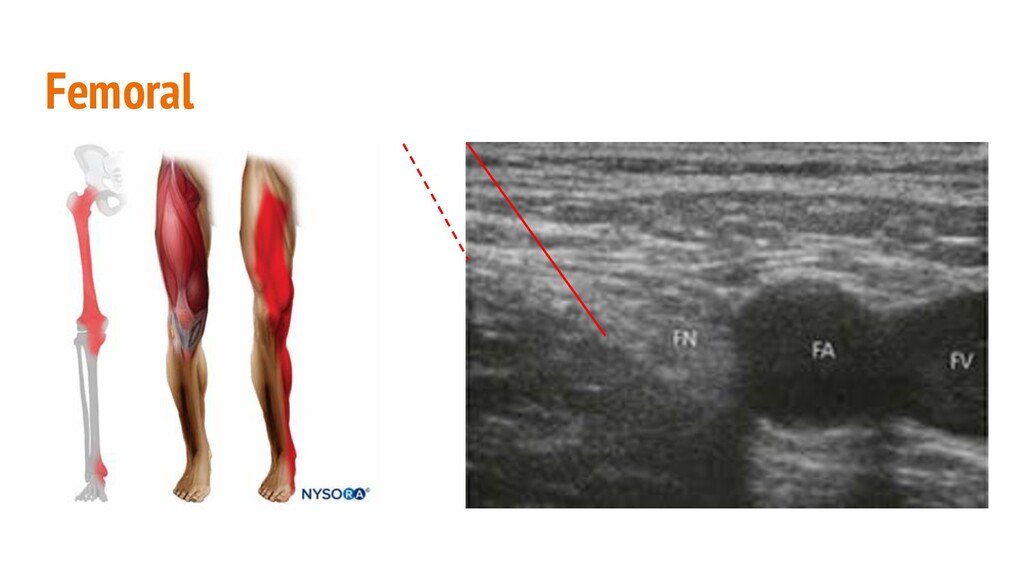
◦ Includes part of the hip • To be done above branchpoint of profunda • Lateral femoral cutaneous may be missed • Indications: Femur, patella, quadriceps tendon, and knee surgery; analgesia for hip fracture • Complications: IV injection ◦ Quad weakness? • Volume: 15 mL
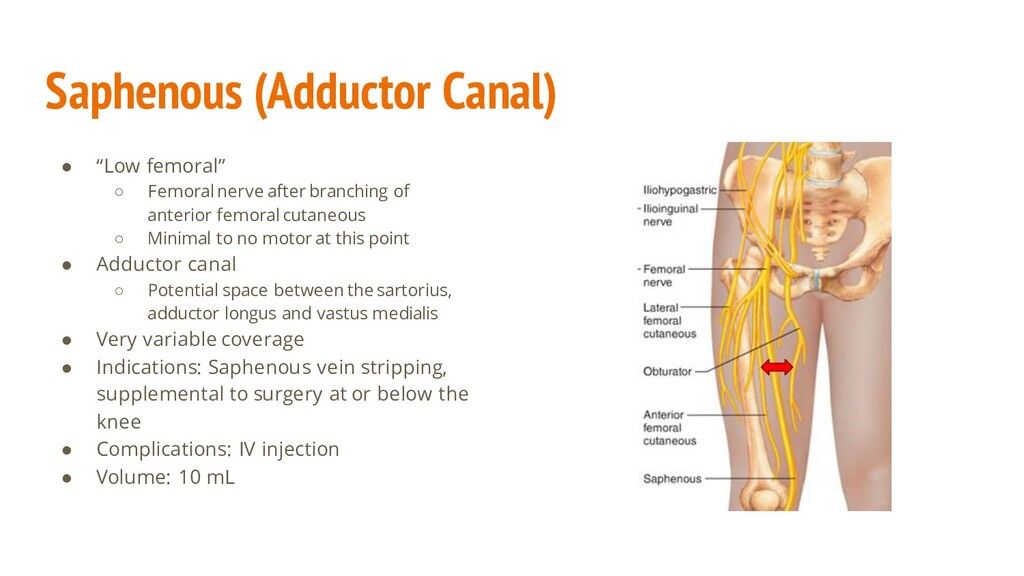
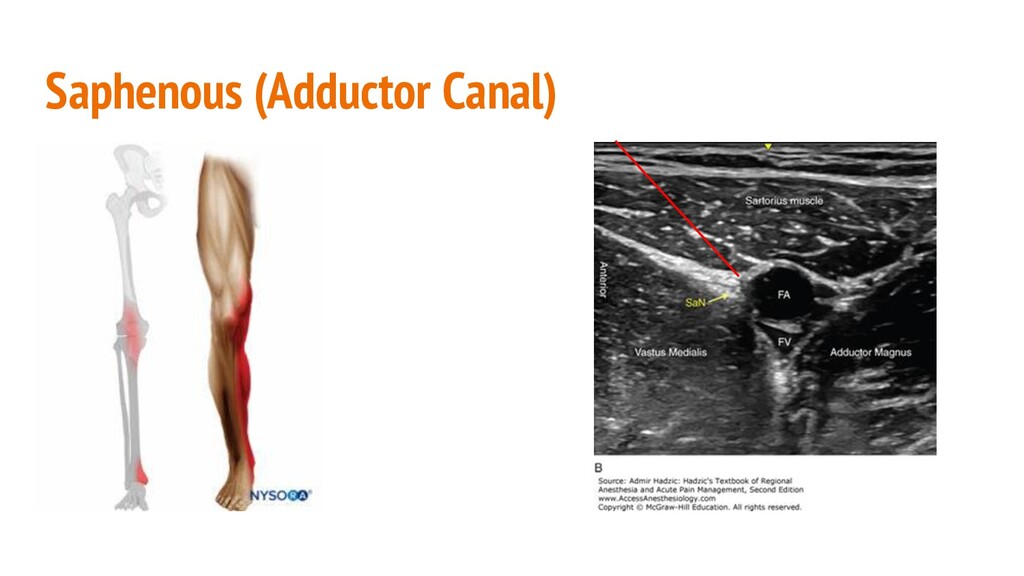
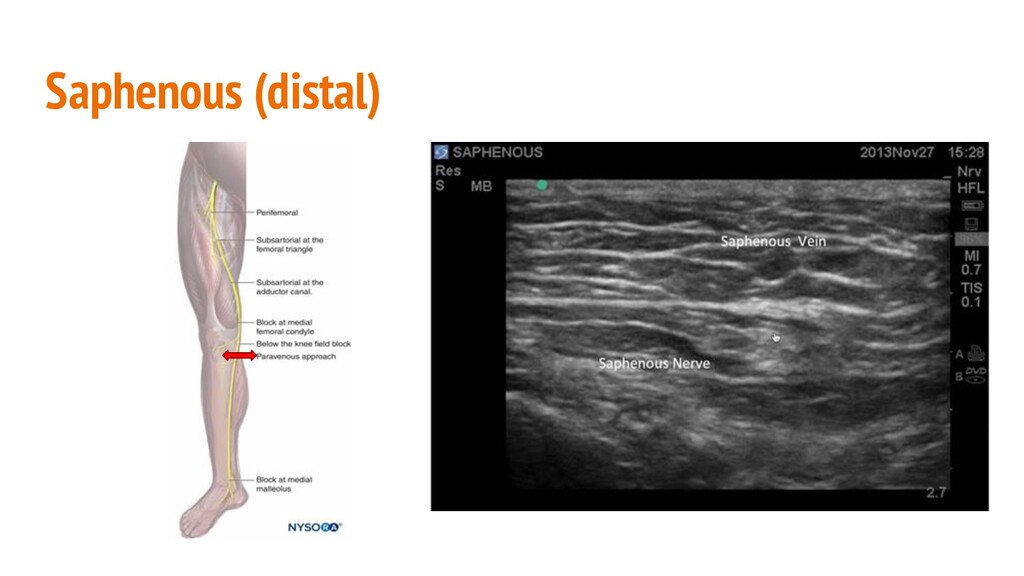
branching of anterior femoral cutaneous ◦ Minimal to no motor at this point • Adductor canal ◦ Potential space between the sartorius, adductor longus and vastus medialis • Very variable coverage • Indications: Saphenous vein stripping, supplemental to surgery at or below the knee • Complications: IV injection • Volume: 10 mL
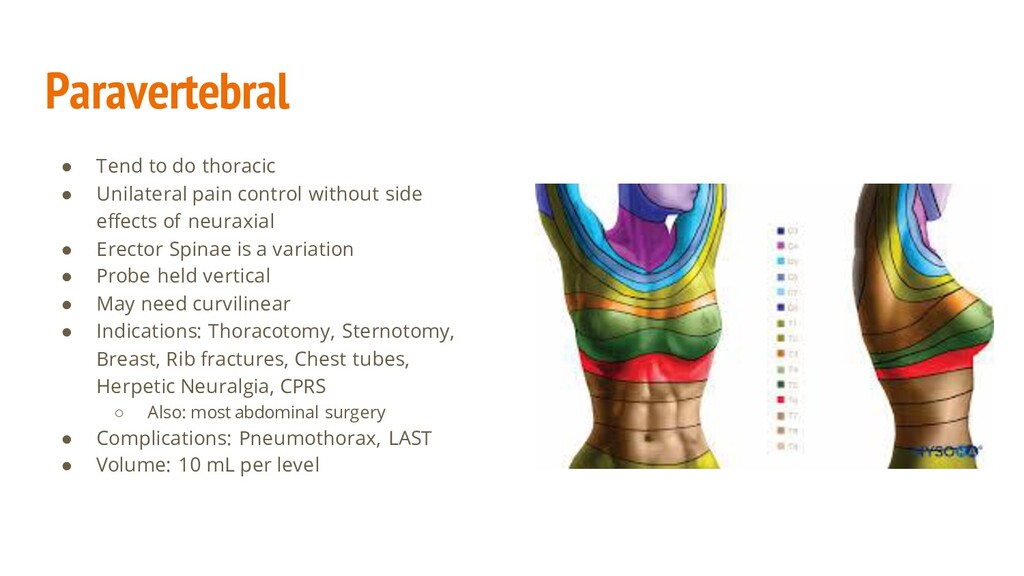
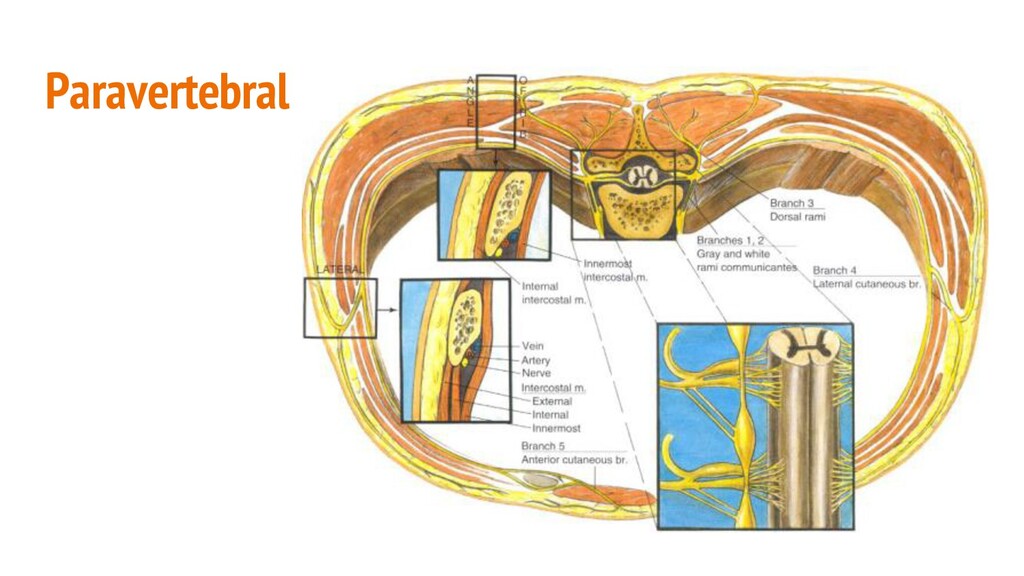
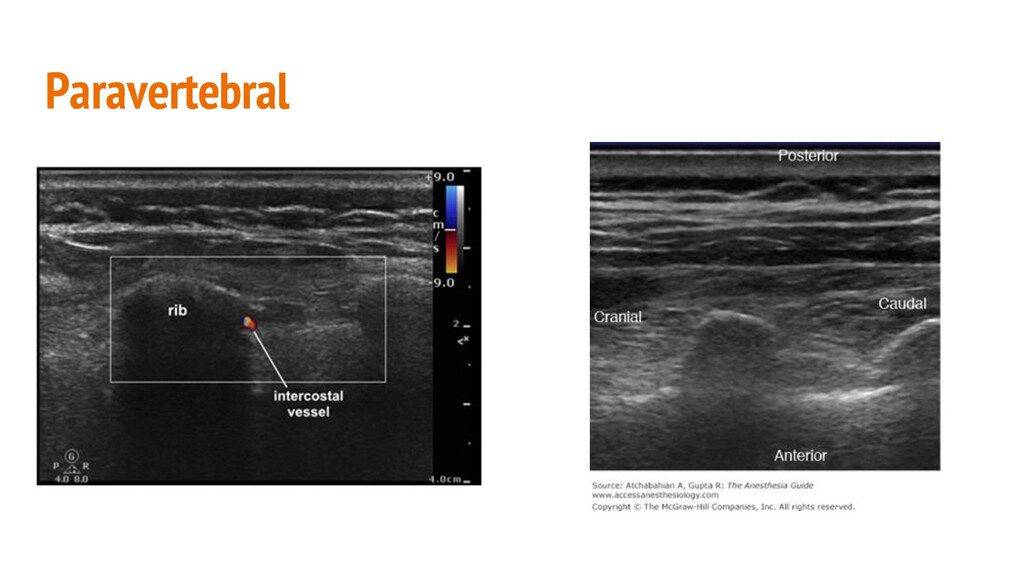
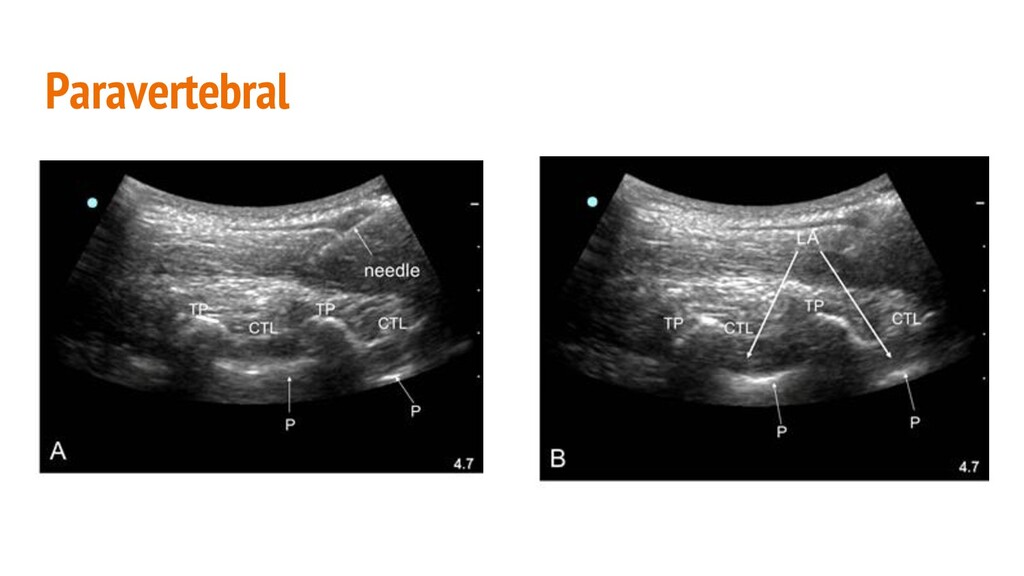
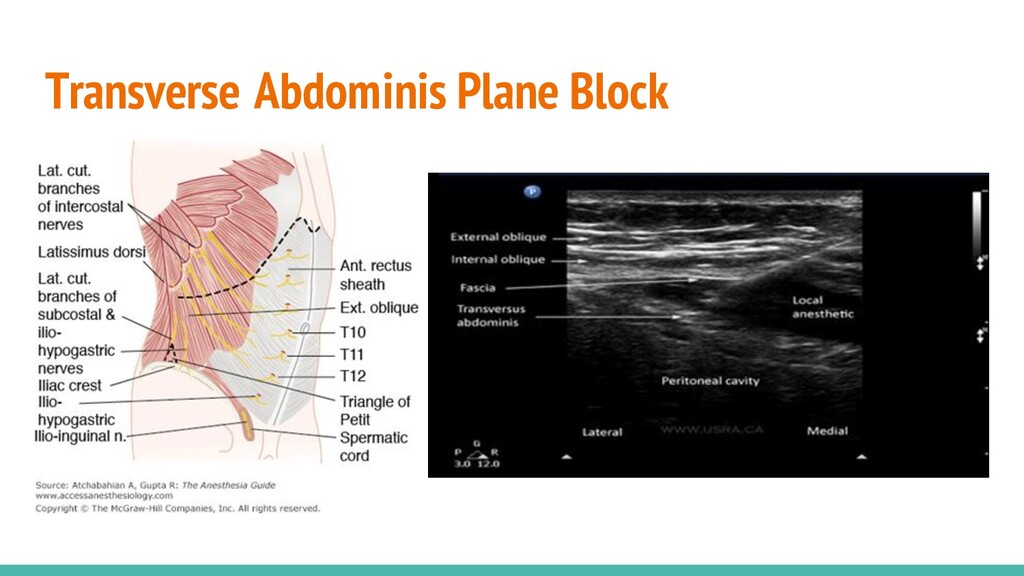
without side effects of neuraxial • Erector Spinae is a variation • Probe held vertical • May need curvilinear • Indications: Thoracotomy, Sternotomy, Breast, Rib fractures, Chest tubes, Herpetic Neuralgia, CPRS ◦ Also: most abdominal surgery • Complications: Pneumothorax, LAST • Volume: 10 mL per level
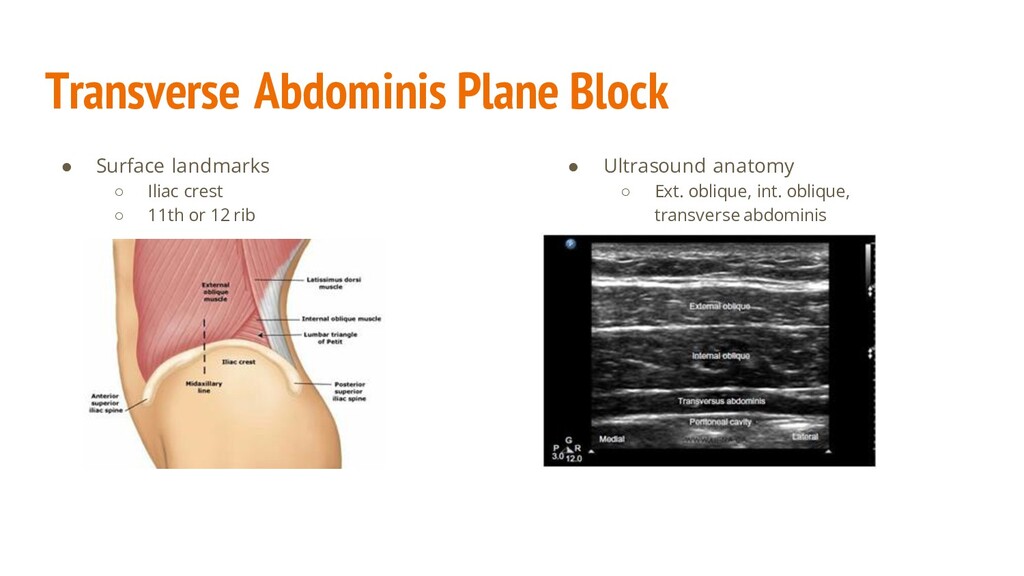
from approximately T6-L1 * ◦ The subcostal nerve (T12) ◦ The iliohypogastric and ilioinguinal nerves (L1) ◦ *The intercostal nerves (T6/7-T10/11) are not typically involved, but the TAP can be modified to include these nerves • Analgesia provided to the parietal peritoneum, muscle, and skin ◦ Does not provide analgesia to the viscera ◦ Variable efficacy • Indications ◦ Abdominal surgery, primarily below the umbilicus ◦ More effective in surgeries with a lesser degree of organ manipulation • Risks ◦ Infection, bleeding, bowel perforation
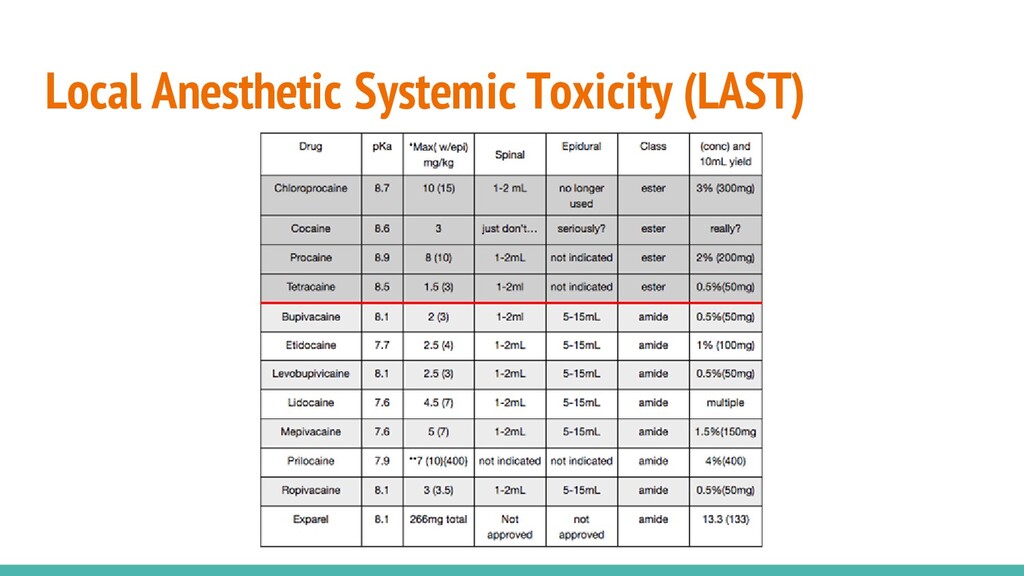
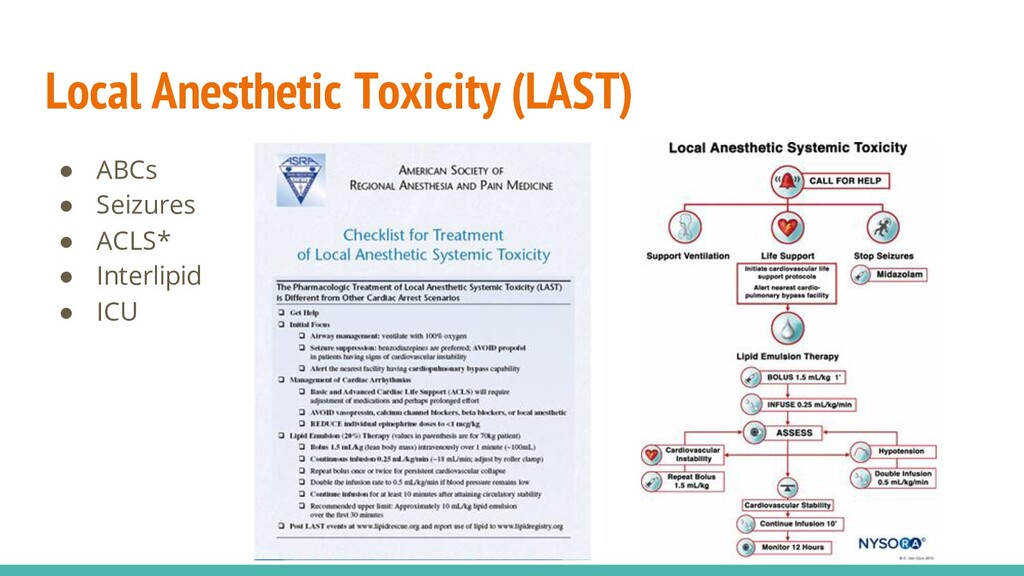
injection of local anesthetics or from absorption of deposited local anesthetic • Local anesthetics bind to and inhibit sodium and calcium channels ◦ Local anesthetics can accumulate in cardiac tissue ◦ Lethal due to cardiac dysrhythmias • Symptoms: ◦ Altered mental status, perioral numbness, tinnitus, agitation, dysarthria, and confusion. ◦ Seizures, coma. ◦ Hypertension and tachycardia, followed by hypotension and bradycardia followed by ventricular arrhythmias and asystole. • Onset: usually within the first minute after injecting.
◦ Type of local anesthetic - lipophilic have increased risk of toxicity ◦ Location of injection - intercostals, epidural, brachial plexus, lower extremity ◦ Larger doses ◦ Patient risk factors - renal or hepatic dysfunction, underlying disease process, protein binding ◦ Extremes of age - possibly from decreased muscle mass ▪ Mild symptoms in young children will be missed • Occurrence ◦ Peripheral blocks - 1.6-2/1000 in 1990, now 0.08-0.98/1000 ◦ Epidural - 9.75/1000 in 1980s, 0.1-1.2/1000 in 1990s, now 0.1/1000
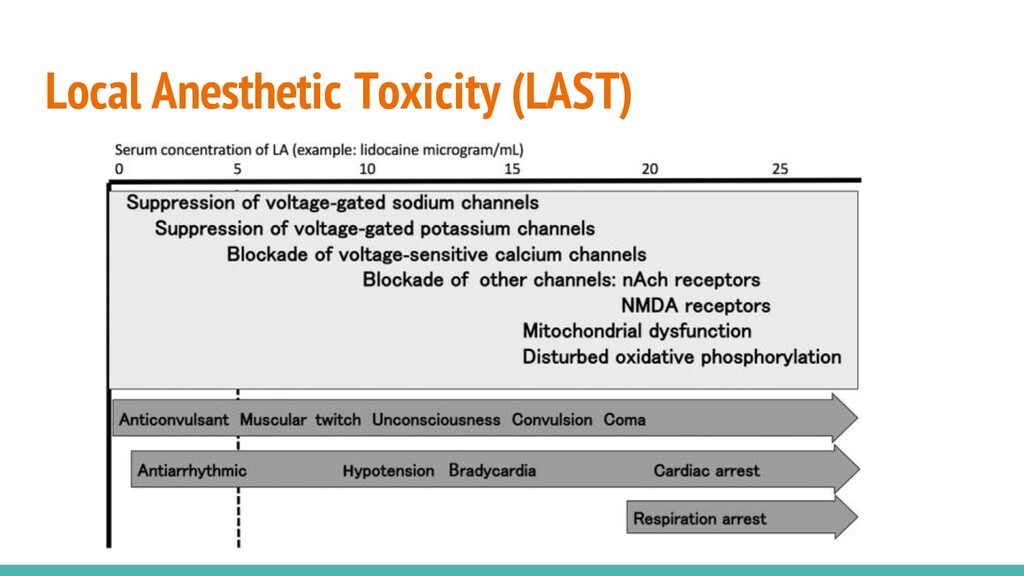
Acute Pain Management Second Edition Sekimoto K, Tobe M, Saito S. Local anesthetic toxicity: acute and chronic management. Acute Med Surg. 2017;4(2):152–160. Published 2017 Mar 6. doi:10.1002/ams2.265
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}