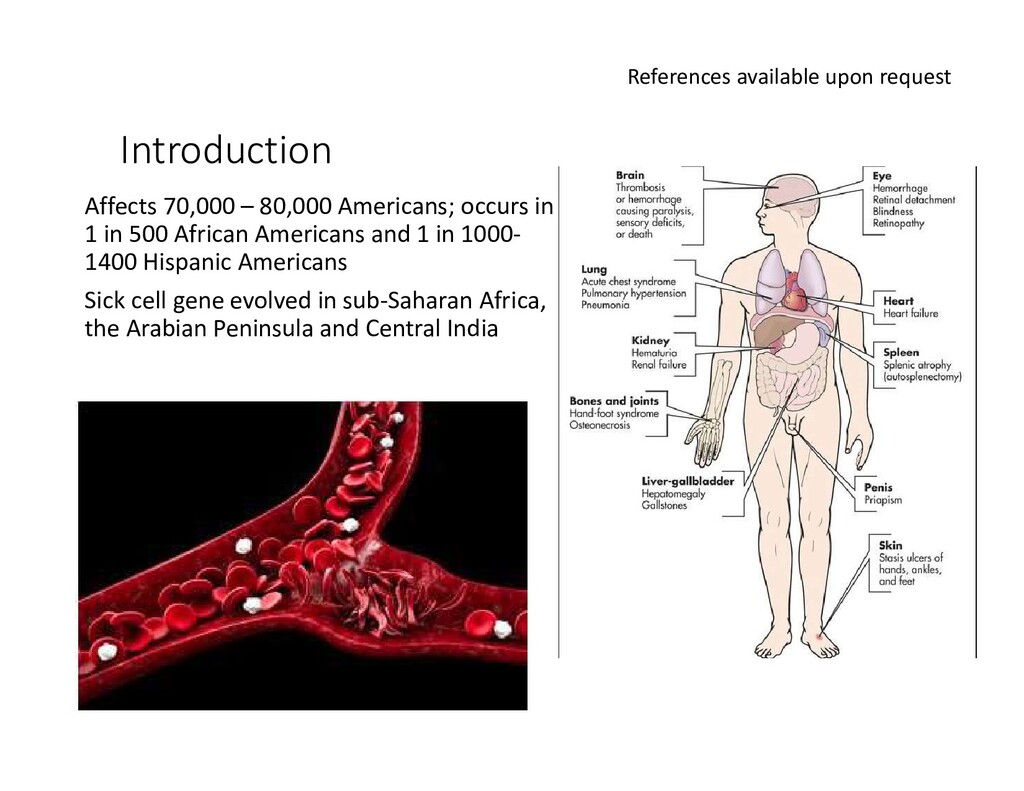
500 African Americans and 1 in 1000- 1400 Hispanic Americans Sick cell gene evolved in sub-Saharan Africa, the Arabian Peninsula and Central India References available upon request
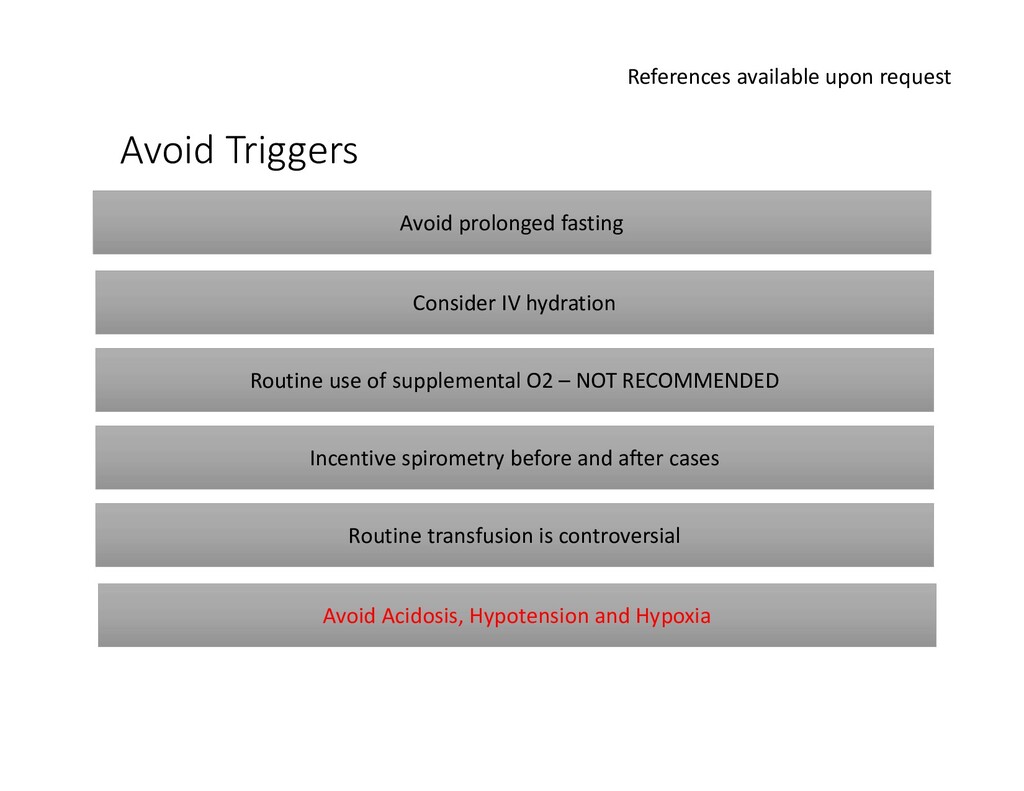
IV hydration Routine use of supplemental O2 – NOT RECOMMENDED Incentive spirometry before and after cases Routine transfusion is controversial Avoid Acidosis, Hypotension and Hypoxia
hypoventilation leading to respiratory acidosis • Intubation after paralysis with a short-acting agent • Maintain saturation >92% and OR temperature no less than 24C • There are no absolute contraindications to sedation in patients with SCD; • General Anesthesia can be safely administered with volatile or intravenous agents References available upon request
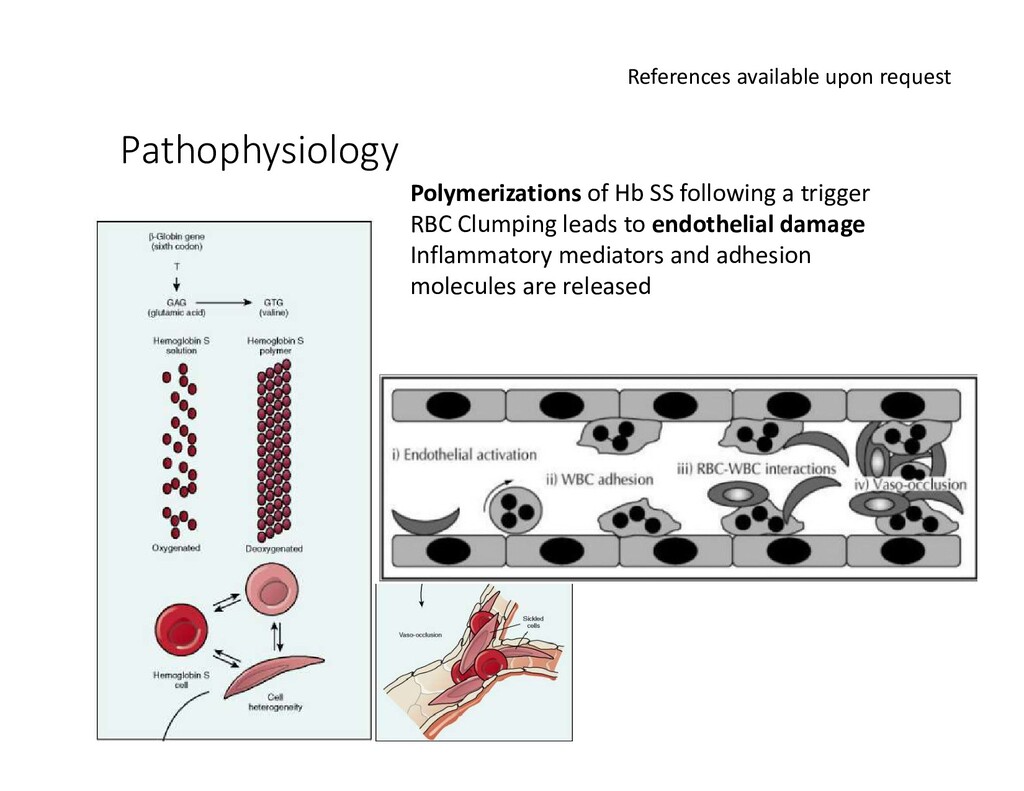
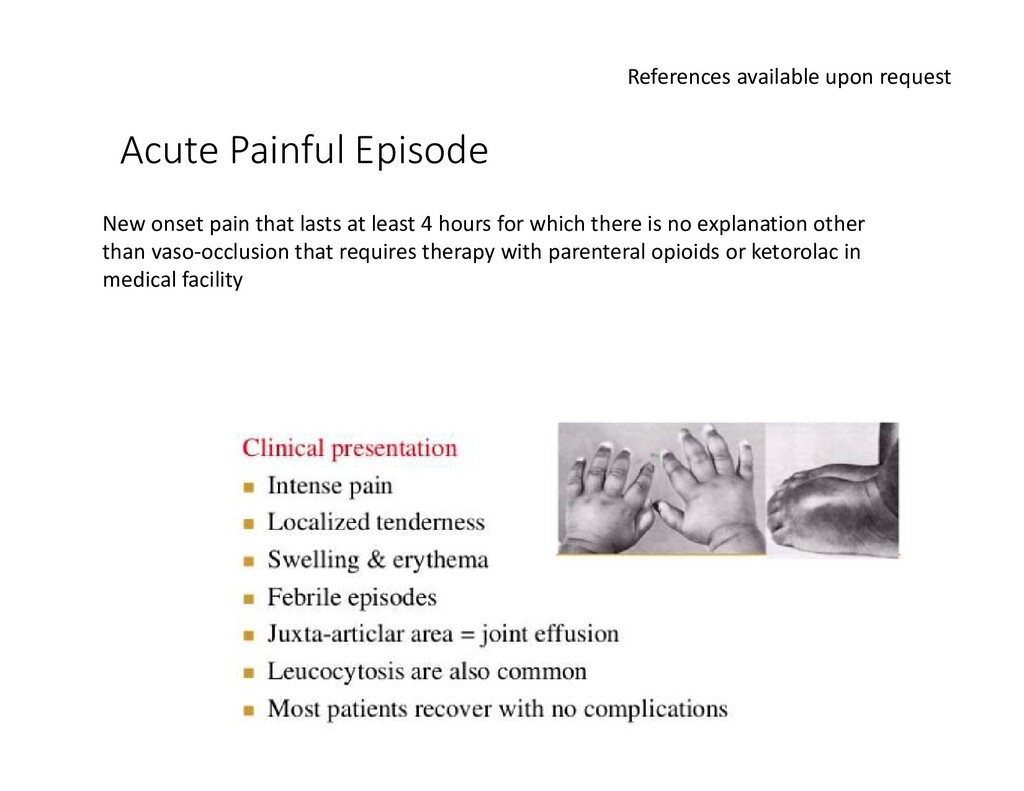
that lasts at least 4 hours for which there is no explanation other than vaso-occlusion that requires therapy with parenteral opioids or ketorolac in medical facility
Non-pharmacologic • Heat/cold packs, distraction, relaxation, massage, music, acupuncture • Pharmacologic • Nonopioids (Acetaminophen, NSAIDS, topical agents and corticosteroids) • Opioids (mu-agonists, mixed agonists/antagonist buprenorphine and partial agonist pentazocine) • Adjuvants (Antihistamines, benzodiazepines, antidepressants, anticonvulsants) • Regional Techniques • Local anesthetics via neuraxial blocks or peripheral nerve blocks can be used but patients should be monitored closely as there have been case reports of sickle cell crises induced peripheral neuropathy after neuraxial blocks • Transfusion • No data that supports routine transfusion; does not shorten the duration of a pain crisis
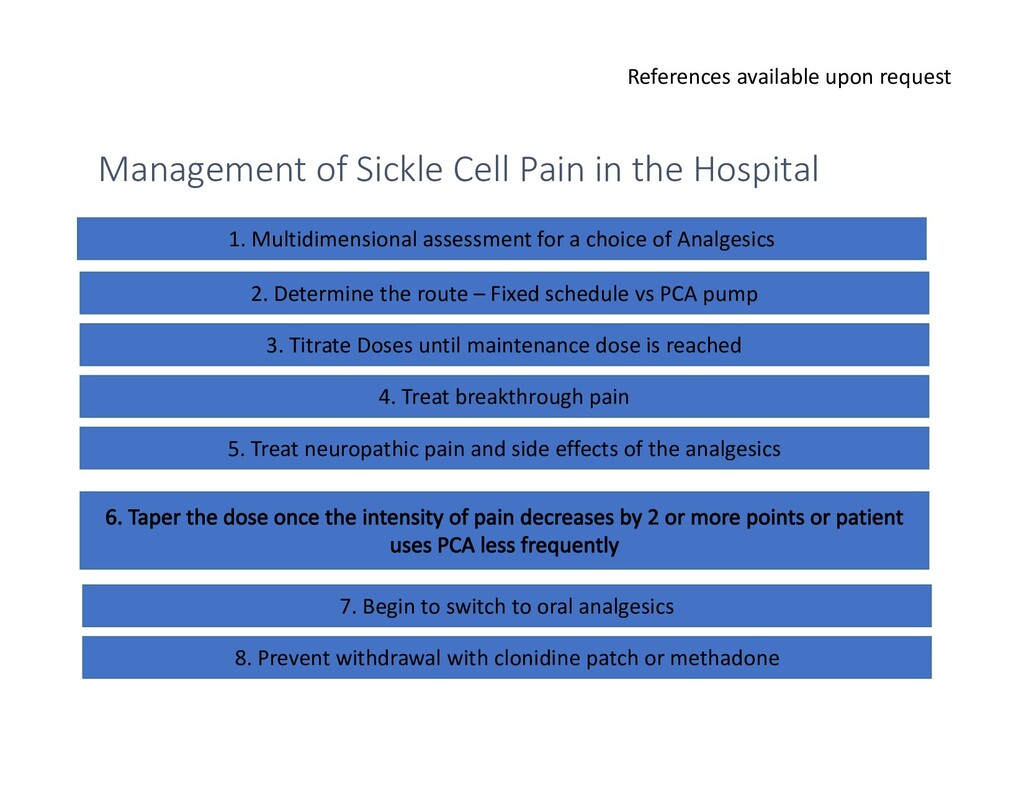
the Hospital 1. Multidimensional assessment for a choice of Analgesics 2. Determine the route – Fixed schedule vs PCA pump 3. Titrate Doses until maintenance dose is reached 4. Treat breakthrough pain 5. Treat neuropathic pain and side effects of the analgesics 7. Begin to switch to oral analgesics 8. Prevent withdrawal with clonidine patch or methadone
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}