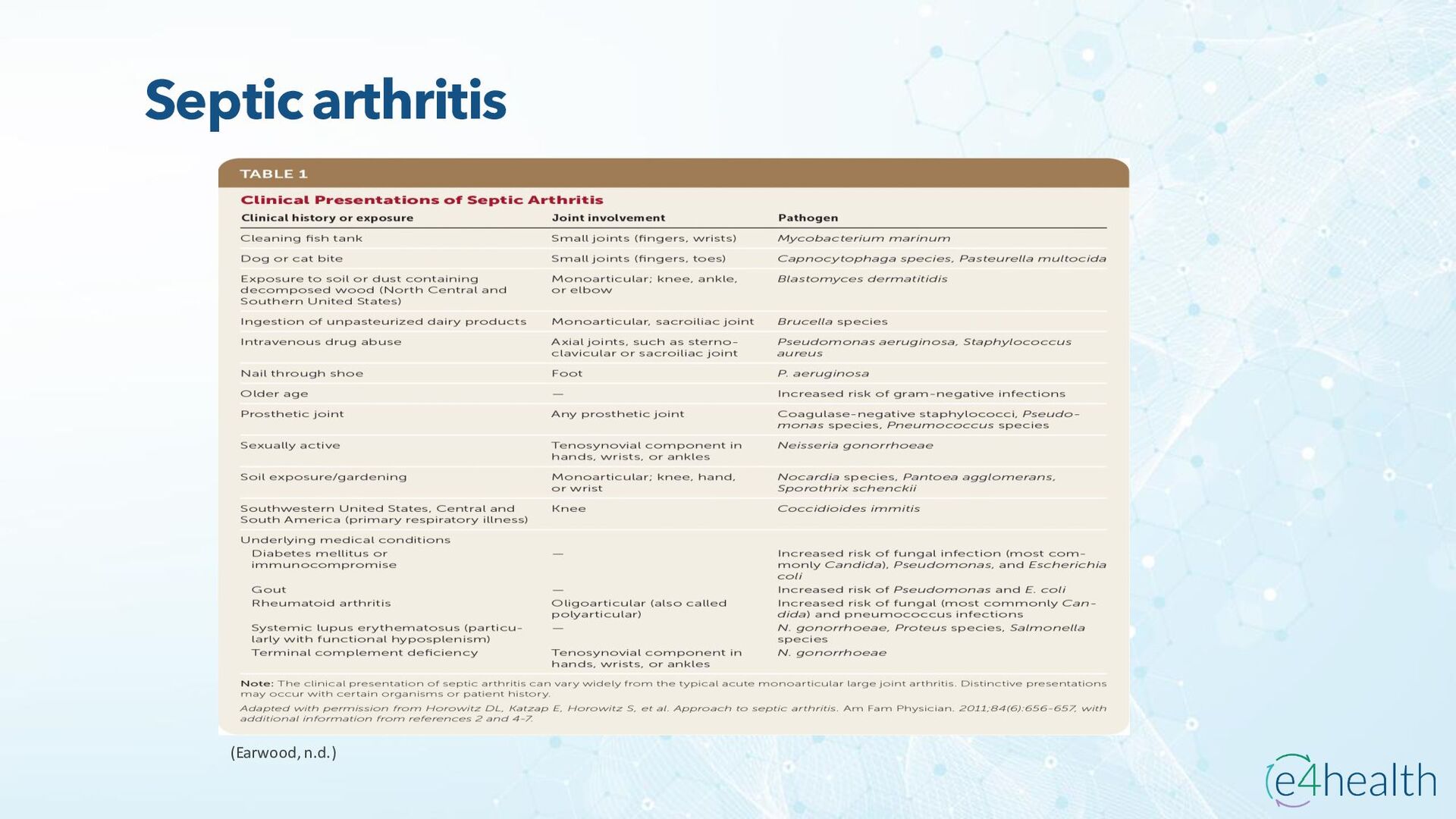
https://www.hopkinsmedicine.org/health/conditions -and- diseases/ankylosing-spondylitis • Chauhan K, Jandu JS, Brent LH, et al. Rheumatoid Arthritis. [Updated 2023 Jan 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441999/ • Chen, Leon L. DNP, AGACNP-BC, FCCP, FAANP, FNYAM; Fasolka, Brian PhD, RN, CEN; Treacy, Caitlin MS, AGACNP-BC. Necrotizing fasciitis: A comprehensive review. Nursing 50(9):p 34-40, September 2020. | DOI: 10.1097/01.NURSE.0000694752.85118.62 • Earwood, J. S. (n.d.). Septic Arthritis: Diagnosis and Treatment. AAFP. https://www.aafp.org/pubs/afp/issues/2021/1200/p589.html#afp20211200p589-t1 • Facr, W. C. S. J. M. F. (2023, April 17). Aseptic Necrosis Causes, Symptoms, Treatment, Medications, Prevention. MedicineNet. https://www.medicinenet.com/aseptic_necrosis/article.htm • Gastrointestinal stromal tumor: MedlinePlus Genetics. (n.d.). https://medlineplus.gov/genetics/condition/gastrointestinal-stromal- tumor/#:~:text=A%20gastrointestinal%20stromal%20tumor%20%28GIST%29%20is%20a%20type,of%20Cajal%20%28ICCs%29%20or %20precursors%20to%20these%20cells. • Groner, L. K., Green, D. J., Weisman, S. V., Legasto, A. C., Toy, D., Gruden, J. F., & Escalon, J. G. (2021). Thoracic Manifestations of Rheumatoid Arthritis. Radiographics, 41(1), 32–55. https://doi.org/10.1148/rg.2021200091
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}