12 – Ileal Strictures, perianal abscesses – Several years on Pentasa, 2 resections • Now in deep remission on ADA + MTX • Decides to stop meds, use marijuana instead • Does “fine” for 6 months, misses clinic appt – Turns up in ER in month 7 – Perianal abscess, active inflammation, new SB stricture – + Antibodies to adalimumab
Maintenance of remission reduces hospitalizations and surgery and improves patients’ quality of life – The word “maintenance” appears 63 times in the guideline – The words “de-escalation” or “step down” do not appear at all. – “Stay with what Got you to Remission” approach Lichtenstein, G., et al. AJG 3 104:465–483 2009.
– Never steroids – Never hospitalized – Never significant endoscopic disease or complications • The ileal CD discovered at screening colonoscopy – May not need any therapy • The mild proctitis patient who uses 5-ASA suppositories for 8 weeks a year
stop wearing my seat belt (maintenance therapy). If not - Minimize risk! - Monitor for near misses - Go back to seat belts if/when he has a near miss Your patients are thinking this right now. Try to talk them out of it.
Patient Factors Am I cured? Did I even really have IBD? Do I still need this therapy? Magical Thinking Some don’t want to self- identify as a sick person
taking this medication, and you can’t make me take it anymore. But I want you to be responsible for the outcome of my decision. A cry for help – can we renegotiate Rx?
Flares disrupt life, hurt QoL – Are family, spouse supportive of this risk-taking? • Steroid rescue AE Rate >> therapy AE rate • Antibodies: Biologic may not work if stop/restart – Anti-biologic antibodies could be result
azathioprine can take a thiopurine holiday – 53% had clinical flare by 3 years – Lower risk if CRP <2 mg/L, Hgb >12, ANC <4.0 • CD patients on IFX/Aza can step down to Aza – 43% had clinical flare by 1 year – CRP >5 mg/L or FCP >300 mg/g predicted flare 3-6 months before Treton, CGH 7: 80-85, 2009. Louis, Gastro, 142: 63-79, 2012.
Biologic Remission – Low CRP and FCP, high hemoglobin, no ulcers • Willing and able to do frequent monitoring of inflammation – Every 12 weeks – NPV for flare w/FCP<167: 100% Gisbert, IBD 15: 1190-98, 2009.
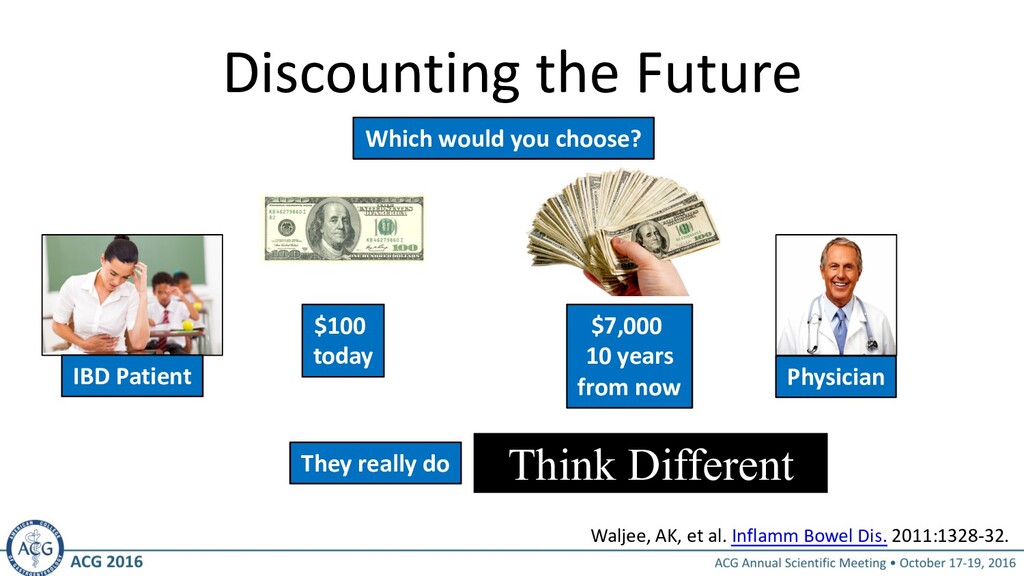
pain, symptoms - Can’t plan for future, can’t count on the future Wants relief NOW, wants low risk NOW Thinks about the future - Invested years of training (pain now) for future benefits - Can plan for future, can count on the future Willing to take small risks now for future benefits Discount Rate 3-5% 55% Waljee, AK, et al. Inflamm Bowel Dis. 2011:1328-32.
in the past • Low rate of bowel damage, complications, surgeries – Have been in BIOLOGIC remission for >1 year – Willing to do q 12 week monitoring – Have proven reliable in the past
for a big flare? – Could cost you time from work/home – Time in hospital, unable to support family • Are you willing to take big steroids when you flare? • Understand it could take months to return to remission? • Are you prepared for risk that we may not be able to get you back in remission, and you may need surgery? • Will you agree to more frequent testing in place of meds? • When you flare, are you willing to go back on medication?
– Full dose immunomodulator for at least 12 weeks before stopping a biologic – Continue IMM for at least 12 weeks after discontinuing the biologic – Prevent Abs to allow restart later (88%) – Confirm plan with patient Louis, Gastro, 142: 63-79, 2012.
of inflammation – Does CRP identify flares in this patient? – Does fecal calprotectin? – If not, scope and scan • Practical? Does patient really want this? – Plan on an objective measure every 12 weeks – Document biologic remission with scope at 6 months after step down
worries about anti-drug antibodies • Do need to monitor closely – Biomarkers q 12 weeks • Documented plan to restart if inflammation returns • Confirm remission with scope at 6 m Higgins, PDR, AJG 106: 556-8, 2011.
medication – Pre-emptively start the difficult conversation – Detect patients experimenting with skipped doses • Consider the consequences before de-escalation – Respect the disease! – Maintenance = Standard of Care • Make it a shared decision • Have a clear plan to: – Avoid anti-drug antibodies – Objectively monitor inflammation q 12 weeks – Step up therapy when inflammation returns
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}