Remission ~ 15-55% of the time • Lots of patients are treatment-refractory • Is this just difficult-to-treat inflammation? • Is there a single damaged segment? • Are symptoms due to a structural problem? • Is treatment being blocked (Anti-Biologic Abs, poor perfusion)? • Do we need better / combination therapies? • Is there an immunologic defect / genetic mutation?
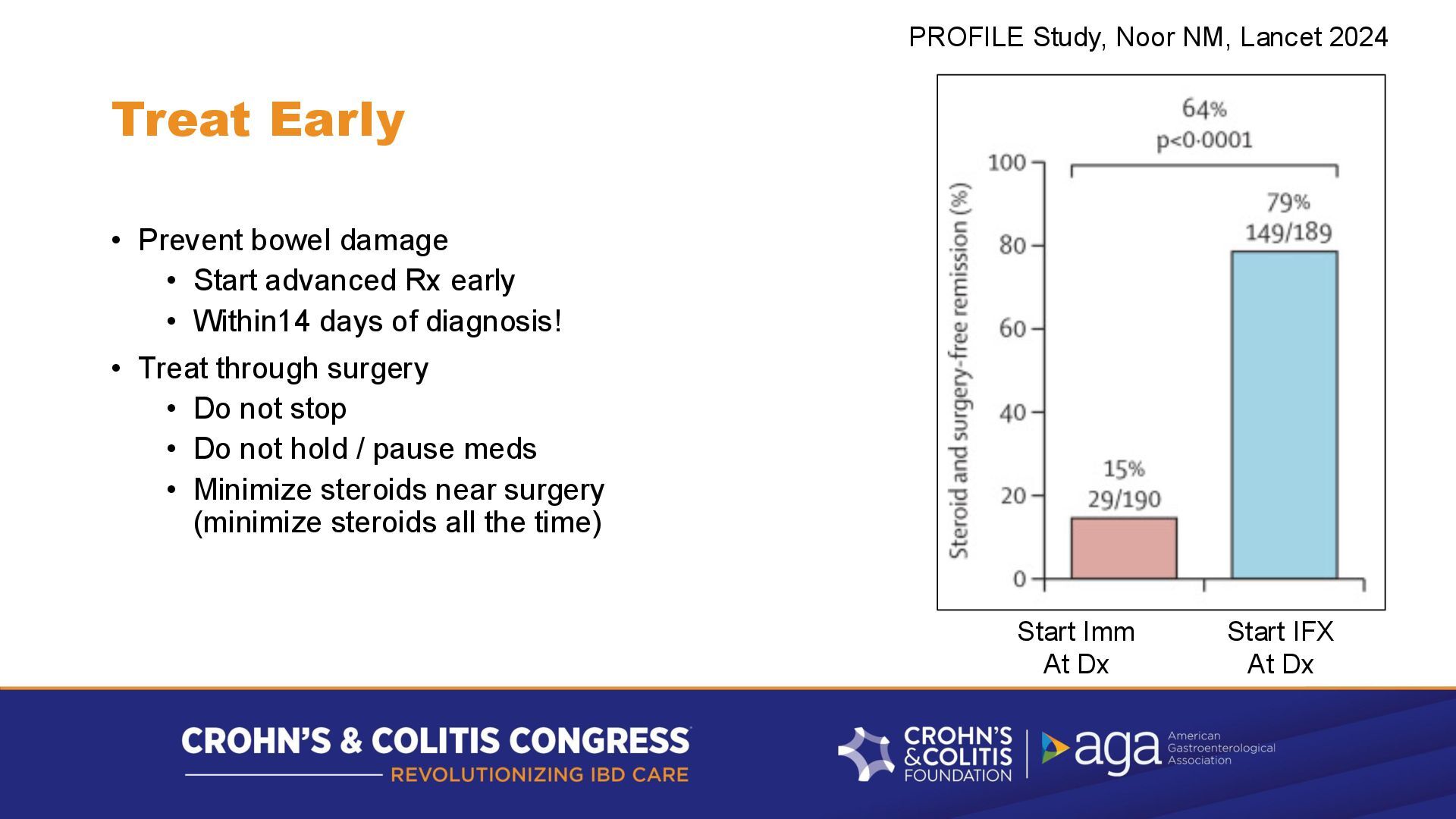
early • Within14 days of diagnosis! • Treat through surgery • Do not stop • Do not hold / pause meds • Minimize steroids near surgery (minimize steroids all the time) PROFILE Study, Noor NM, Lancet 2024 Start Imm At Dx Start IFX At Dx
fairly “mousy” o Prone to Anti-Biologic Antibody (ABA) formation, not very durable o Watch drug levels, ABA levels, choose to Adjust or Exit • Newer biologics o More human, less ABA prone o Better binding to target cytokines – serum levels are less important • Small molecules (JAKi, S1PR) – 'invisible' - no antibodies
biologic • More drug / shorter interval? – can buy time • But commit to an exit strategy • Don't fight with insurance for weeks while bowel damage is accumulating • Generally, CHANGE your MoA for better outcomes • Don't delay a MoA switch when it is needed – • Monitor response to dose/interval change • If it is not great, change to avoid more bowel damage • Four MoAs to choose from • TNF, IL-23, Anti-integrin, JAKi (S1PR)
or contraindications to some (CHF, demyelinating disease) • Which prior MoA did best / lasted longest? • Was it an ABA LoR (loss of response)? – try a different drug in the same MoA • Were levels too low w/o ABA? Re-try at higher dose/shorter interval • Were prior ‘adverse events’ truly drug-related? • Often disease-related (hair loss) > drug, or unrelated • If revisiting a prior drug class with LOR due to ABA • Consider Aza 50 / Allo 100 Combo with Biologic for up to 4 years (PANTS) • Consider a small molecule to get to smoldering, then start a Biologic
TNFi, Vedo, p19i, JAKi without repeating meds • Some marginal gains ~ 5-15% for clinical remission, but not truly closing the therapeutic gap • Vedolizumab (anti-integrin) probably safest (?), good in combinations • MUCH more data needed on Combos
in Crohn's • Several segments get better with a new advanced Rx • One or two segments do not • Is it Time to switch Rx? • Bad segments may be too severely damaged • May have fibrosis and poor blood flow, limiting drug delivery • Take the win • Resect or strictureplasty the damaged segments • Treat the rest of the bowel with the effective drug
seen on imaging • Upstream dilation can come and go proximal to early strictures • Penetrating complications (fistula, abscess) are usually associated with an adjacent stricture or sphincter • Make sure to identify, dilate any local or downstream strictures • Consider (esp. if recurrent) surgical strictureplasty or resection • Consider endoscopic strictureplasty if available
before 25, consider late presentation of VEO • Treatment-refractory IBD – seek help before the 3rd MoA • Panel testing for monogenic causes – find your team, or refer to an IBD Center for help Pediatric GI Jeremy Adler Immunohematopathology Kelly Jo Walkovich
well on Abatacept • 20% fail – 30 BM/d - Abatacept to 18 BM/d • did well on Abatacept + Upadacitinib – case report • XIAP mutation case- most do well on Anakinra • Anakinra is pretty good, with intermittent budesonide is better • IL-18BP (tadekinig alfa) is now in clinical trials • Consider BMT if an intractable monogenic cause of IBD is found
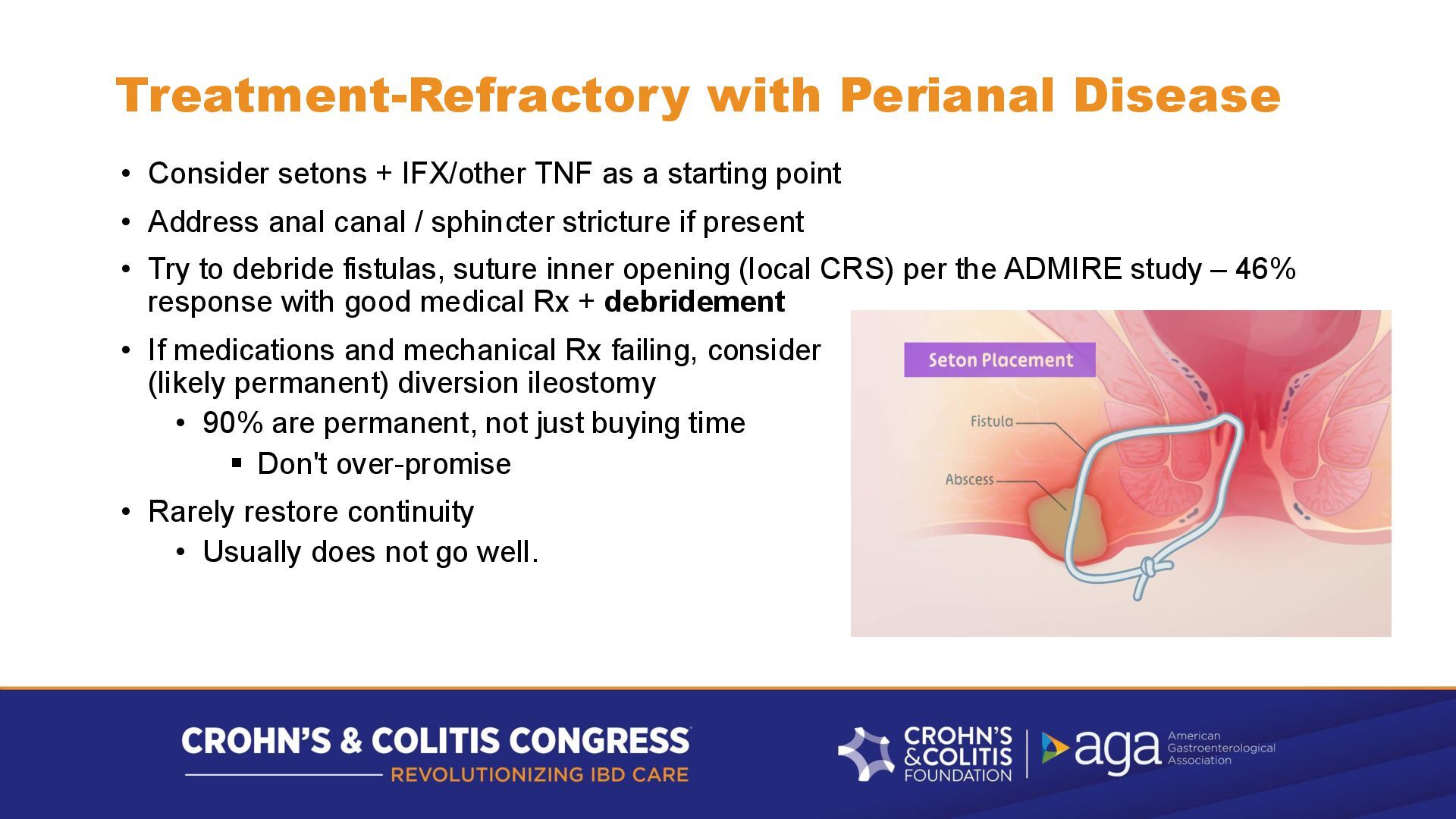
as a starting point • Address anal canal / sphincter stricture if present • Try to debride fistulas, suture inner opening (local CRS) per the ADMIRE study – 46% response with good medical Rx + debridement • If medications and mechanical Rx failing, consider (likely permanent) diversion ileostomy • 90% are permanent, not just buying time ▪ Don't over-promise • Rarely restore continuity • Usually does not go well.
hair, nails • Think vitamin C (collagen) • Think Zinc • Think iron • Think protein • Hair – inflammation (telogen effluvium ~ 100d), A, D, E, B6, B12 • Common deficiencies – need these to heal
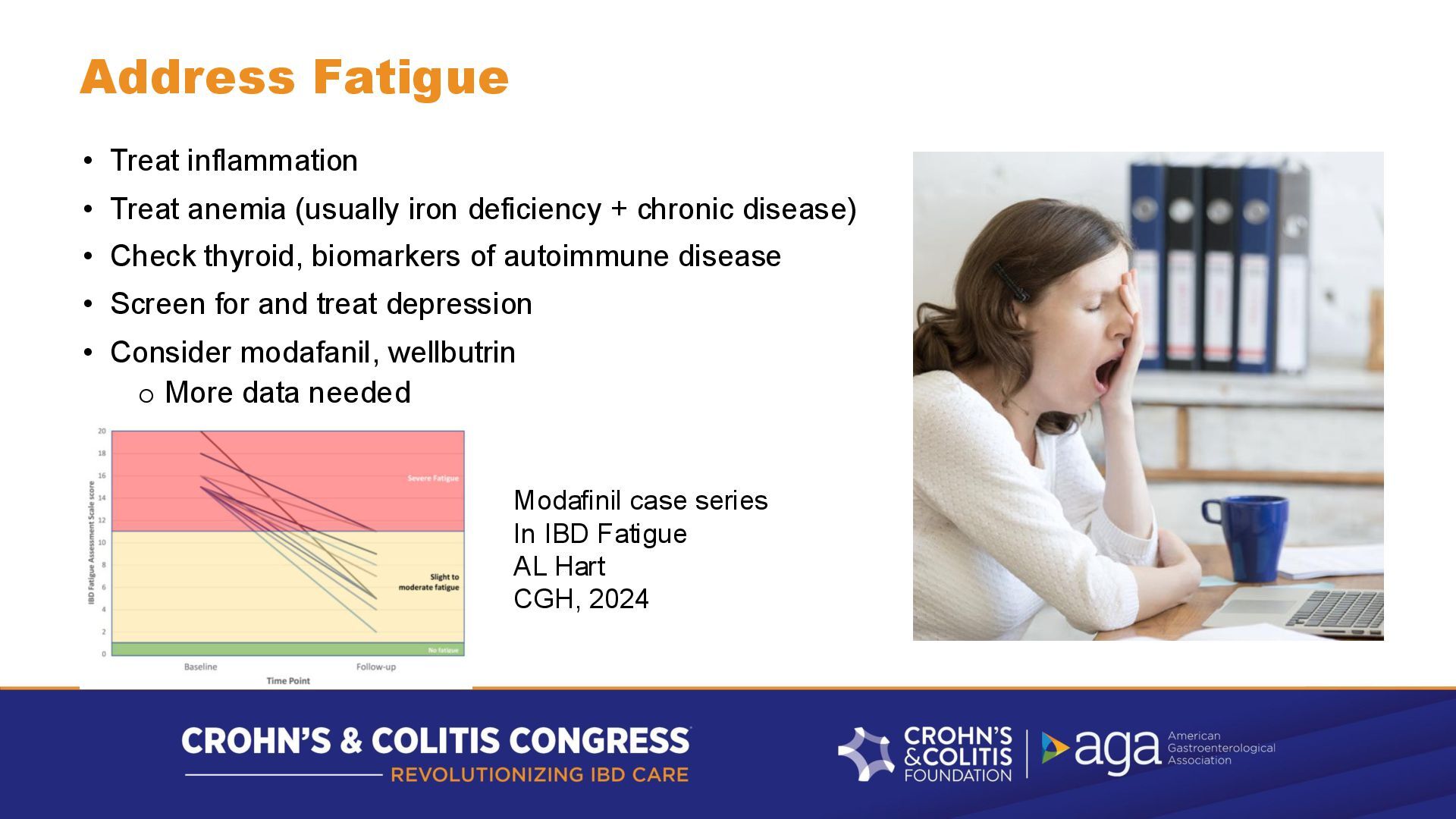
deficiency + chronic disease) • Check thyroid, biomarkers of autoimmune disease • Screen for and treat depression • Consider modafanil, wellbutrin o More data needed Modafinil case series In IBD Fatigue AL Hart CGH, 2024
rectum • Rectum heals last or not entirely • Often left with intractable proctitis • Problematic urgency has a big negative effect on QoL • Often fail 5-ASA suppositories • Often fail corticosteroids (suppository, enema) • Cyclosporine enemas failed in RCT • Consider tacrolimus suppositories (2 mg BID PR)? ▪ Often available as vaginal suppositories for lichen sclerosis/lichen planus ▪ No better than beclomethasone supp in RCT (MRKL Lie, CGH 2020) • In 2026, generic Tofacitinib suppository/foam? TBD
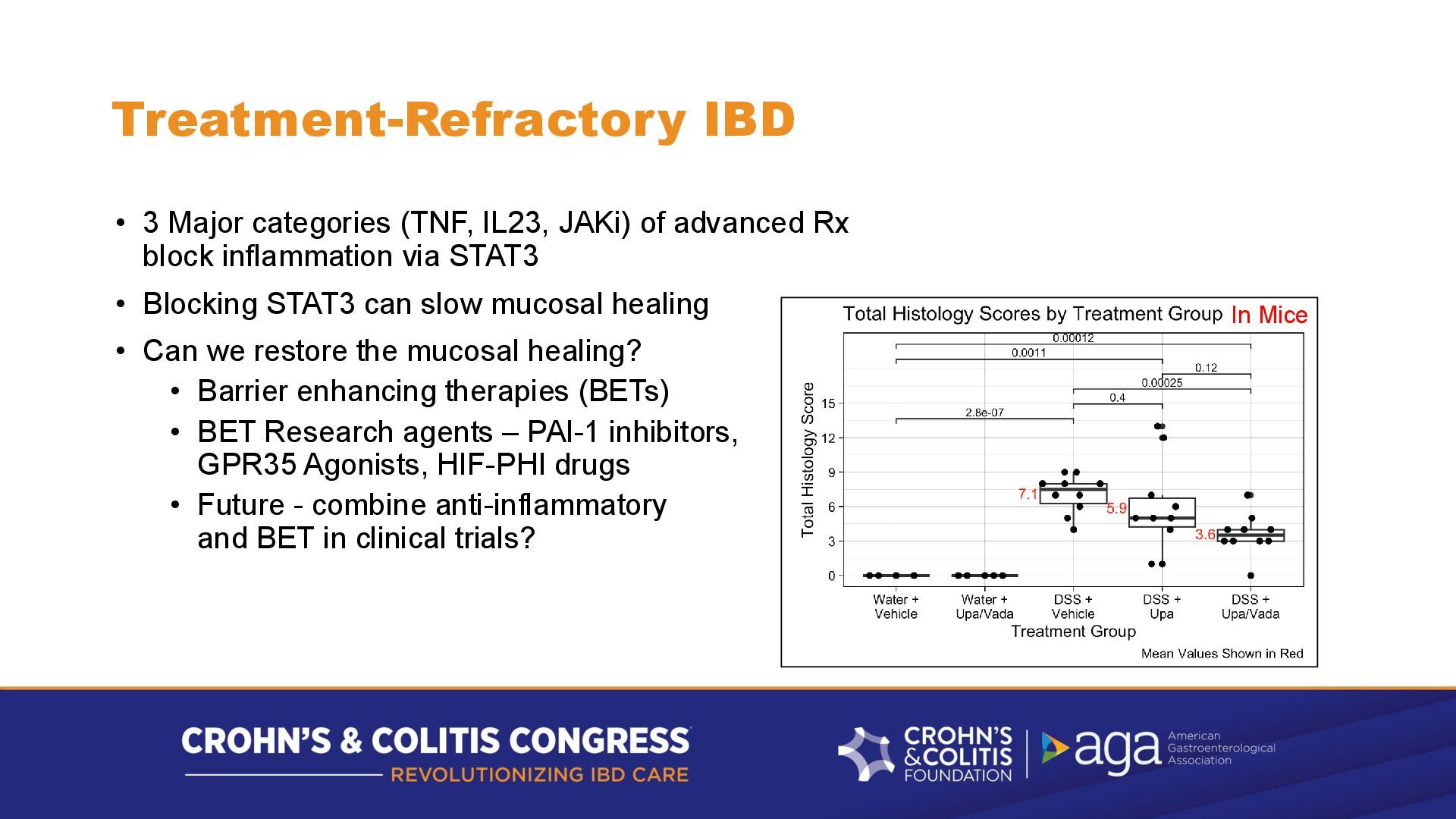
advanced Rx block inflammation via STAT3 • Blocking STAT3 can slow mucosal healing • Can we restore the mucosal healing? • Barrier enhancing therapies (BETs) • BET Research agents – PAI-1 inhibitors, GPR35 Agonists, HIF-PHI drugs • Future - combine anti-inflammatory and BET in clinical trials? In Mice
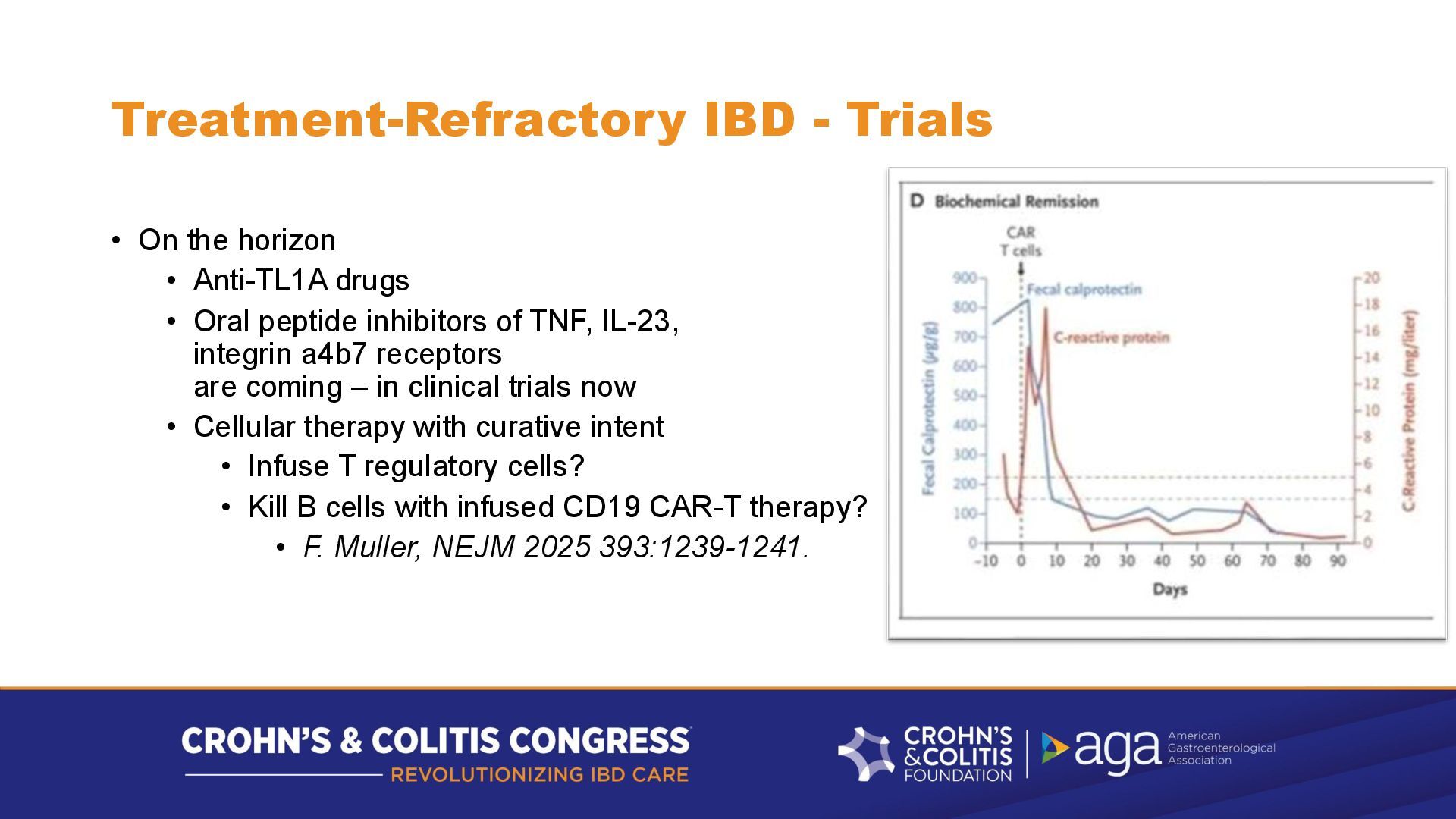
drugs • Oral peptide inhibitors of TNF, IL-23, integrin a4b7 receptors are coming – in clinical trials now • Cellular therapy with curative intent • Infuse T regulatory cells? • Kill B cells with infused CD19 CAR-T therapy? • F. Muller, NEJM 2025 393:1239-1241.
will tell your GI fellows - "Back in the 2020s, we would use steroids for refractory IBD, we rarely did genetic testing, we never used cellular therapy, and barrier-enhancing therapy was barely on the horizon" • And your fellows will have a good chuckle about how primitive IBD therapy was in the mid-2020s
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}