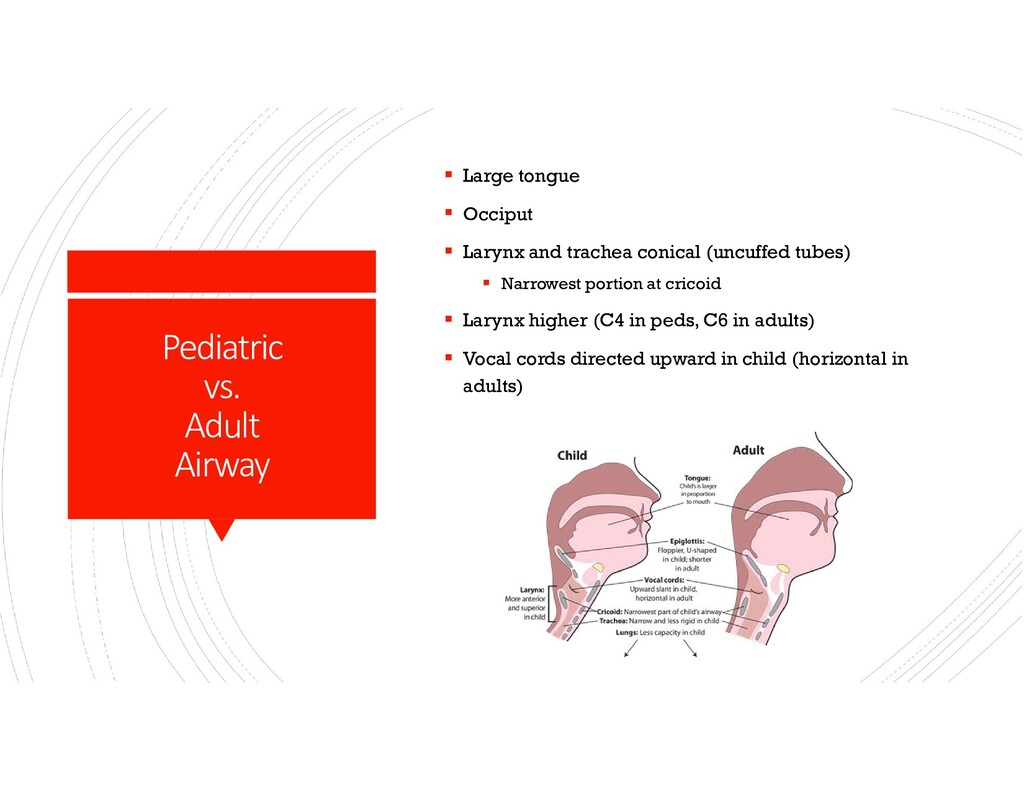
Larynx and trachea conical (uncuffed tubes) Narrowest portion at cricoid Larynx higher (C4 in peds, C6 in adults) Vocal cords directed upward in child (horizontal in adults)
liver, kidney) Malignancy within 2 years Psychiatric disorder or noncopliant behavior Substance addiction Chronic active Hep B or C, or HIV Significant chest or spinal deformity Noncurable chronic extrapulmonary infection RELATIVE Age >65 Unstable condition (shock, ECMO) Limited functional status Severe obesity Severe/symptomatic osteoporosis Colonization with highly resistant or virulent bacteria, fungi, or mycobacteria
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Immunoglobulin E Blockers Monoclonal antibodies (omalizumab [Xolair]) Prevent](https://files.speakerdeck.com/presentations/794fc9a371464b22ab18ef68db022621/slide_18.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}