able to: 1. Describe the basic alterations in cardiovascular physiology. 2. List most common changes in pulmonary physiology including a “normal” ABG in a parturient. 3. Describe changes to the gastrointestinal tract both during pregnancy and specific to labor.
of both stroke volume and heart rate • By the end of the 2nd trimester CO is elevated 40-50% above prepregnancy levels, of that approximately 25% is due to stroke volume and 15% is due to heart rate • During labor CO increases further due to uterine contractions, increased venous return and increased sympathetic activity • Immediately after delivery, CO increases even more due to autotransfusion once the placenta is delivered – This is the time that patients with pre-existing cardiac conditions are at the most risk – CO returns to nearly normal by about 2 weeks postpartum
normal blood pressure in the face of increased cardiac output, the systemic vascular resistance decreases during pregnancy • Overall decrease in systolic and diastolic blood pressure are around 10-20% and is secondary to maternal vasodilation from elevated progesterone levels as well as the presence of the low-resistance uteroplacental bed • Blood pressure nadirs at the end of the second trimester and will be close to pre-pregnancy values closer to term.
volume is approximately 40-50% higher • Dilutional anemia of pregnancy • A normal Hb at term parturient is ~11 g/ dL. • Blood volume returns to pre- pregnancy state after a little over 6 weeks
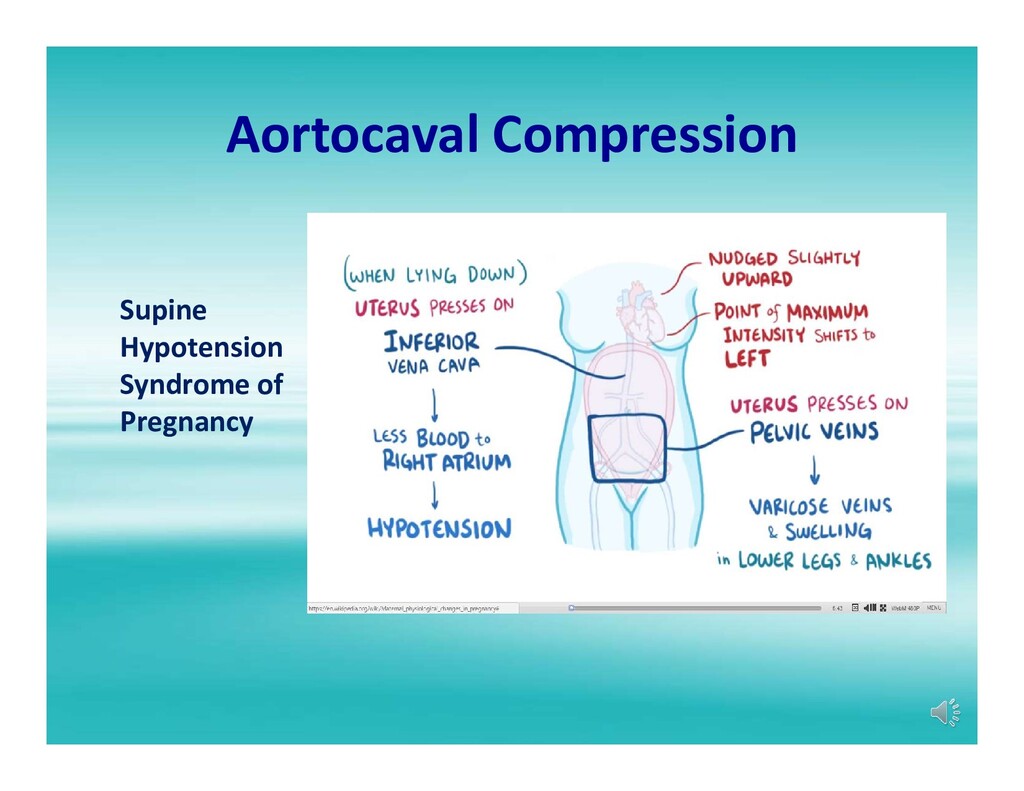
uterus after 16-20 wks EGA • Causes decreased venous return, decreased preload and decreased cardiac output – Compression of the aorta • Increases afterload, can impair uterine blood flow • Symptoms: Maternal hypotension, lightheadedness, dizziness and decreased FHT may be seen • Recommend 15-30 degrees of left uterine displacement
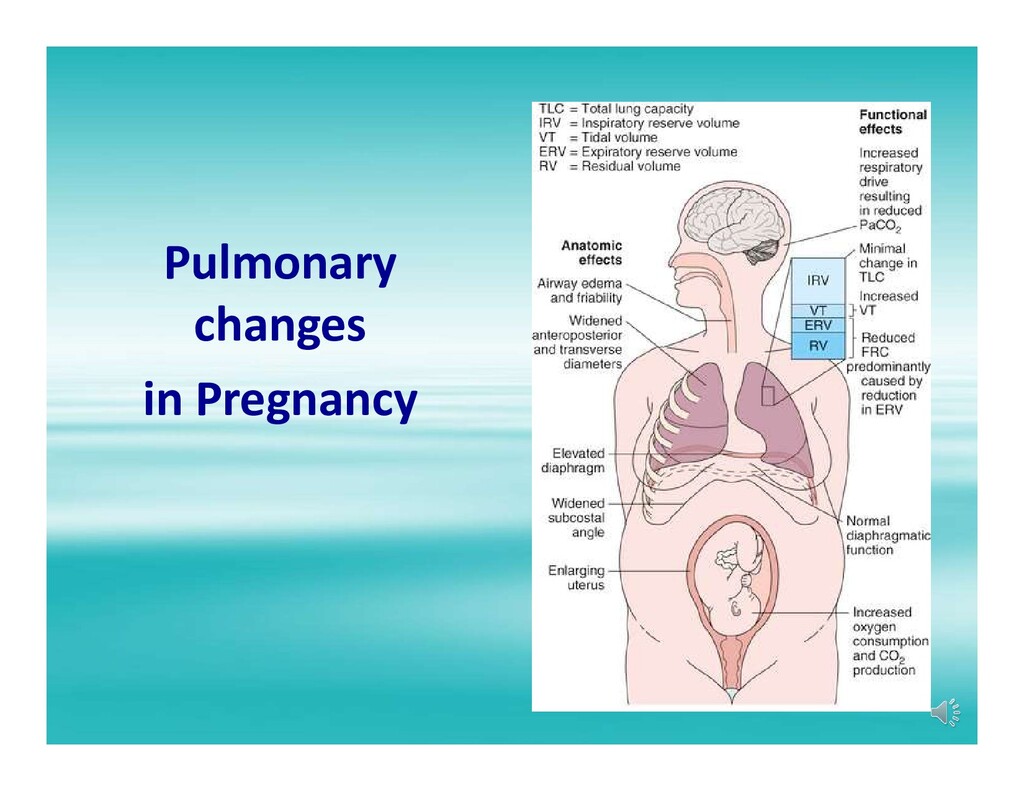
to 45% at term – Due to increased RR and Vt – 1st stage and 2nd labor MV can be as high as 300% • Increased O2 consumption (20-40%) • During labor O2 consumption increases further • 45% increase in the 1st stage • 75% increase in the 2nd stage
stomach position cephalad – Loss of lower esophageal sphincter tone secondary to position change and progesterone levels – Increased intragastric pressure
Pregnancy: no change per se – Labor: once labor starts gastric motility can be significantly delayed • Aspiration Risk – Consider all pregnant patients from 16-20 weeks GA as full stomachs – Therefore they are at increased risk for aspiration – They need aspiration prophylaxis with non-particulate antacids and require RSI
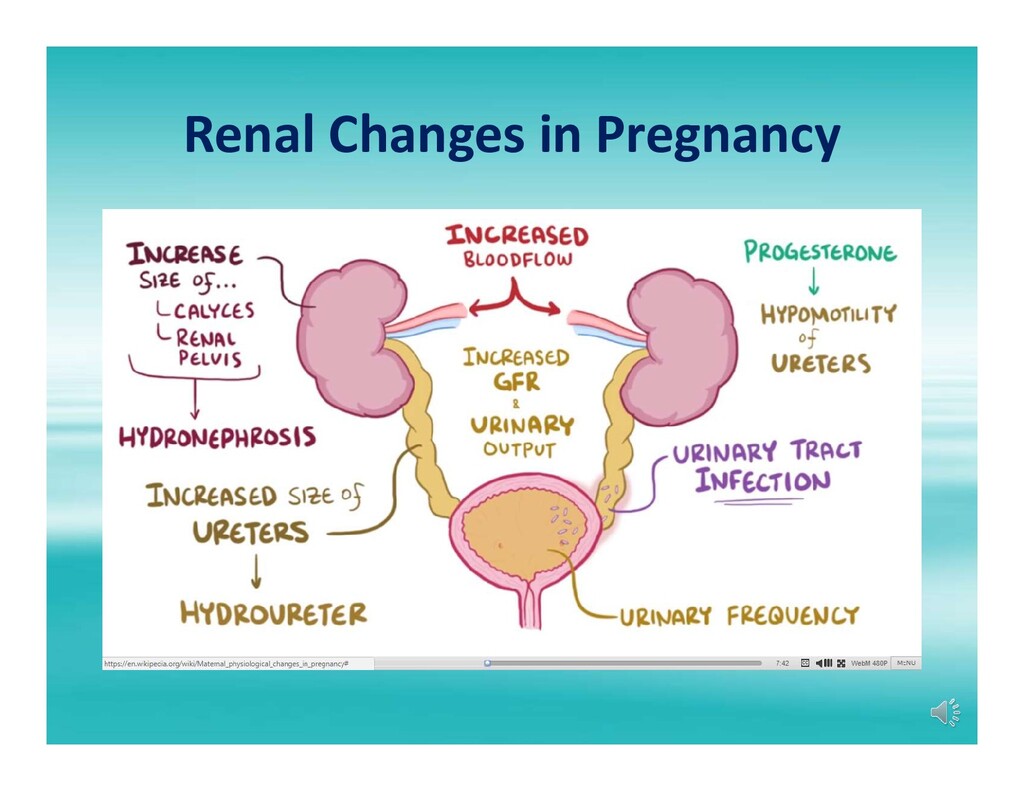
increases • This leads to increased GFR with consequently increased creatinine clearance and decreased serum creatinine • Normal creatinine at term is 0.5 – 0.6 mg/ dL • “Abnormal” creatinine = > 1.0 mg/ dL • Kidneys may enlarge during pregnancy up to 30% • There is increased sodium retention due to increased renin and aldosterone.
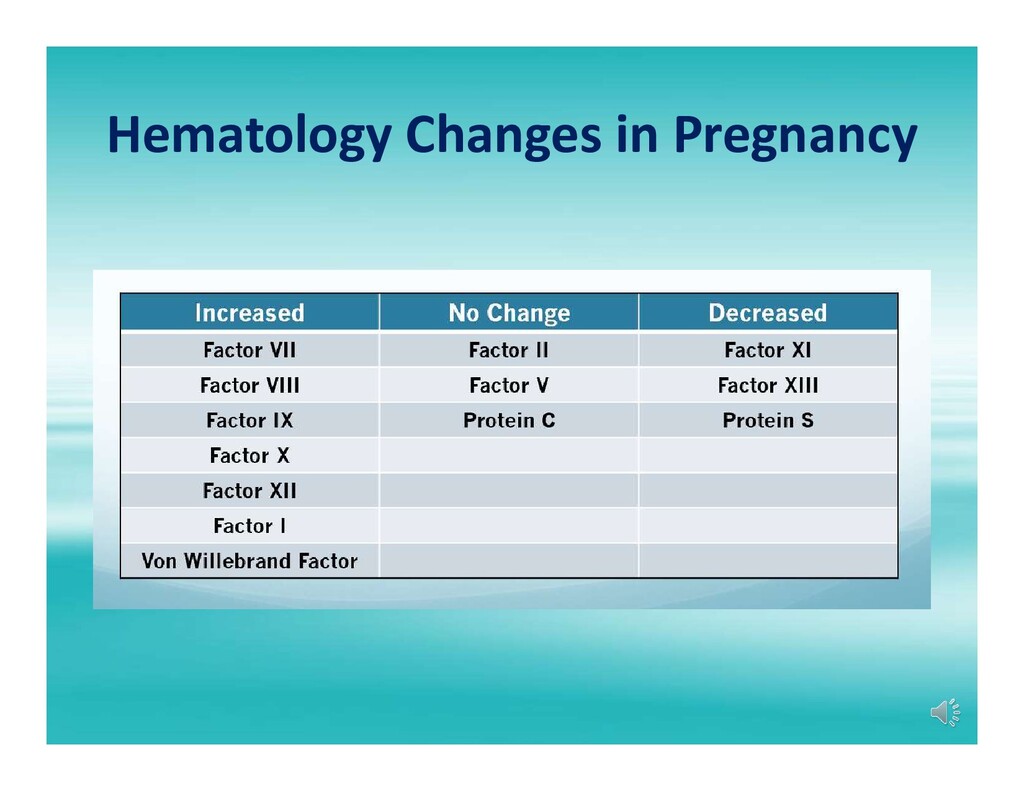
during which the majority of clotting factors increase • Elevated fibrinogen (Normal = 350 – 650 mg/ dL) • During pregnancy there is increased platelet turnover but overall the concentration remains for the most part unchanged. • Laboratory analysis in pregnant patients may reveal a mild decrease in PT/ INR and PTT, but this is not clinically significant.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}