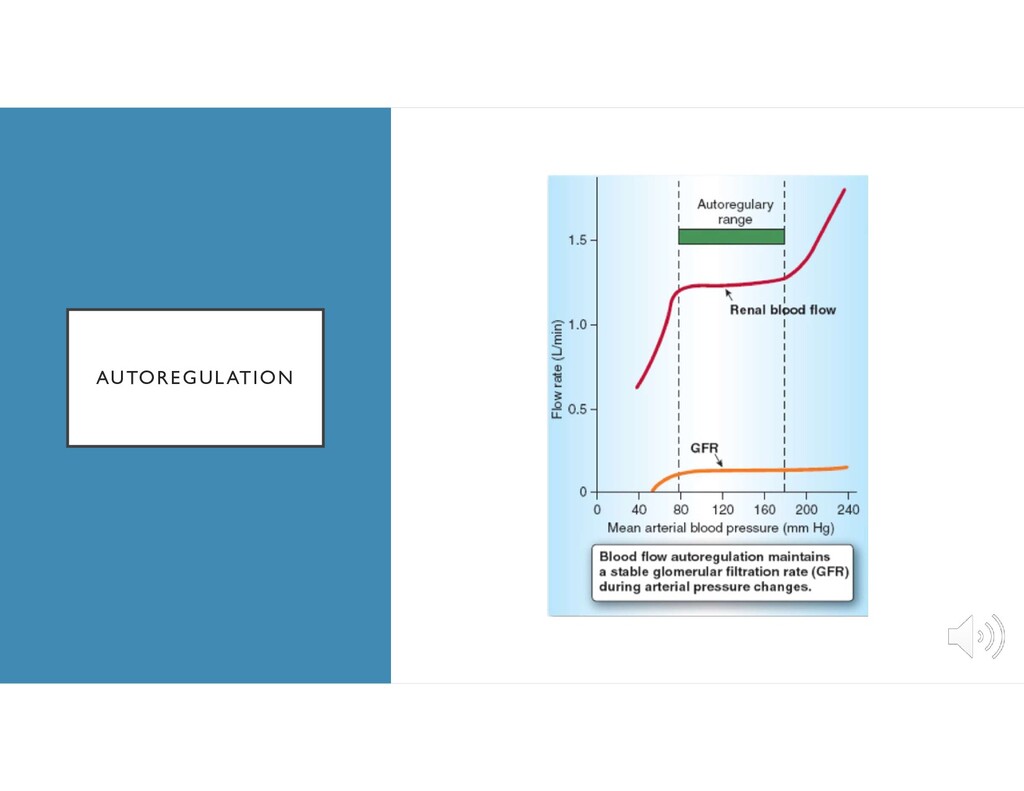
cardiac output • Autoregulation between 80 – 180 mmHg • When MAP is outside autoregulatory range, RBF becomes pressure dependent • Changes in autoregulation with HTN and DM
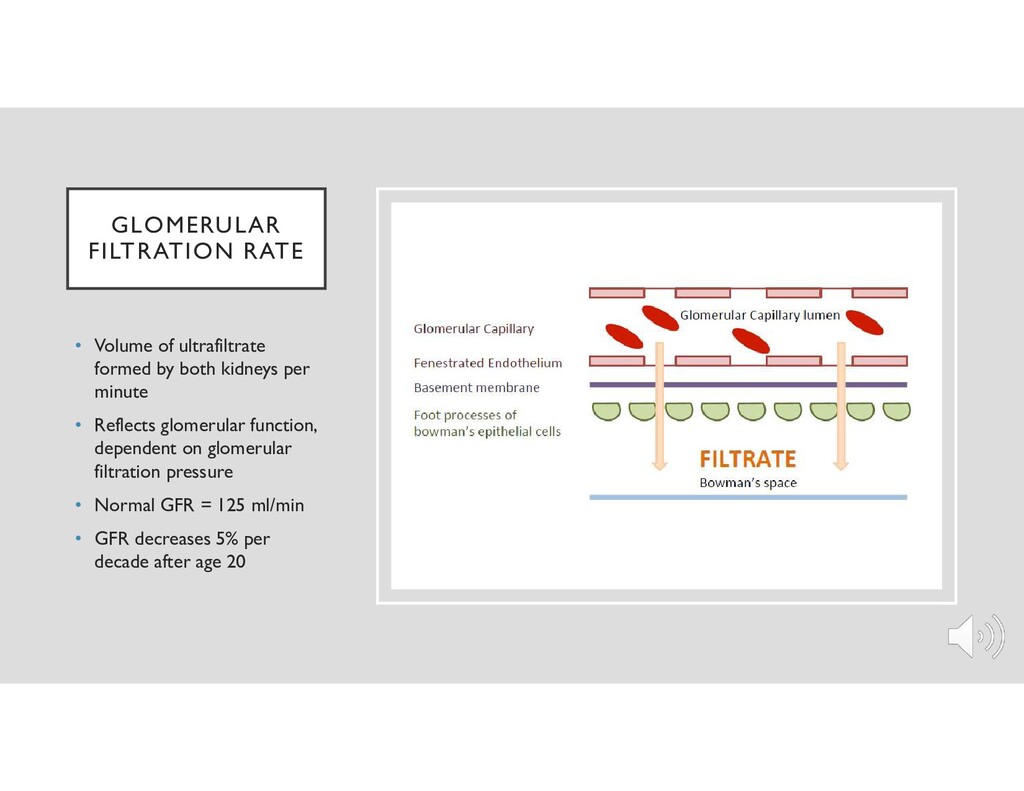
kidneys per minute • Reflects glomerular function, dependent on glomerular filtration pressure • Normal GFR = 125 ml/min • GFR decreases 5% per decade after age 20
normal lab values • Normal values may not be applicable during anesthesia • Tests of glomerular filtration: BUN, Creatinine, Creatinine clearance • Tests of tubular function: Urine specific gravity, Urine osmolality, Urine sodium
marker for GFR • Filtered but not resabsorbed • Muscle metabolism creatine creatinine (nonenzymatically converted) • Not influenced by protein metabolism • Not influenced by fluid flow through renal tubules • Influenced by skeletal muscle mass, age, catabolism • Increases in creatinine not noted until GFR declines 50% • Nonrenal excretion of creatinine via GI tract • Normal serum creatinine = 0.5 – 1.2 mg/dl
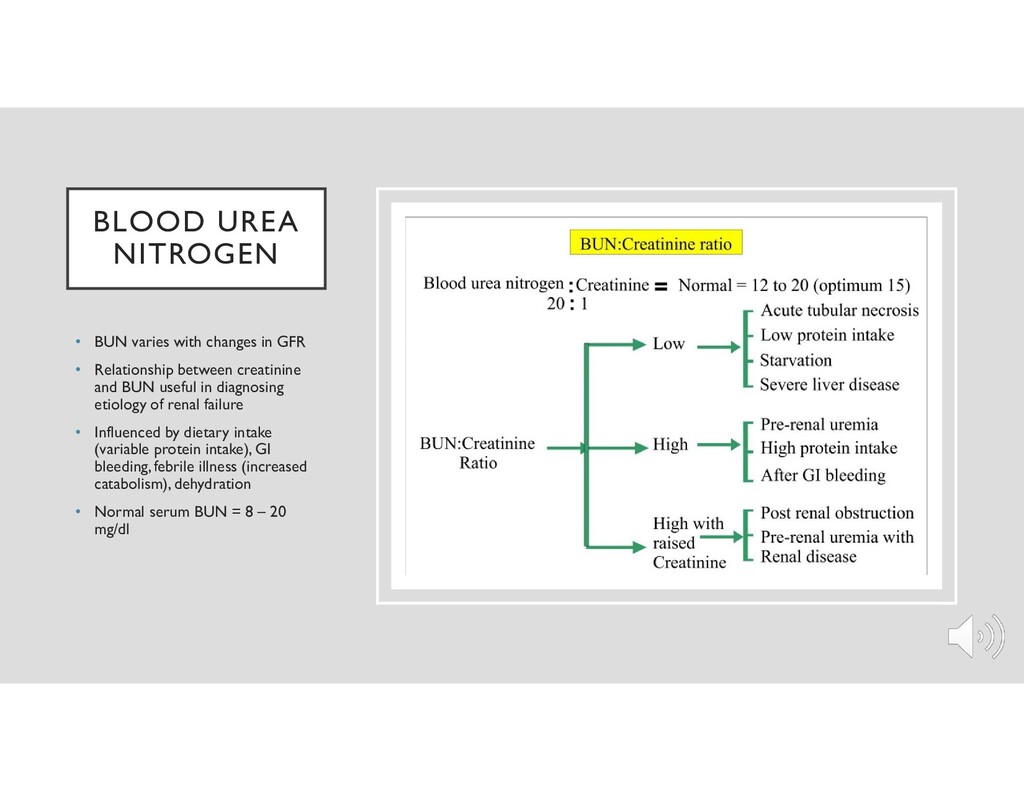
• Relationship between creatinine and BUN useful in diagnosing etiology of renal failure • Influenced by dietary intake (variable protein intake), GI bleeding, febrile illness (increased catabolism), dehydration • Normal serum BUN = 8 – 20 mg/dl
into urine for a given serum creatinine concentration • Most reliable measure of GFR (than serum BUN and creatinine) • Does not depend on age or presence of steady state • Timed test, accurate urine volume measurement influences interpretation • GFR = CrCl = (Urine creatinine x Urine flow rate)/(Serum creatinine) • Progressive renal disease enhances creatinine secretion in proximal tubules (CCR progressively overestimates true GFR)
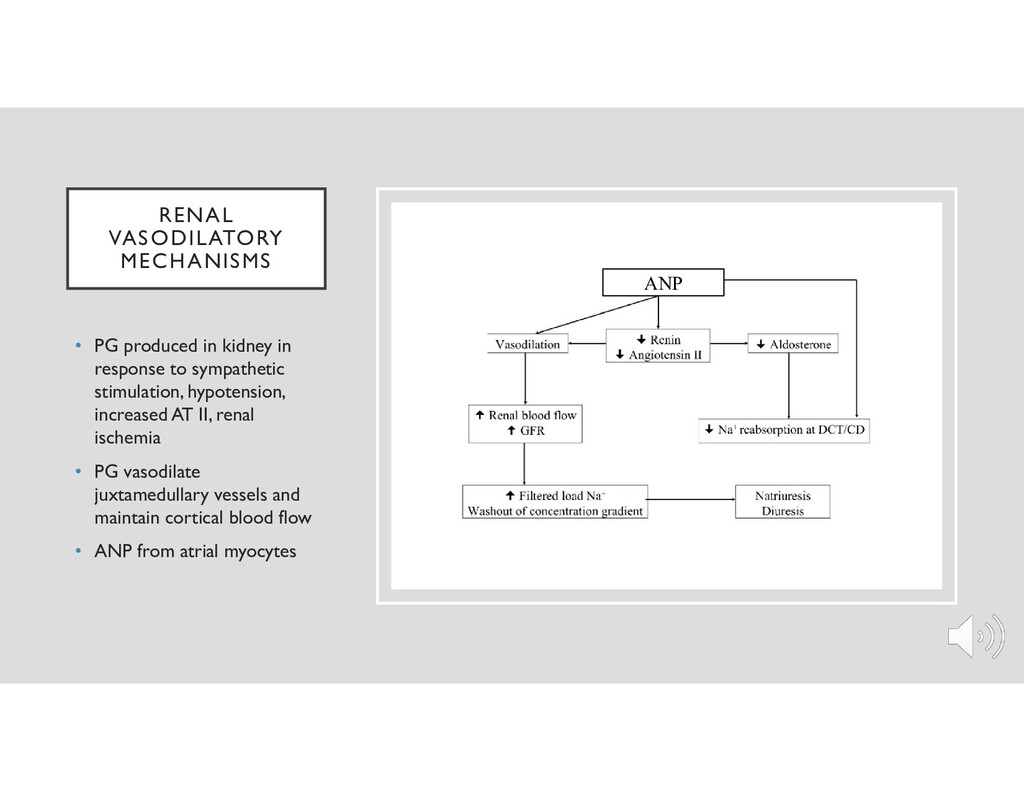
to sympathetic stimulation, hypotension, increased AT II, renal ischemia • PG vasodilate juxtamedullary vessels and maintain cortical blood flow • ANP from atrial myocytes ANP
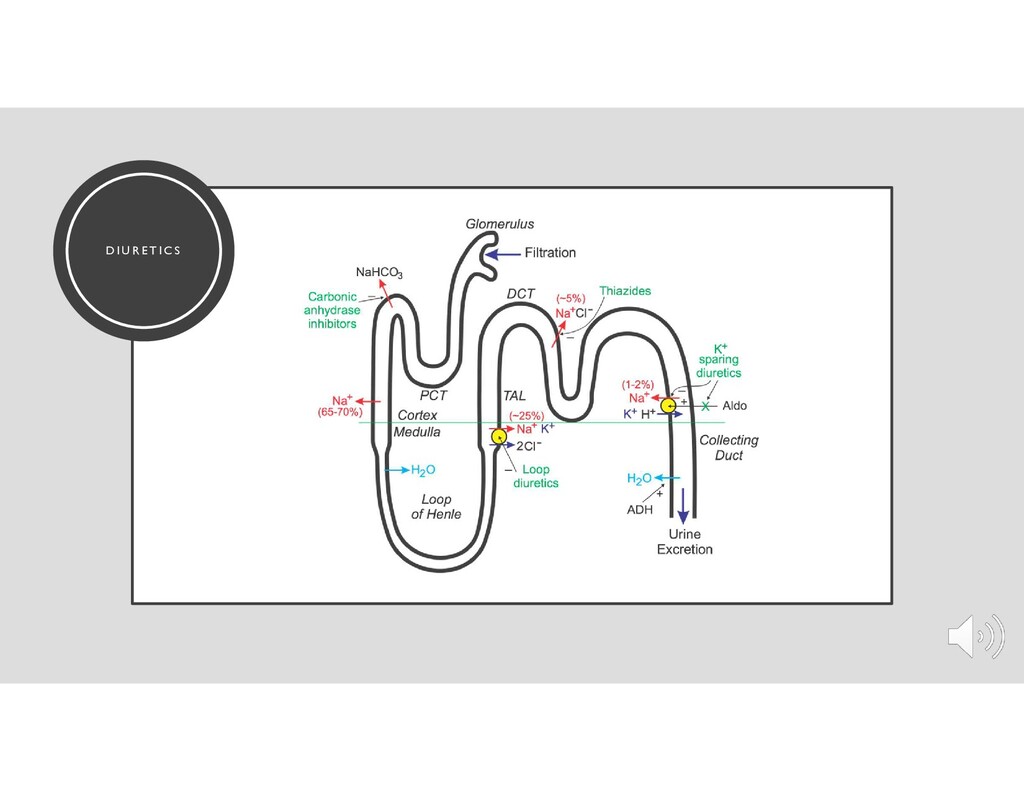
• This is accomplished by altering how the kidney handles sodium • Many have more than one mechanism of action • Majority of diuretics exert their action on the luminal cell membrane from within the renal tubules • Highly protein bound
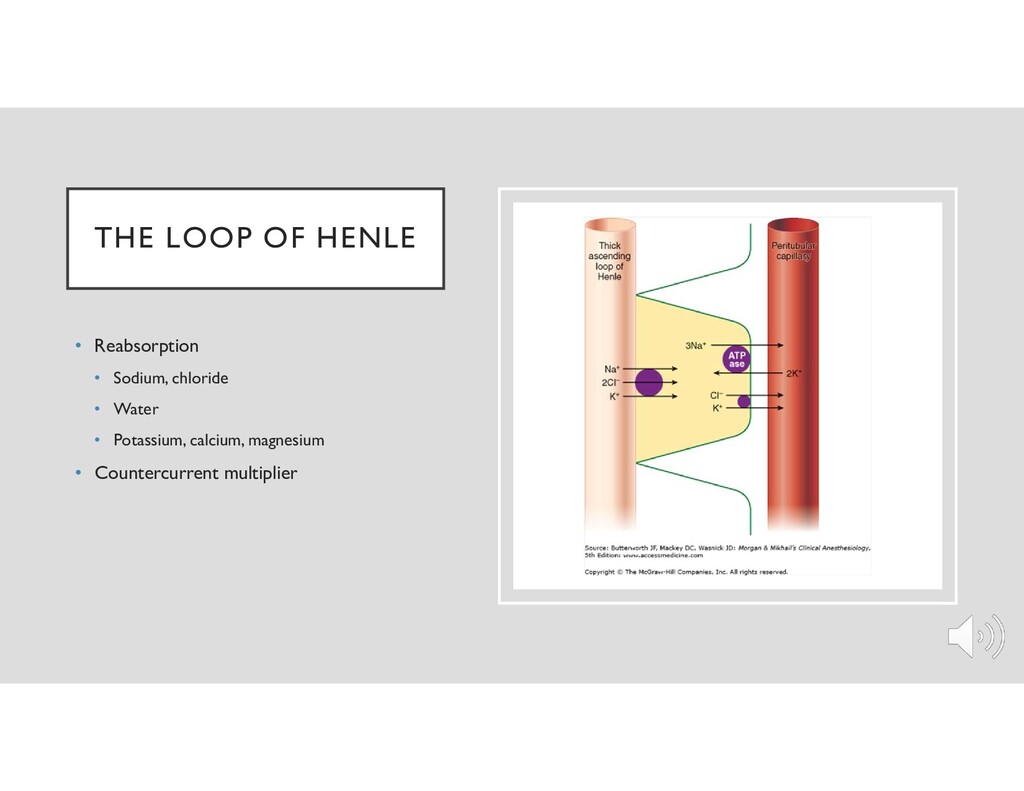
• Inhibit the sodium-potassium-chloride cotransporter in the thick ascending limb • With max effect, promote excretion of 15-20% of filtered sodium load • Induce renal synthesis of prostaglandins • Increase urinary calcium and magnesium excretion (treatment of hypercalcemia)
in the distal tubule • Increase Na+ excretion to only 3-5% of the filtered load • Carbonic anhydrase inhibiting action in proximal tubule • Augment calcium reabsorption in the distal tubule
Noncompetitive potassium-sparing diuretics (Triamterene and amiloride) – not dependent on aldosterone activity • Adjuvants, usually used in conjunction with other diuretics • Inhibit Na+ reabsorption in collecting tubules
not reabsorbed • Increased osmolarity of renal tubule fluid and associated excretion of water • Increased RBF, PG synthesis, free radical scavenger • Reduction of ICP and cerebral edema • Role in AKI
arterioles via its agonistic action at the DA1 receptor, leading to increased RBF and GFR • Dopamine dose dependent side effects: tachydysrhythmias, pulmonary shunting, tissue ischemia • Fenoldopam is a selective DA1 receptor agonist, lacks adrenergic activity • Low dose dopamine (0.5-3 mcg/kg/m) is natriuretic • “Renal dose dopamine” – no significant renoprotective properties
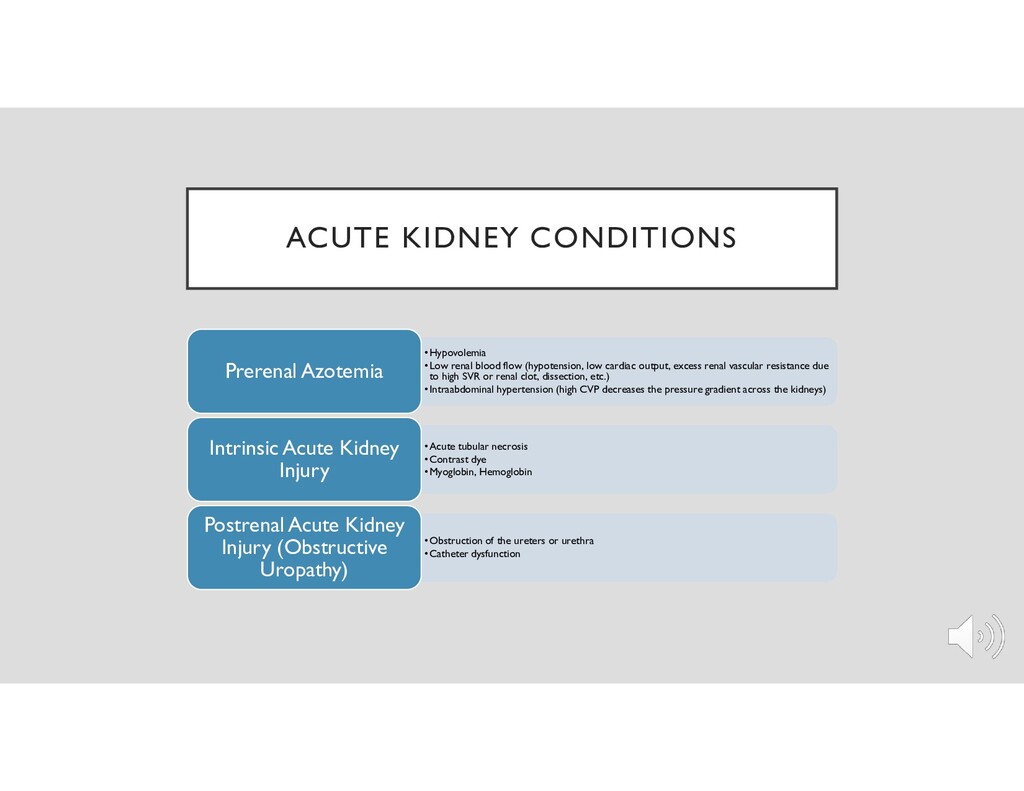
amounts of sodium • Tubular function intact • Management is influenced by their risk for development of ARF • Fluid challenge may help • Administration of diuretics is controversial
large amounts of fluid can be removed and electrolyte abnormalities can rapidly be corrected •Not appropriate in unstable patients, as 20-30% of patients undergoing hemodialysis will become hypotensive •In an unstable patient, the hypotension may not be tolerated and could cause further renal injury or disequilibrium syndrome from the large osmotic shifts Peritoneal dialysis •Simple and cost effective •Can cause infection, has poor clearance of solutes and uric acid Continuous hemodiafiltration •More effective urea clearance and controlled fluid removal •Beneficial in the critically ill patient, as these patients usually have intravascular hypovolemia secondary to decreased oncotic pressure from capillary leak, and this method allows for precise volume control, continuously. •Provides improved nutritional support •Safer in patients with cerebral injury or cardiovascular disorders, given the improved control of volume
decreases in RBF, GFR, urinary flow, sodium excretion occur during both general and regional anesthesia • Increases in epinephrine, norepinephrine, renin, ATII, aldosterone, ADH, cortisol common as a stress response • Volatile and intravenous drug effects… • Pneumoperitoneum produces abdominal compartment-like state
kidneys for elimination, ability to control BP, minimal direct effects on RBF • Decrease renal vascular resistance • Accelerated induction and emergence may be seen in severely anemic patients • Compound A, breakdown product of Sevoflurane, accumulation in breathing circuit is favored by low flow rates (<2L/min) • Nitrous oxide decreases arterial oxygen content, may be avoided in severely anemic patients
morphine-6- glucuronide and normeperidine, respectively, can prolong respiratory depression (with chronic administration). Increased normeperidine lowers seizure threshold • Hydromorphone metabolite hydromorphone-3-glucuronide may accumulate causing cognitive dysfunction and myoclonus • Codeine & sufentanil can cause prolonged narcosis • Fentanyl – no active metabolites, unchanged free fraction, short redistribution phase • Alfentanil – reduced protein binding, no change in elimination half life or clearance, inactive metabolites • Remifentanil metabolite clinical implications are limited
effects in ESRD because of their dependence on renal excretion • Succinylcholine, atracurium, cis-atracurium, and mivacurium appear to have minimal renal excretion of the unchanged parent compound • Most nondepolarizing muscle relaxants must be either hepatically excreted or metabolized to inactive forms in order to terminate their activity • Some muscle relaxants have renally excreted active metabolites that may contribute to their prolonged duration of action in patients with ESRD
elevated, its use can be justified as part of a rapid-sequence anesthesia induction technique because its duration of action in ESRD is not significantly prolonged • The rise in serum potassium following succinylcholine administration is 0.5 mEq/L in normal • Potassium rise following succinylcholine administration is usually well tolerated in patients with chronically elevated serum potassium levels • Although decreased plasma cholinesterase levels have been reported in uremic patients following dialysis, significantly prolonged neuromuscular block is rare
enzymatic ester hydrolysis and spontaneous nonenzymatic (Hoffman) degradation with minimal renal excretion of the parent compound • Their elimination half-life, clearance, and duration of action are not affected by renal failure • Atracurium metabolite, laudanosine, may accumulate with repeated dosing or continuous infusion (Seizures in animals)
as a result of reduced plasma clearance and increased elimination half-life • An intubating dose lasts approximately 50% longer in patients with ESRD • Active metabolite, 3-desmethylvecuronium, accumulates in patients receiving a continuous vecuronium infusion • Rocuronium has a pharmacokinetic profile in normal subjects similar to that of vecuronium, but block is variable • With appropriate neuromuscular block monitoring, both drugs can be used safely in patients in renal disease
route of elimination for edrophonium, neostigmine, and pyridostigmine • Half-lives are prolonged at least as much as any of the relaxants • The anticholinergic agents atropine and glycopyrrolate are similarly excreted by the kidney • No dosage alteration of anticholinesterases are required • “Recurarization” is unlikely
mild to moderate renal impairment • Bridion not recommended for use in patients with severe renal impairment (CC<30mL/min), including those requiring dialysis • Persistent sugammadex may impair the ability of some paralytics to work if re- paralysis is needed
(balance with need to preserve arteries) • Risk of thrombosis if blood pressure cuff on the same arm with AV fistula • Consider RSI • Dose of induction agent reduced if immediately following dialysis • Maintenance agent should control HTN with minimal deleterious effect on CO • Controlled ventilation should be considered with kidney failure • Consider avoiding LR if large volumes required (4 mEq/L potassium)
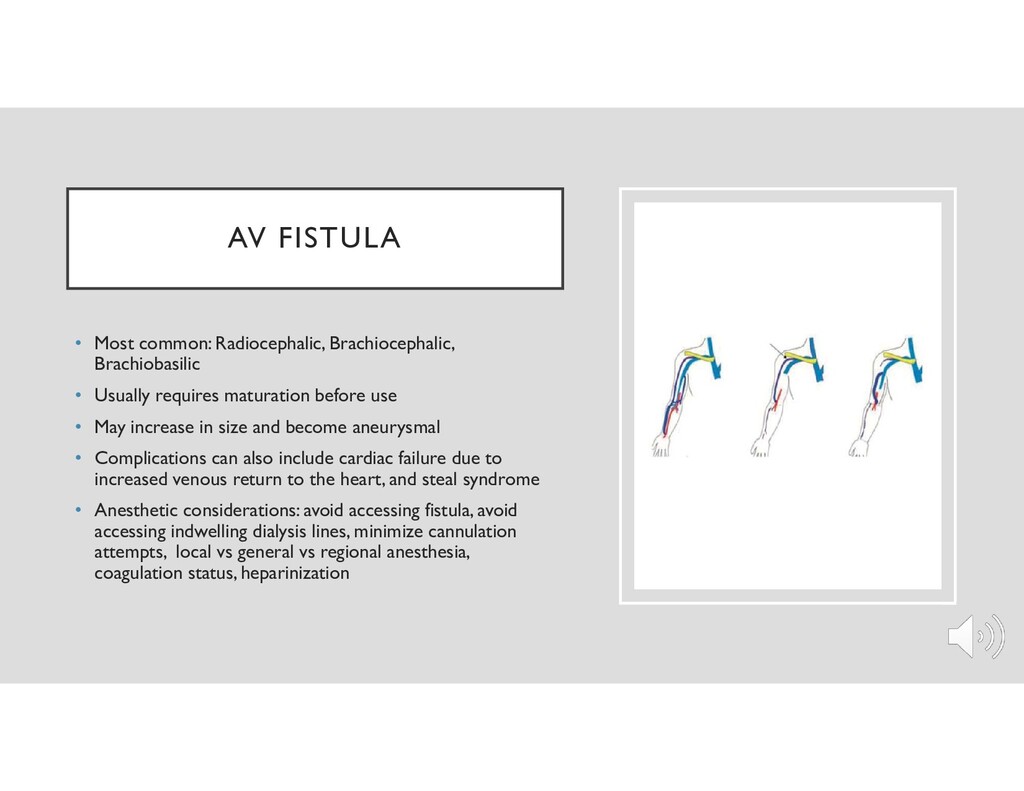
requires maturation before use • May increase in size and become aneurysmal • Complications can also include cardiac failure due to increased venous return to the heart, and steal syndrome • Anesthetic considerations: avoid accessing fistula, avoid accessing indwelling dialysis lines, minimize cannulation attempts, local vs general vs regional anesthesia, coagulation status, heparinization
graft to connect artery and vein, tunneled subcutaneously • Ease of cannulation, large surface area, short maturation time • Greater thrombosis and infection rates, and inferior long-term patency
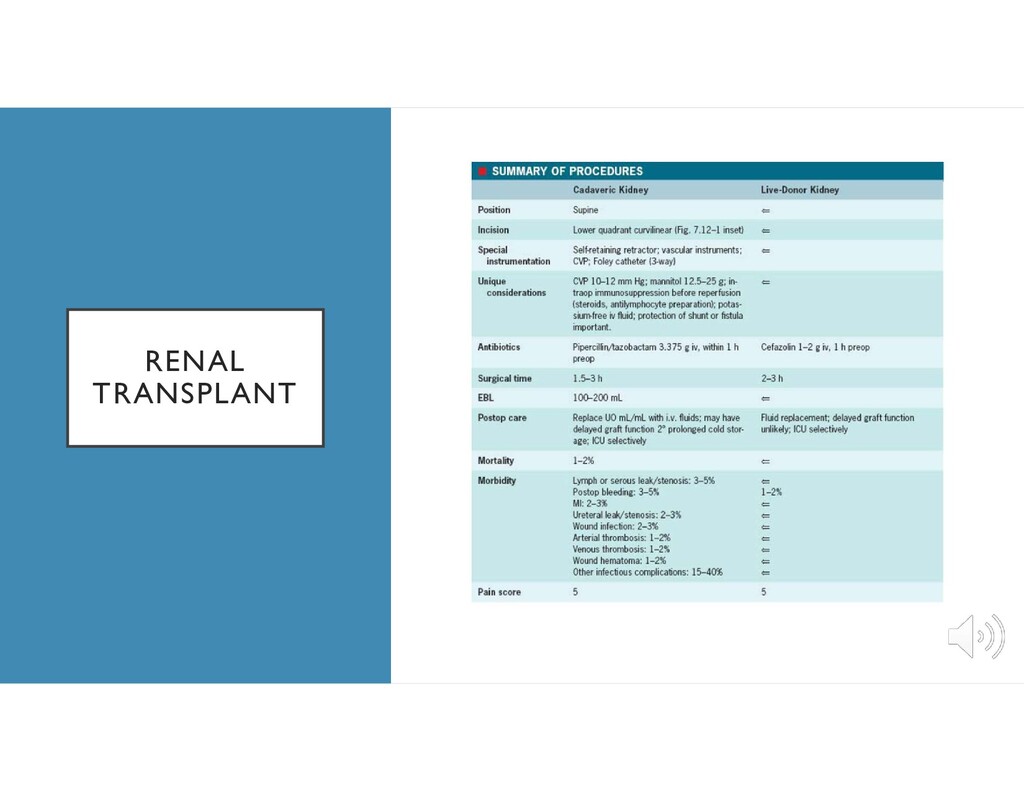
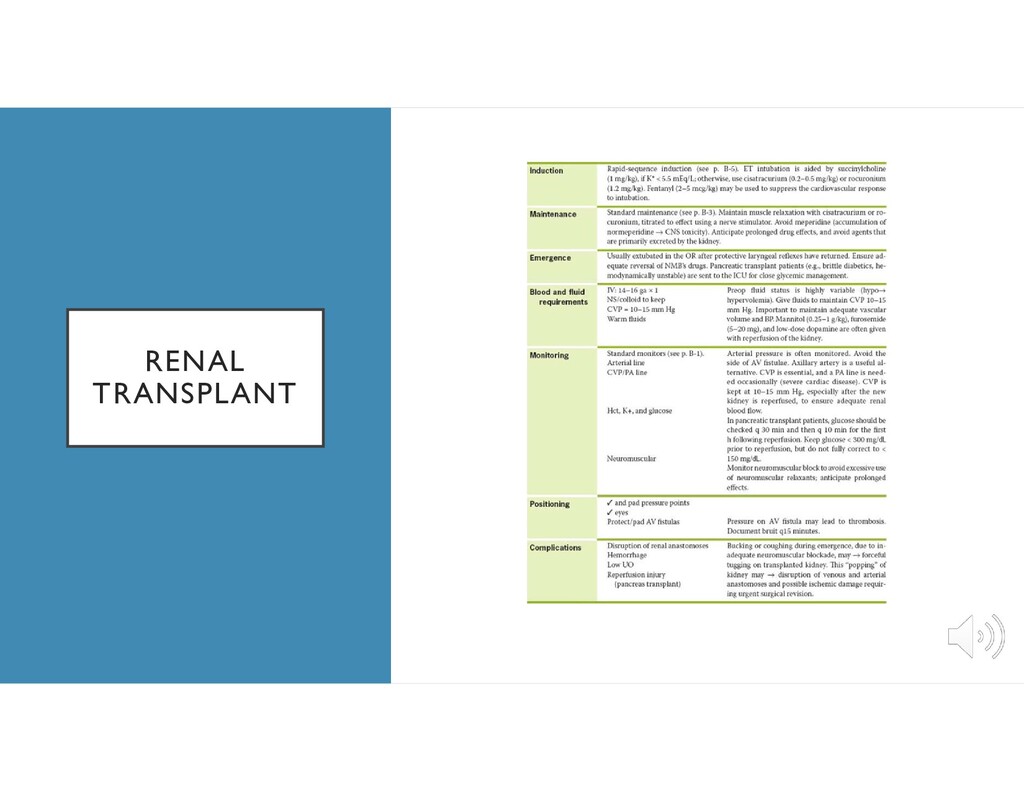
transplant list: T2DM and HTN • Cardiovascular disease is the leading cause of death (and therefore graft loss) after renal transplantation • Screening for tumors and infection, psychiatric stability, social support • Severe heart, lung, or liver disease; most malignancies are exclusions • Patients should be dialyzed before surgery • Scheduling of transplant and maximal cold ischemia time dependent on type of donor (ie. SCD, ECD, DCD)
• Ability to increase renal blood flow • Release of intrarenal vasodilating prostaglandins and atrial natriuretic peptide (ANP) • Oxygen free-radical scavenger • May convert a patient from oliguric ARF to nonoliguric ARF • Significant reduction in postoperative acute tubular necrosis in patients treated with mannitol • Adequate volume expansion with crystalloid prior to vessel clamp also helps decrease postoperative ATN
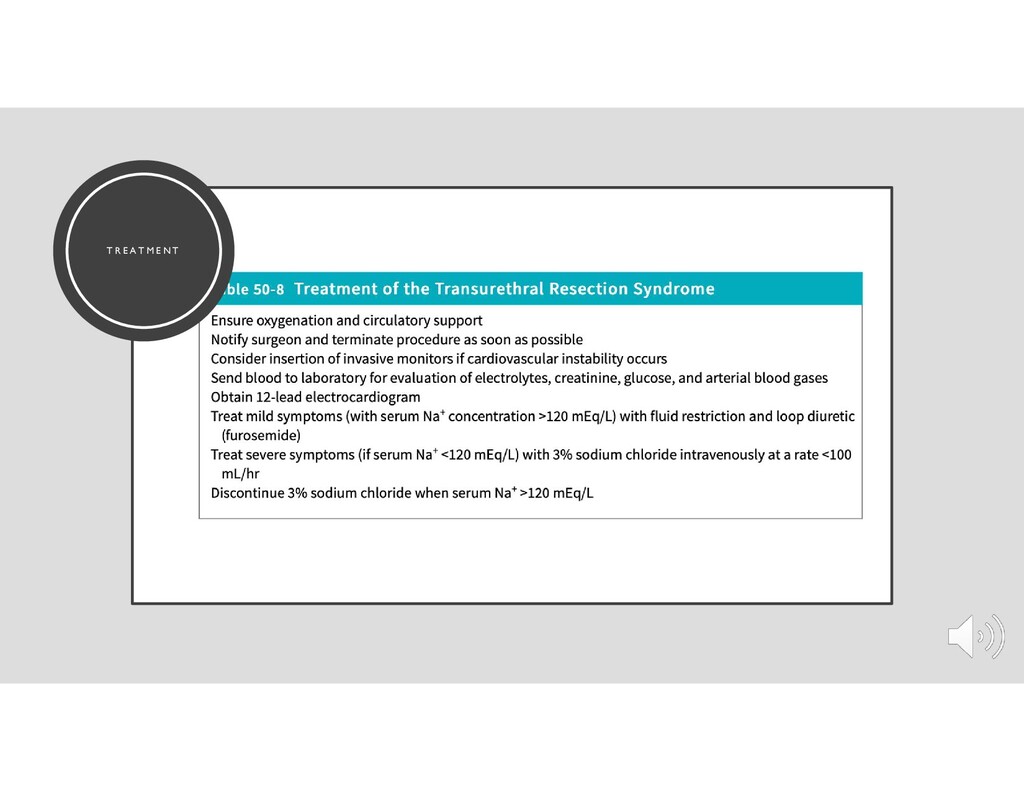
• Nonconductive nonelectrolyte solutions • Hypervolemic water intoxication • The principal components are • (1) excessive volume expansion (respiratory distress, congestive heart failure, pulmonary edema, hypertension, bradycardia, etc.) • (2) hyponatremia (mental confusion, nausea, etc.) • (3) other problems specific to each of the irrigating solutions
• Increased irrigant absorption dependent on • number and size of open venous sinuses • surgical disruption of the prostatic capsule • longer duration of resection (limit to 1 hour) • higher hydrostatic pressure of the irrigating fluid (limit suspension no more than 30cm) • lower venous pressure at the irrigant–blood interface
than 125 mmol/L • Hyponatremia may occur in the setting of an expanded, normal, or contracted extracellular fluid volume • Intravascular volume status and urinary sodium concentration are key in differentiating • If water excess is a reason for hyponatremia, a dilute urine with a sodium concentration above 20 mmol/L is expected • Renal sodium retention (urine sodium <20 mmol/L) suggests sodium loss as a cause • If hyponatremia is acute, the risk of neurologic complications is higher, and cautious treatment is indicated to prevent cerebral edema and seizures • This should be accomplished with intravenous hypertonic saline and furosemide to enhance water excretion and prevent sodium overload
commonly the latter • Dehydration of brain tissue can cause symptoms ranging from confusion to convulsions and coma • Hemoconcentration, hyperosmolar low urine output, very low urinary sodium concentration and evidence of prerenal failure (elevations of BUN and serum creatinine) • Occasionally, the urine is not maximally concentrated, suggesting an osmotic diuresis or an intrinsic renal disorder such as diabetes insipidus • The primary goal of treatment is restoration of serum tonicity, which can be achieved with isotonic or hypotonic parenteral fluids and/or diuretics
to the intracellular space • Total body depletion may exist even with normal extracellular potassium levels (e.g., diabetic ketoacidosis) • Causes of hypokalemia include extrarenal loss (e.g., vomiting, diarrhea), renal loss (impaired processing due to drugs, hormones, or inherited renal abnormalities), potassium shifts between the extra- and intracellular spaces (e.g., insulin therapy) • Clinical manifestations of hypokalemia include electrocardiography (ECG) changes (flattened T waves—“no pot, no T,” U waves, prodysrhythmic state) and skeletal muscle weakness • Hypokalemia treatment involves supplementation by either intravenous or oral route
• Causes of acute hyperkalemia: drugs (succinylcholine, ACE/ARB’s, mannitol, spironolactone, digitalis, non-selective beta blockers) that cause decreased renal K+ excretion, reperfusion of an organ/vascular bed after ischemia (usually greater than 4 hours), transfusions, decreased aldosterone levels, transcellular shifts (intracellular to extracellular), often caused by acidosis, acute renal failure • ECG changes (peaked T waves, ST segment depression, and shortened QT interval), soon followed by manifestations of severe hyperkalemia, including QRS complex widening, prolonged PR interval, disappearance of the P wave, sine wave QRS, ventricular fibrillation, and asystole • Clinically, muscle weakness and paralysis
seizures, and respiratory arrest • Mental status changes, including irritability, depression, and impaired cognition may also occur • Cardiac manifestations include QT interval prolongation and dysrhythmias, possible complete heart block • May be due to several mechanisms, including a decrease in PTH secretion or action, reduced vitamin D synthesis or action, resistance of bone to PTH or vitamin D effects, or calcium sequestration • Acute hypocalcemia due to citrate toxicity can develop from rapid infusion of citrate-stored packed red blood cells, particularly with citrate accumulation during the anhepatic phase of liver transplant procedures • Parathyroidectomy, either selectively or as a complication of thyroidectomy during neck surgery, can acutely reduce PTH levels and precipitate hypocalcemia
mL) often has no symptoms, but when levels > 15 mg/100 mL, clinical changes become more common • Clinical symptoms include constipation, nausea and vomiting, polyuria, renal calculi, oliguric renal failure, drowsiness, lethargy, weakness, stupor, and coma • Cardiovascular manifestations may include shortened QT interval, QRS widening • The most frequent causes of hypercalcemia are primary hyperparathyroidism and malignancy • Other causes include thiazide or lithium therapy, granulomatous disease, renal failure
to dilute plasma calcium • Patients who have muscle weakness should receive decreased doses of nondepolarizing muscle relaxants • Vigilance with respect to EKG
excessive intake (magnesium- containing antacids or laxatives) and/or renal impairment • Iatrogenic hypermagnesemia can also occur during magnesium sulfate therapy for gestational hypertension in the mother as well as the fetus • Clinical manifestations typically are hyporeflexia, sedation, nausea, vomiting, flushing, urinary retention, ileus and skeletal muscle weakness • Impaired release of acetylcholine and decreased motor end-plate sensitivity to acetylcholine • Vasodilation, bradycardia, myocardial depression, respiratory arrest • Prolongation of the P–R interval and widening of the QRS complex
should be stopped • Intravenous calcium • Loop diuretic along with an infusion of ½-normal saline in 5% dextrose enhances urinary magnesium excretion • Dosages of NMBAs should be reduced by 25–50%
it forms ATP in all cells • Symptoms include muscle weakness, respiratory failure, and difficulty in weaning critically ill patients from mechanical ventilation • Leftward shift of the oxyhemoglobin curve (increased affinity for oxygen: less oxygen delivery to tissues), increased RBC fragility • Hypophosphatemia can result from intracellular redistribution, inadequate intake or absorption secondary to alcoholism or malnutrition, or from increased renal or gastrointestinal losses • Treatment with intravenous and oral supplementation
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}