lesions 2. To articulate the anesthetic management of patients with neurological hematomata 3. To assess the measures of controlling intracranial pressure intraoperatively
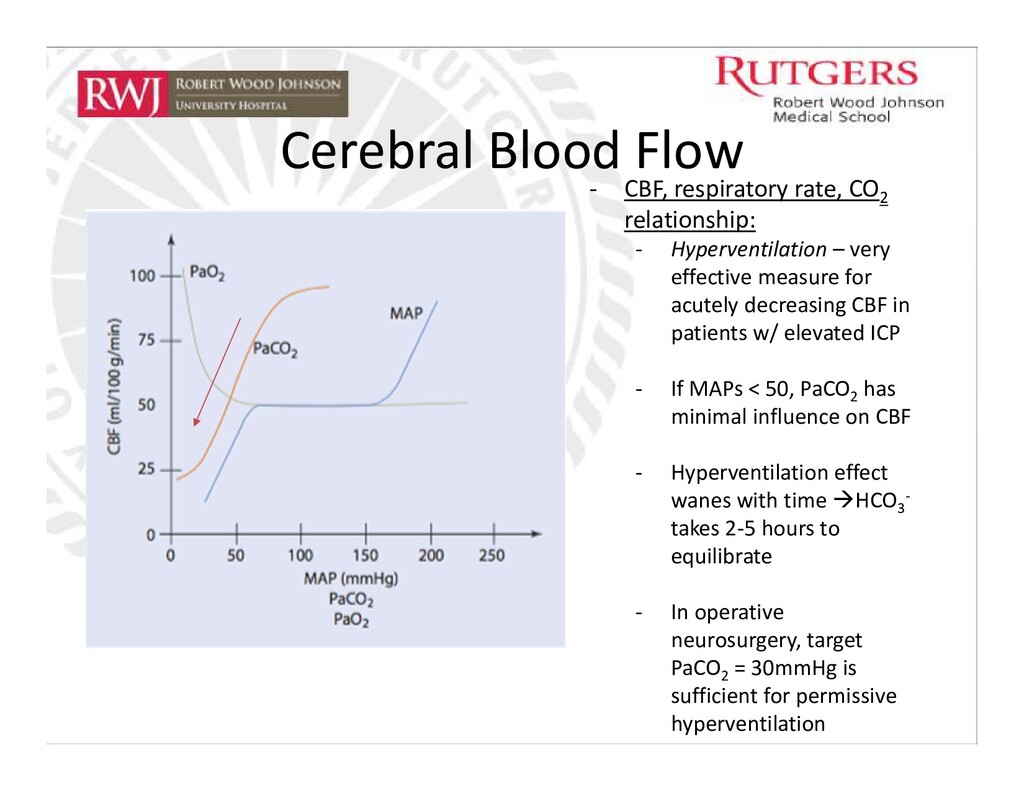
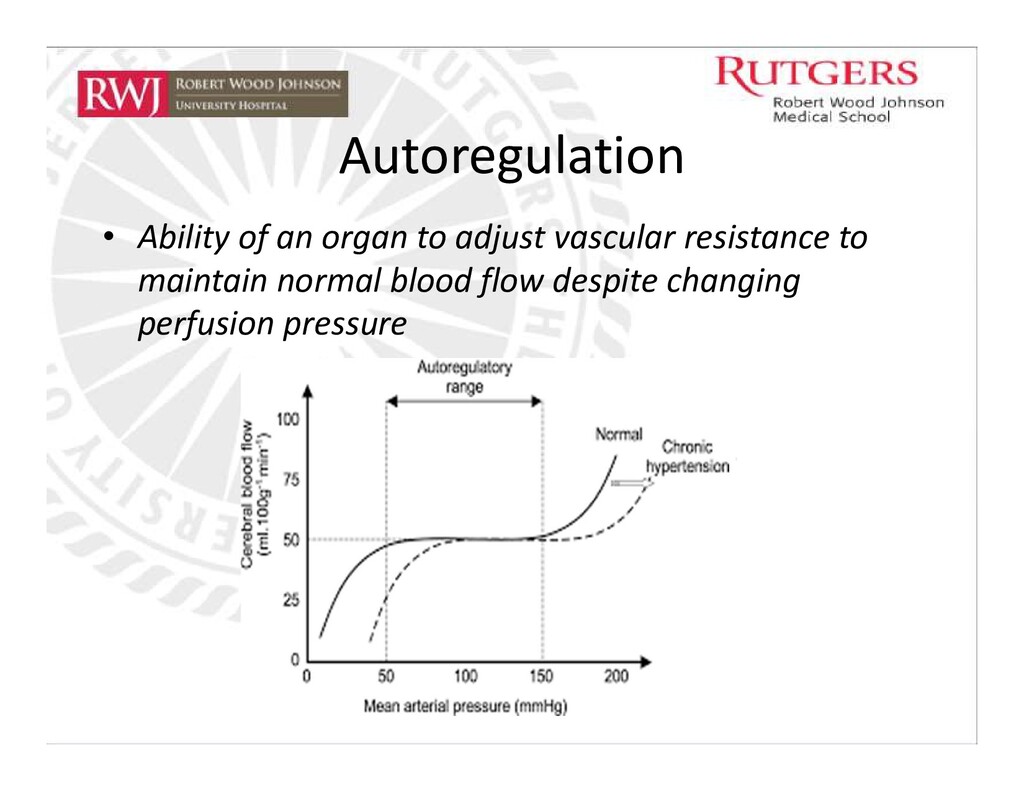
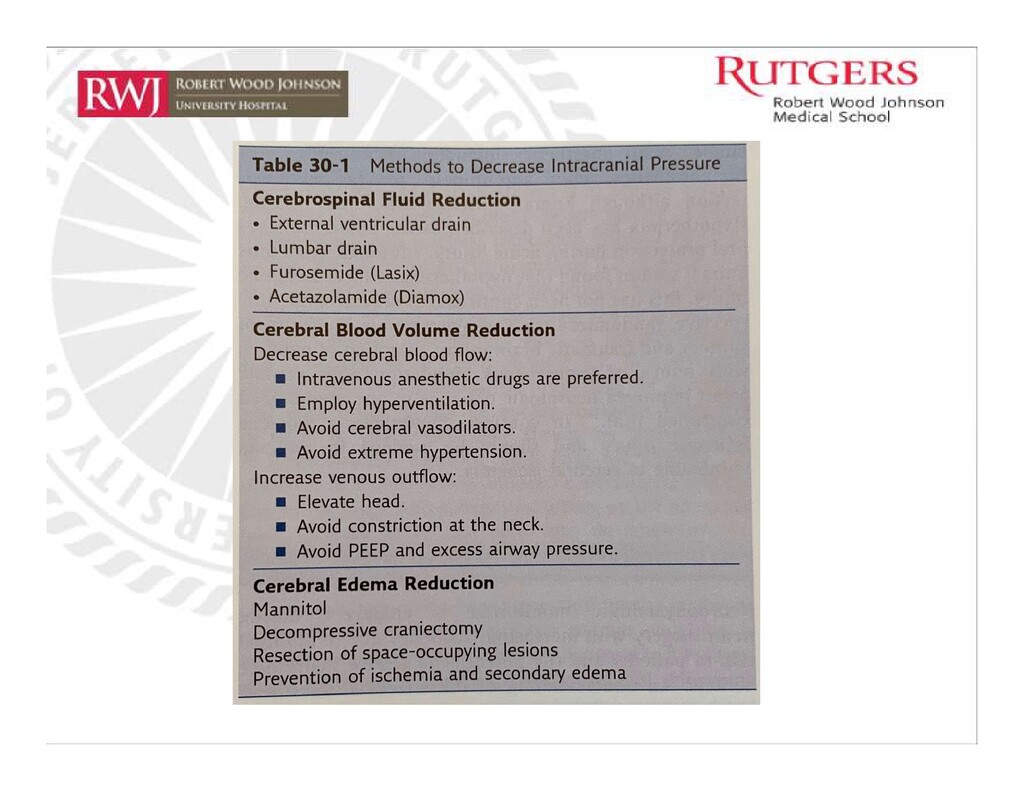
Hyperventilation – very effective measure for acutely decreasing CBF in patients w/ elevated ICP - If MAPs < 50, PaCO2 has minimal influence on CBF - Hyperventilation effect wanes with time HCO3 - takes 2-5 hours to equilibrate - In operative neurosurgery, target PaCO2 = 30mmHg is sufficient for permissive hyperventilation
/100g tissue/min • What Increases CMRO2 ? 1. Elevated regional brain activity 2. Seizures 3. Hyperthermia 4. IV anesthetics such as ketamine • What Decreases CMRO2 ? 1. Hypothermia 2. Inhalational anesthetics 3. Deep sleep 4. Comatose states for every 1°C decrease in temperature, CMR decreases, ultimately decreasing CBF by 7%
on decreasing ICP? a) Increasing respiratory rate from 10 bpm to 14 bpm b) Decreasing PEEP from 8 - 3 c) Administering 20% Mannitol IV d) Elevating head of the bed e) Opening External Ventricular Drain
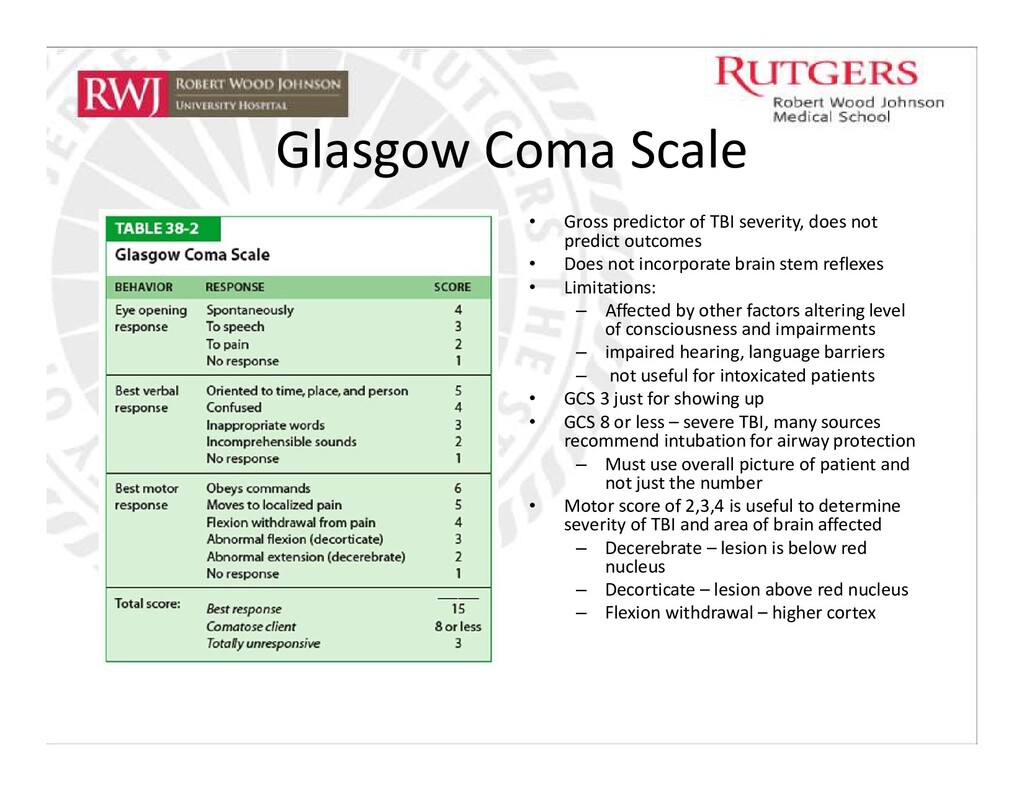
not predict outcomes • Does not incorporate brain stem reflexes • Limitations: – Affected by other factors altering level of consciousness and impairments – impaired hearing, language barriers – not useful for intoxicated patients • GCS 3 just for showing up • GCS 8 or less – severe TBI, many sources recommend intubation for airway protection – Must use overall picture of patient and not just the number • Motor score of 2,3,4 is useful to determine severity of TBI and area of brain affected – Decerebrate – lesion is below red nucleus – Decorticate – lesion above red nucleus – Flexion withdrawal – higher cortex
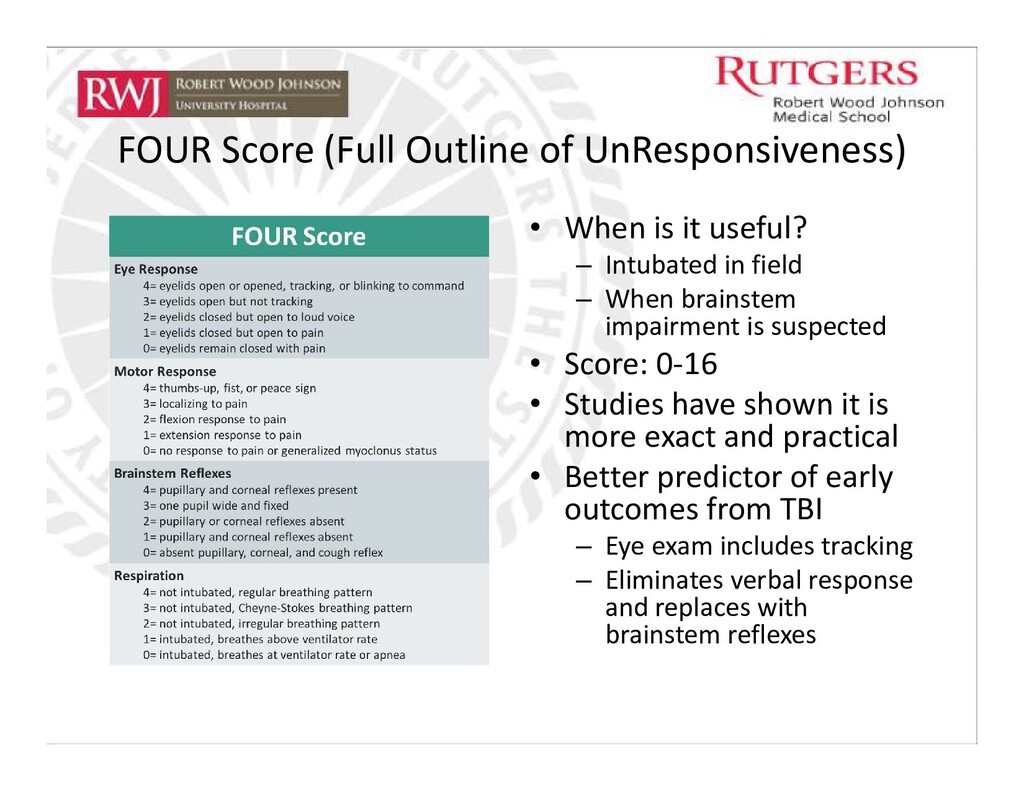
useful? – Intubated in field – When brainstem impairment is suspected • Score: 0-16 • Studies have shown it is more exact and practical • Better predictor of early outcomes from TBI – Eye exam includes tracking – Eliminates verbal response and replaces with brainstem reflexes
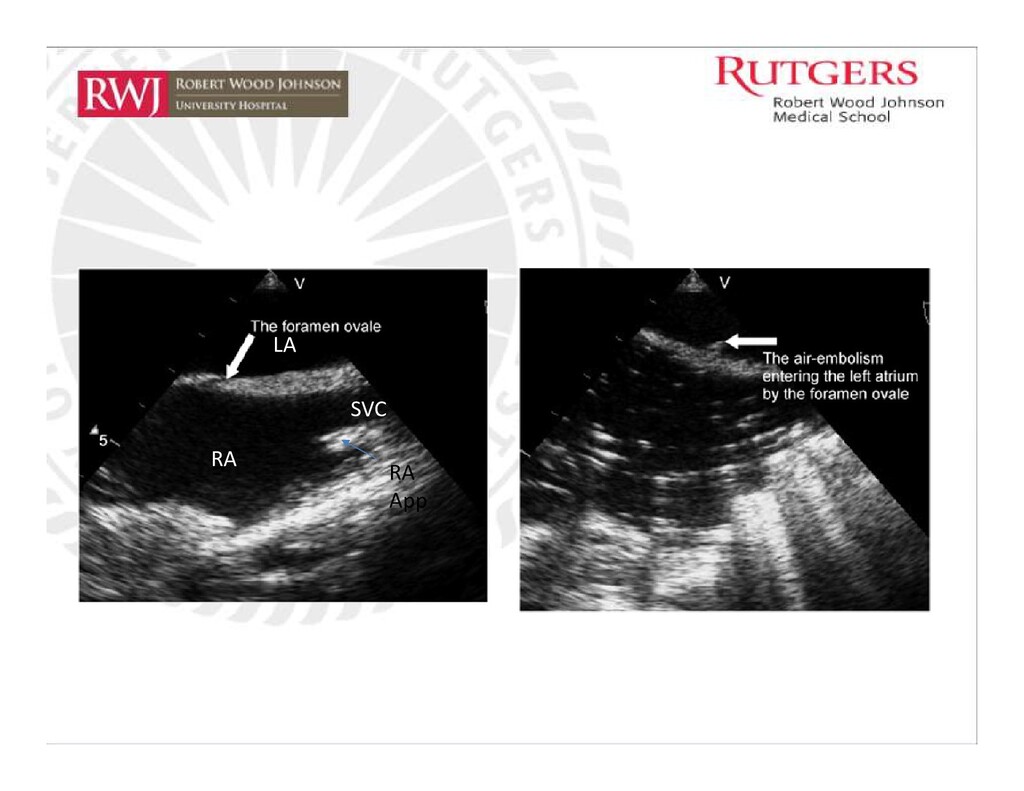
above the heart – veins in the cut-edge of bone and dural veins may not collapse when transected • Air enters pulmonary circulation – Microbubbles - bronchoconstriction with release of inflammatory/endothelial mediators and pulmonary edema • Endothelial damage: accumulation of platelets, fibrin, lipid droplets • Activation of complement and free radicals capillary damage and non-cardiogenic pulmonary edema • V/Q mismatch – increased alveolar dead space w/ hypoxemia and hypercapnia – Larger bubbles - trapped in right ventricle leading to RV failure • Decreased pulmonary VR decreased CO tachyarrhythmia/bradyarrhythmia arrest • Death is usually from cardiovascular collapse and arterial hypoxemia – Morbidity: 5mL of air – Mortality: as little as 20mL of air
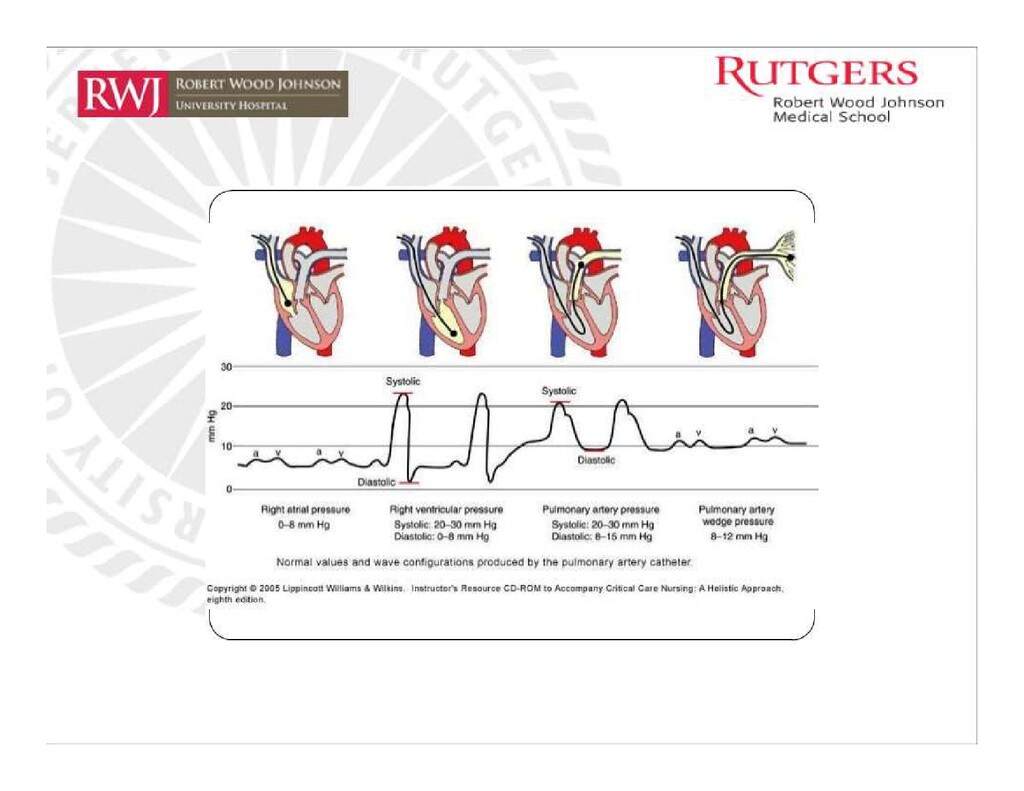
sensitivity = 76% o Capability: 0.02mL/kg of air 2) Precordial doppler ultrasound w/ EtCO2 – sensitivity = 40% o Left/right parasternal between 2nd and 3rd ribs o Capability: 0.05mL/kg of air 3) CVC: diagnostic and therapeutic – if correctly positioned at junction of SVC and RA o Possibility of aspirating air 4) Pulmonary Artery Catheter – increased pulmonary artery pressure o Normal: 20-30/8-15 mmHg o Systolic > 40 mmHg 5) Standard ASA monitors: o Blood pressure – hypotension o EKG – RV strain & ST depressions (low sensitivity) o Stethoscope – “mill-wheel” murmur (constant machine-like murmur)
2) Irrigation of operative site, apply occlusive dressings to all bone edges 3) Compression of Internal Jugular Veins 4) Place patient in head-down position, Durant Maneuver 5) 100% O2, IVF, pressor support * PEEP – can reverse pressure gradient between left and right atria and predispose air passage across PFO
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}