able to • Define different types of obstetric hemorrhage • Be able to describe contributing factors to postpartum hemorrhage • Prioritize treatments for postpartum hemorrhage
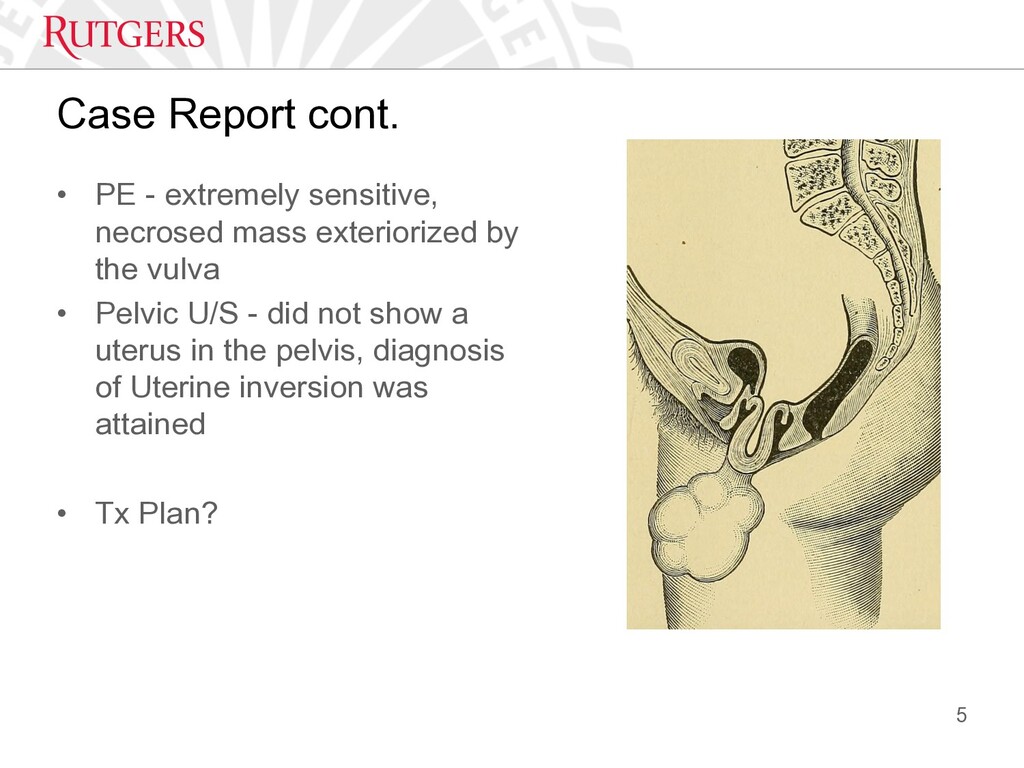
Delivered at home after a fast labor associated with abdominal expression and minimal traction of the umbilical cord at delivery. The newborn is a female of undefined weight. • Two hours later, and following the stage of expulsion, the parturient reports continued bleeding. • BIBEMS. Initial GE found a conscious and agitated patient. • Vitals - BP 100/70, HR 100, RR 20, T 38.6 • DDx? 4
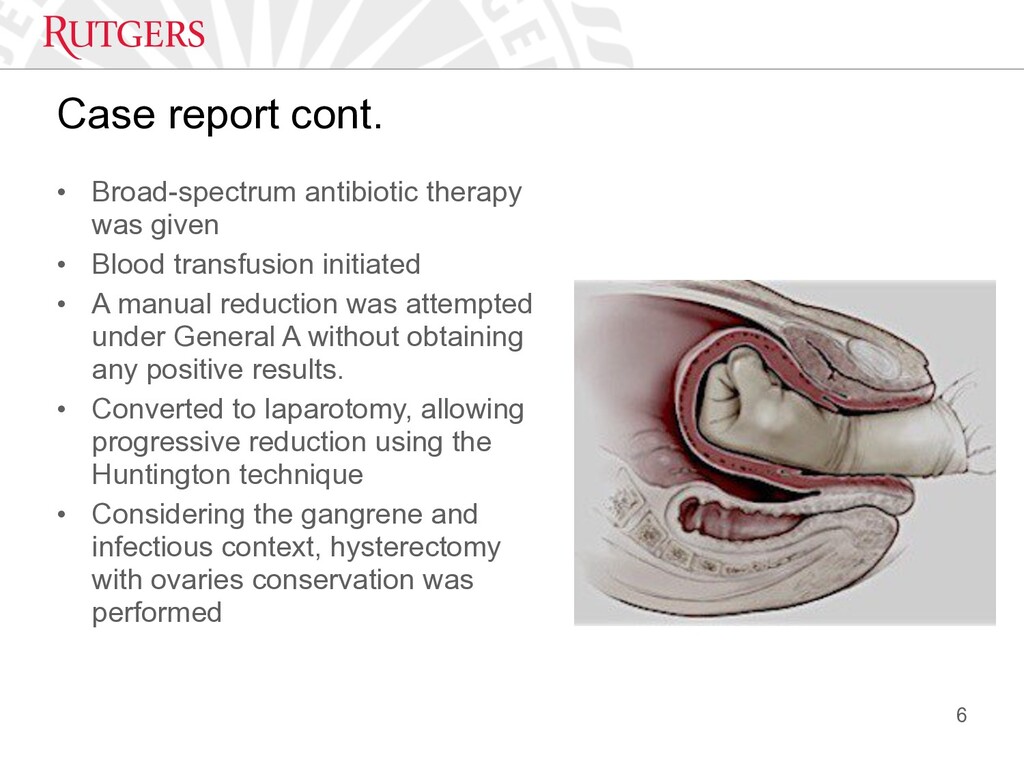
Blood transfusion initiated • A manual reduction was attempted under General A without obtaining any positive results. • Converted to laparotomy, allowing progressive reduction using the Huntington technique • Considering the gangrene and infectious context, hysterectomy with ovaries conservation was performed 6
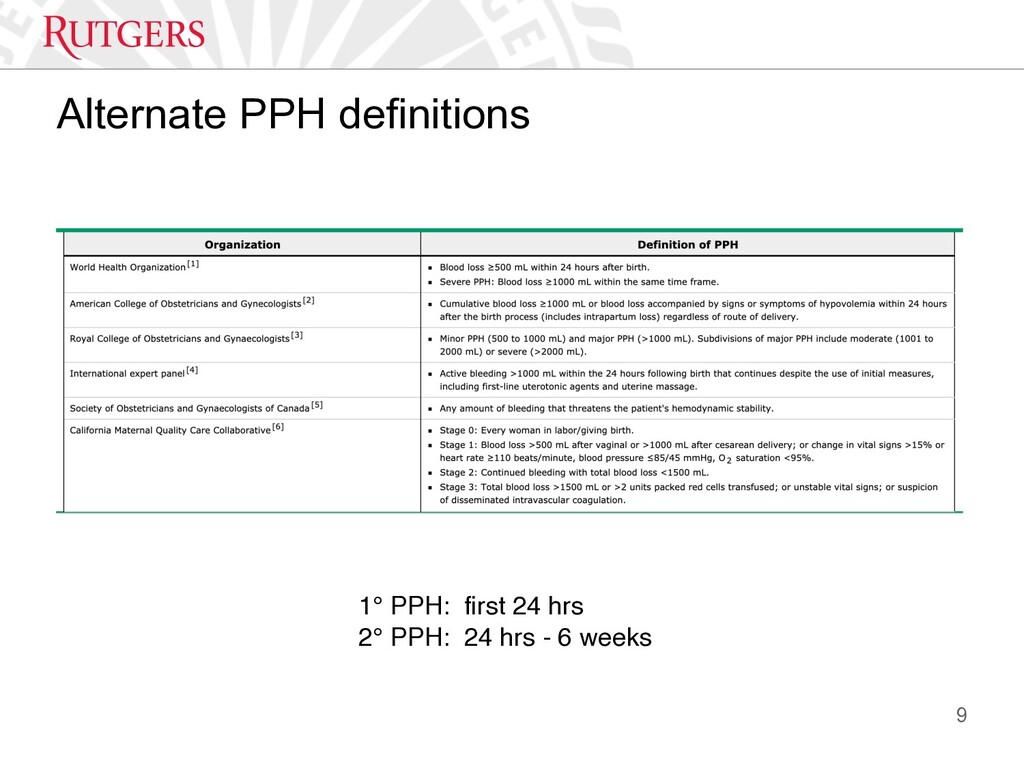
• Wide variations worldwide depending on both the overall health + resources for treatment • Death rates vary from 0.6 percent in the United Kingdom to 20 percent in parts of Africa • From 1:100,000 deliveries in the United Kingdom to 1:1000 deliveries in developing world 7 World Health Organization. WHO Recommendations for the Prevention of Postpartum Haemorrhage. Geneva, WHO, 2007. Ford JB, Roberts CL, Bell JC, et al. Postpartum haemorrhage occurrence and recurrence: A population-based study. Med J Aust 2007; 187:391-3.
-> compresses the blood vessels supplying the placental bed + causes mechanical hemostasis • Local decidual hemostatic factors -> tissue factor, type-1 plasminogen activator inhibitor, systemic coag factors (eg, platelets, circulating clotting factors) • Most remaining d/t loss of intact vasculature (ie, trauma) • Consistent potential for massive hemorrhage in late pregnancy -> uterine artery blood flow is 500 to 700 mL/min and accounts for approximately 15 percent of cardiac output 10
that compared 666 cases of PPH vs controls, associated risk factors were: • Retained placenta/membranes (odds ratio [OR] 3.5, 95% CI 2.1-5.8) • Failure to progress during the second stage of labor (OR 3.4, 95% CI 2.4-4.7) • Laceration (OR 2.4, 95% CI 2.0-2.8) • Large for gestational age (eg, >4000 g) (OR 1.9, 95% CI 1.6-2.4) • Hypertensive disorders (preeclampsia, eclampsia, HELLP (OR 1.7, 95% CI 1.2-2.1) • Induction of labor (OR 1.4, 95% CI 1.1-1.7) 11 Obstetric risk factors and outcome of pregnancies complicated with early postpartum hemorrhage: a population-based study. Sheiner E, Sarid L, Levy A, Seidman DS, Hallak M J Matern Fetal Neonatal Med. 2005;18(3):149.
Gestational Age presents for elective C-Section for history of 3 prior C Sections. Her past OB history is significant for preclampsia. A combined spinal epidural is placed in the OR without complication and immediately after delivery of the fetus you start an oxytocin infusion. However, blood loss continues and has reached 800ml in the past 5mins and is continuing. What is the most likely cause of her bleeding? A. Placenta accreta B. Cervical laceration C. Uterine atony D. Retained placenta • 13
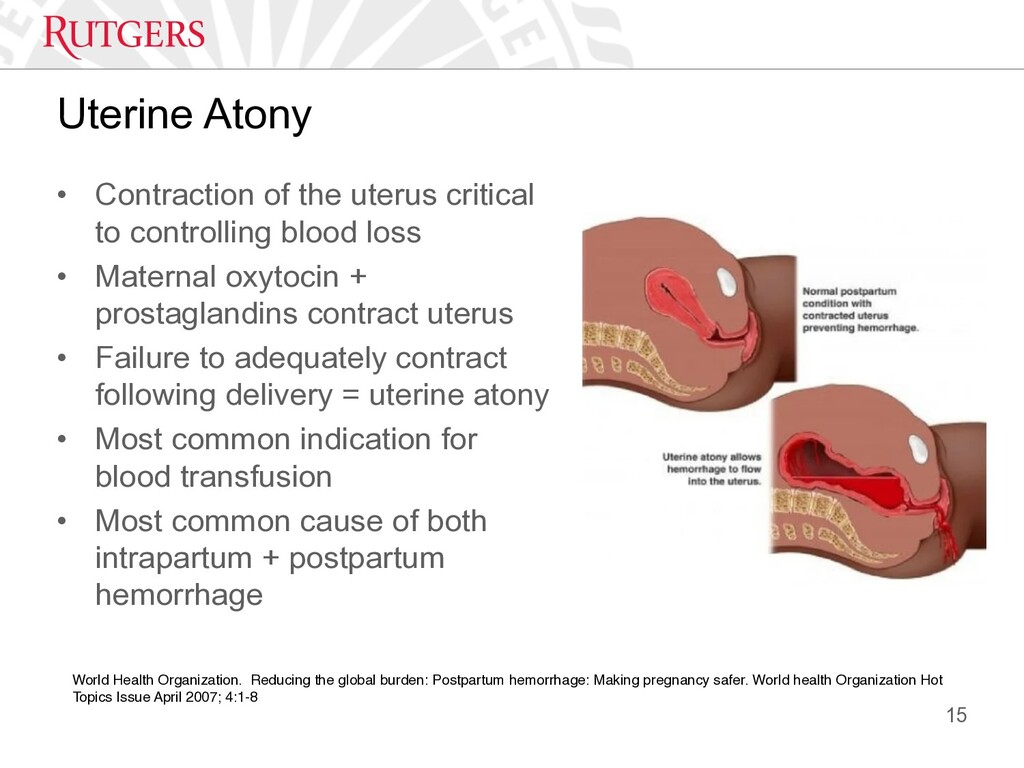
blood loss • Maternal oxytocin + prostaglandins contract uterus • Failure to adequately contract following delivery = uterine atony • Most common indication for blood transfusion • Most common cause of both intrapartum + postpartum hemorrhage 15 World Health Organization. Reducing the global burden: Postpartum hemorrhage: Making pregnancy safer. World health Organization Hot Topics Issue April 2007; 4:1-8
uterine compression • Confirm oxytocin administration • Address IV access if blood transfusion needed • Explore uterine cavity for retained placenta fragments • Inspect cervix + vagina for lacerations • Insert Foley to monitor UOP • Begin volume resuscitation, re-consider blood product transfusion 18 Alexander James M, Wortman Alison C. Intrapartum Hemorrhage. Obstet Gynecol Clin N Am 2013; 40:15-26
history of well controlled asthma, is being taken back for an urgent C section for failure to progress. She has been on an oxytocin infusion for the past 8hours for augmentation. Her epidural is titrated to achieve surgical anesthesia for the C-section and a healthy baby boy is delivered. However the Ob residents looks over and says to you that her uterus looks boggy can you give her some utertonic agents. Which of the following agents are relatively contraindicated? A. Oxytocin 20 Units infusion B. Methylergonovine 200mcg im C. Prostaglandin E1 100mcg per rectum D. 15 Methyl Prostaglandin F 2 Alpha 250mcg im • 19
delivery of placenta > 30 min 1. Trapped or incarcerated - placenta is trapped behind a partially closed cervix 2. Placenta adherans – placenta adheres to the endometrial lining, manually separates 3. Placenta accreta – placenta is abnormally adherent to the myometrium, no signs of separation 21 Magann EF, Evans S, Chauhan SP, et al. The length of the third stage of labor and the risk of postpartum hemorrhage. Obstet Gynecol 2005; 105 (2): 290-293
may proceed with existing CSE or epidural • Existing single shot spinal is unlikely to provide sufficient duration for complicated surgery and GA should be considered • Unstable with existing neuraxial anesthesia ! GA should be strongly considered 33
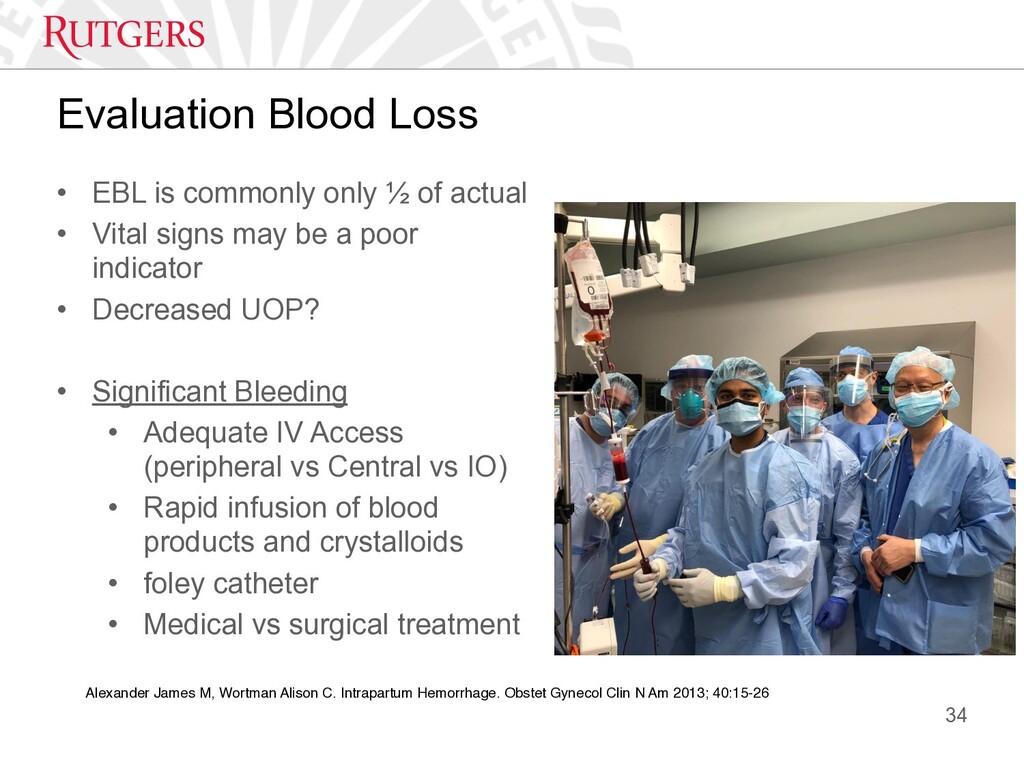
actual • Vital signs may be a poor indicator • Decreased UOP? • Significant Bleeding • Adequate IV Access (peripheral vs Central vs IO) • Rapid infusion of blood products and crystalloids • foley catheter • Medical vs surgical treatment 34 Alexander James M, Wortman Alison C. Intrapartum Hemorrhage. Obstet Gynecol Clin N Am 2013; 40:15-26
sutures • Intrauterine balloon tamponade • Angiographic arterial embolization • Bilateral surgical ligation 36 Allam MS, B-Lynch C. The B-Lynch and other uterine compression suture techniques. Int J Gynaecol Obstet 2005; 89:236-41 Doumouchtsis SK, Papageorghiou AT, Aruklumaran S. Systematic review of conservative management of postpartum hemorrhage: What do to when medical treatment fails. Obstet Gynecol Surv 2007; 62:540-7
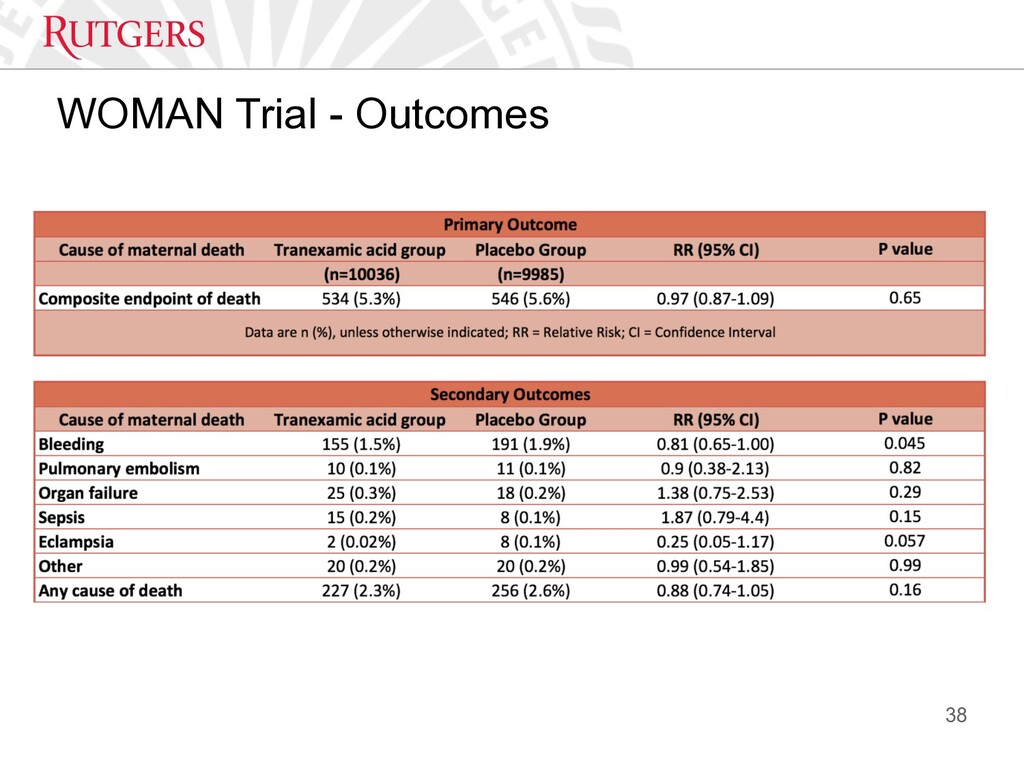
for the treatment of PPH (2017) • Clinical question - Does the early administration of tranexamic acid (TXA), compared with placebo, reduce death from bleeding in women with post-partum haemorrhage (PPH)? • Design - large, multicentre, Double-blinded, RCT • Population - 16+, clinical diagnosis PPH, 20,060 enrolled • Intervention - Tranexamic Acid (n=10036), 1g (10mg/ml) IV over 10 min 37
Postpartum Hemorrhage 1. Tone – uterine tone* 2. Tissue – retained placenta 3. Tissue – placenta accreta 4. Trauma – genital trauma 5. Turned Inside Out – uterine inversion 1. Ensure adequate IV access (PIV vs IO vs CVC) 2. Administer uterotonics 3. Assess blood loss and transfuse as indicated 4. Call for help and initiate the Massive Transfusion Protocol 39 Treatment
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}