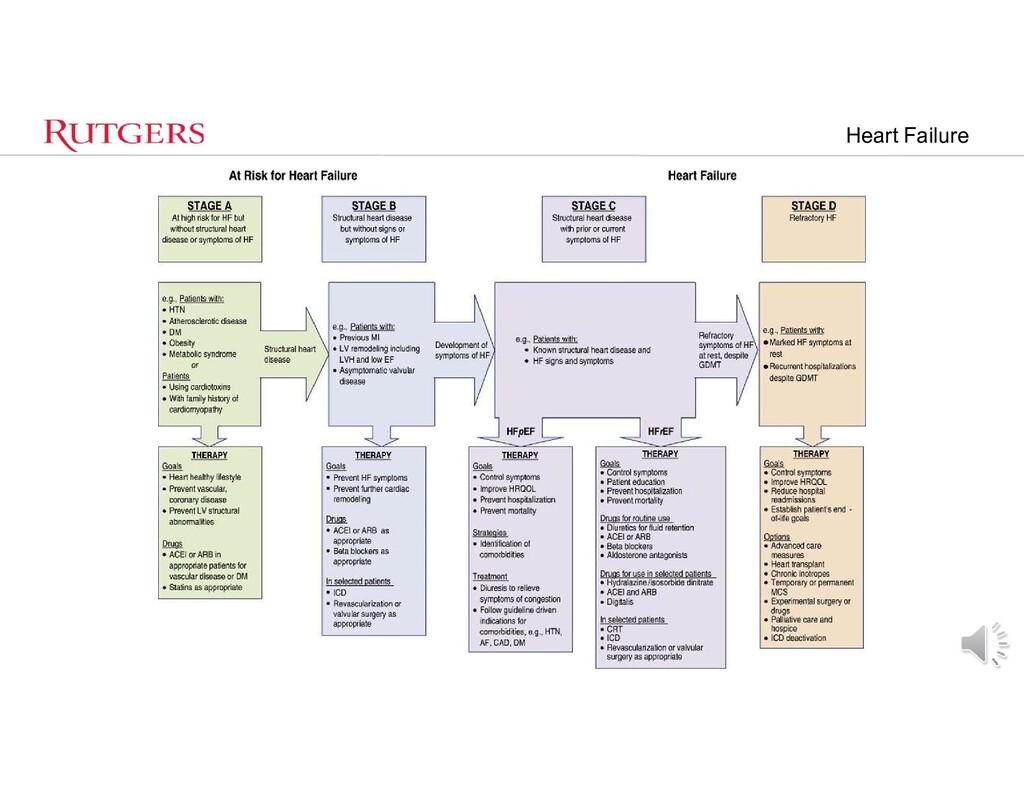
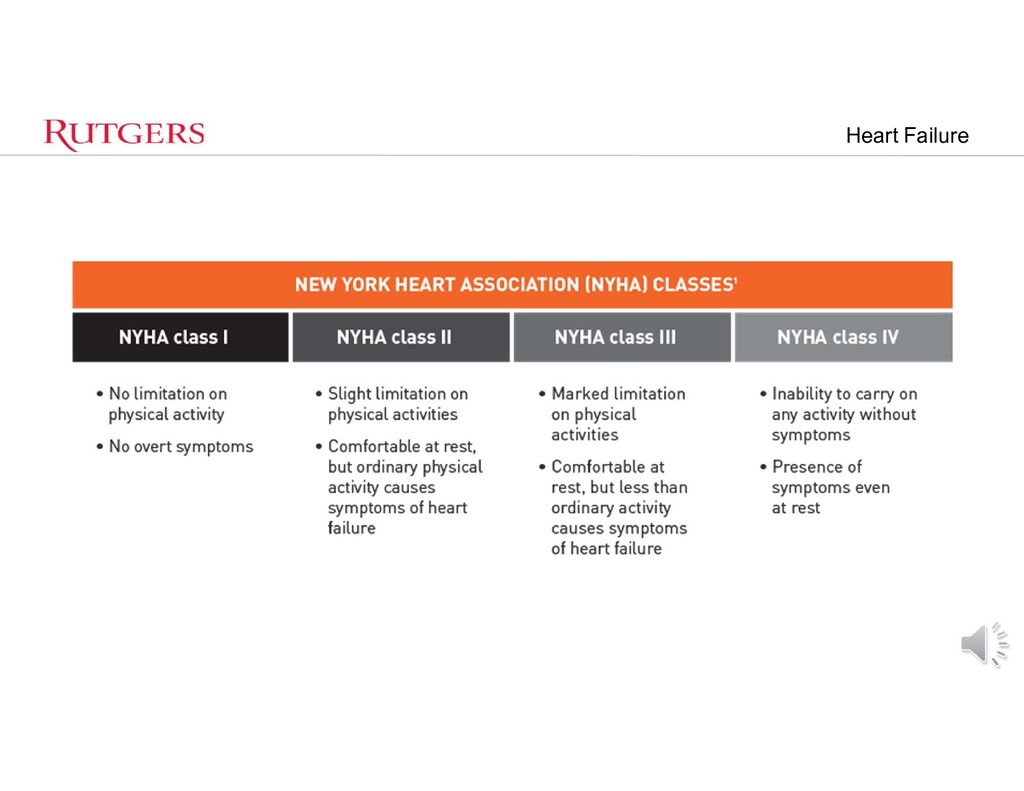
congestive HF – Incidence • 15.2 per 1000 after age 65 • 31.7 per 1000 after age 75 • 65.2 per 1000 after age 85, with 1,106,000 hospital discharges for heart – HF is the leading cause of hospitalization in patients older than 65 – Cost of $24 to $50 billion annually. • Patients with New York Heart Association (NYHA) Class IV symptoms currently have a reported 1-year mortality rate of 30% to 50%. • Rates for NYHA Class I-II patients and Class II-III patients are 5% and 10% to 15%. • Major goals in the management is the prevention of progression.
of HF symptoms with medical management, the underlying pathophysiology inevitably progresses, – pharmacologic interventions alone eventually will become inadequate – A variety of surgical procedures can be performed to improve cardiac function and potentially arrest (or even reverse) the progression.
pressure trigger the release of endogenous natriuretic peptides that promote diuresis. • Activation of the sympathetic nervous system causes peripheral vasoconstriction and increases the inotropic state of the myocardium. – Act to decrease excessive preload and restore wall tension to normal • Maintain cardiac output (CO) and arterial blood pressure (BP) in the face of mildly depressed ventricular function. – Eventually, the carotid, ventricular, and aortic arch baroreceptors are activated by the relative hypovolemia • leads to further activation of the sympathetic nervous system the renin-angiotensin-aldosterone axis, and the release of vasopressin. – The resultant peripheral vasoconstriction, mild fluid retention, and further increases in heart rate and inotropy will again compensate for the failing heart.
myocardial β1-adrenergic receptors to downregulate, and as ventricular function deteriorates, left ventricular (LV) end-diastolic volumes and pressures again increase – Results in adverse myocardial remodeling. • Dilation and hypertrophy – Progresses to decreased Cardiac Output, increased oxygen demand and so begins the vicious cycle • Increased LA and pulmonary pressures → RV failure
to decelerate the progression to severe failure, reduce adverse myocardial remodeling, and enhance survival – ACEI – Beta Blockers – Aldosterone Antagonists – Agents that improve symptoms but not long term survival • Diuretics • Digoxin
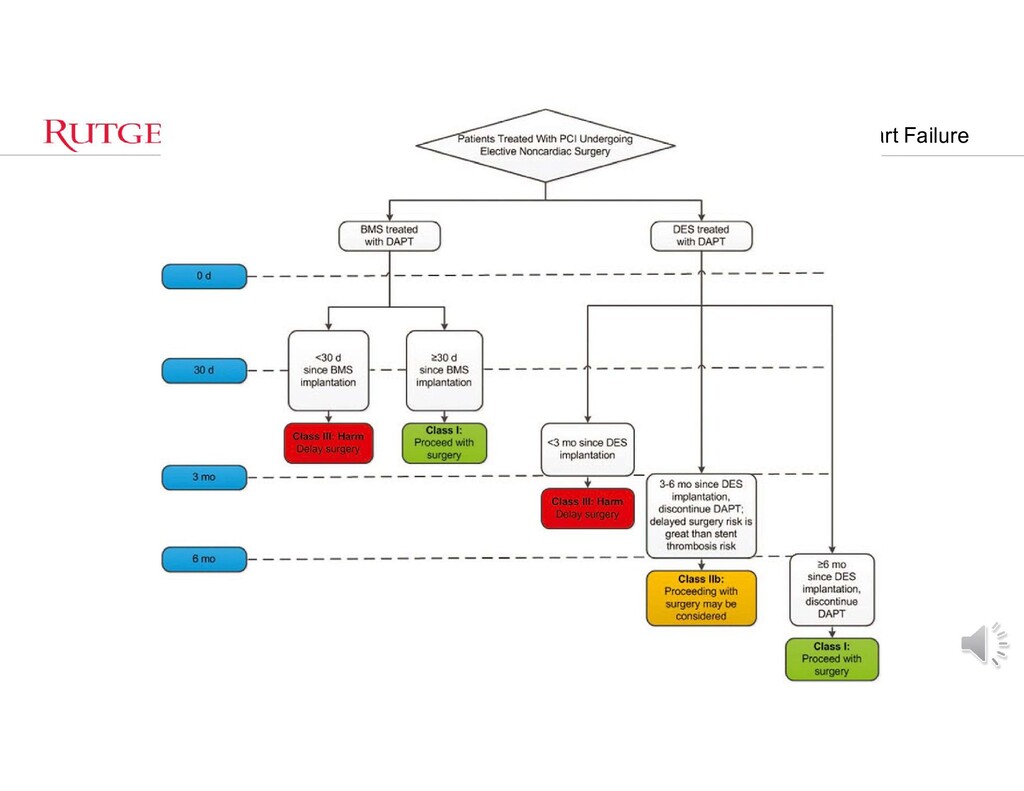
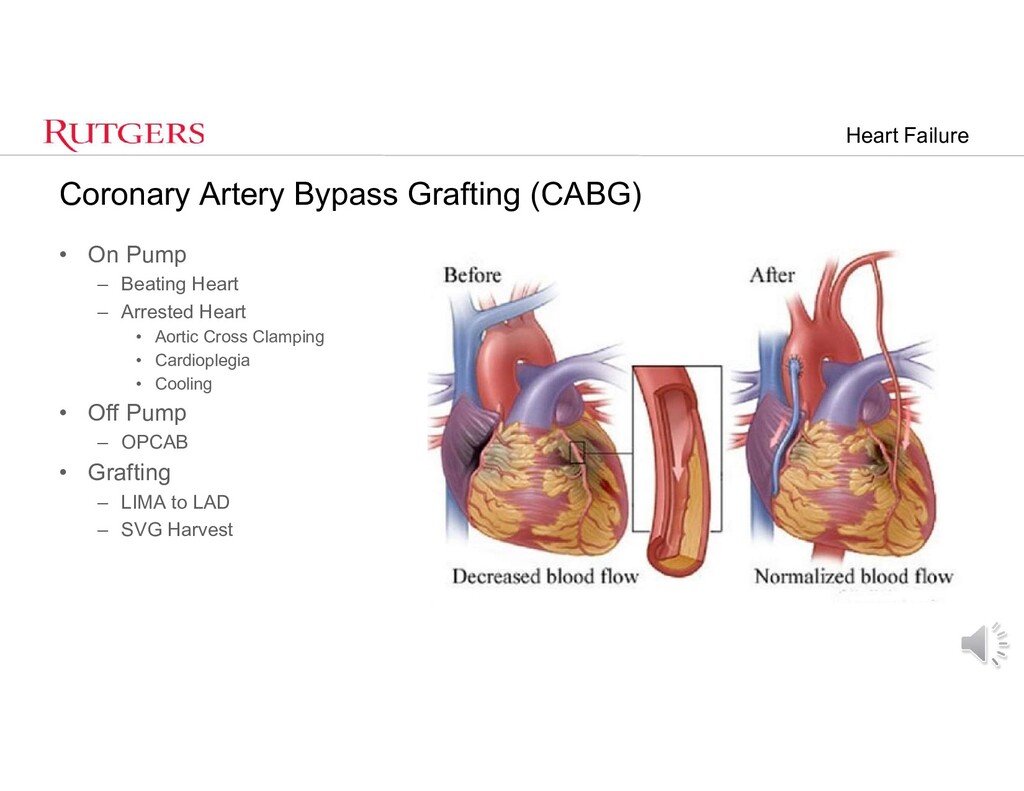
with biventricular pacing • Revascularization (coronary artery bypass grafting or percutaneous coronary artery stenting) • Mitral valve repair or replacement • Surgical ventricular restoration • Implantation of a left ventricular assist device • Cardiac transplantation • New therapies for congestive heart failure in various stages of development include transplantation of skeletal myoblasts and stem cells, “gene” therapy, and xenotransplantation
most common cause of HF • Where viable myocardium and feasible targets exist, revascularization of chronically ischemic, hibernating myocardium can improve ventricular function, downgrade NYHA functional class, and improve prognosis. – Ischemic • Insufficient oxygen supply to meet myocardial oxygen demand – Stunned • Acute myocardial dysfunction after an ischemic event with potential for full recovery – Hibernating • Chronically ischemic, dysfunctional myocardium with potential for full recovery – Maimed • Dysfunctional myocardium on the basis of ischemia that does not fully recover – Infarcted – Myocardial necrosis caused by ischemia with no potential for recovery
then no reason to revascularize – Dobutamine stress echocardiography • improvement in mechanical contraction under pharmacologic stimulation – Single-photon emission computed tomography – Positron emission tomography – Cardiac magnetic resonance imaging • Nuclear Medicine Thallium Viability Scan – Injection of Thallium – Thallium taken into good portions of heart muscle and not absorbed by scarred/dead tissue – Pictures taken at various intervals show amount of thallium tracer
cardiac and respiratory support to persons whose heart and lungs are unable to provide an adequate amount of gas exchange to sustain life. • Hypoxemic respiratory failure • Cardiogenic Shock • Cardiac Arrest • Failure to wean from CPB • Bridge to Transplant or VAD
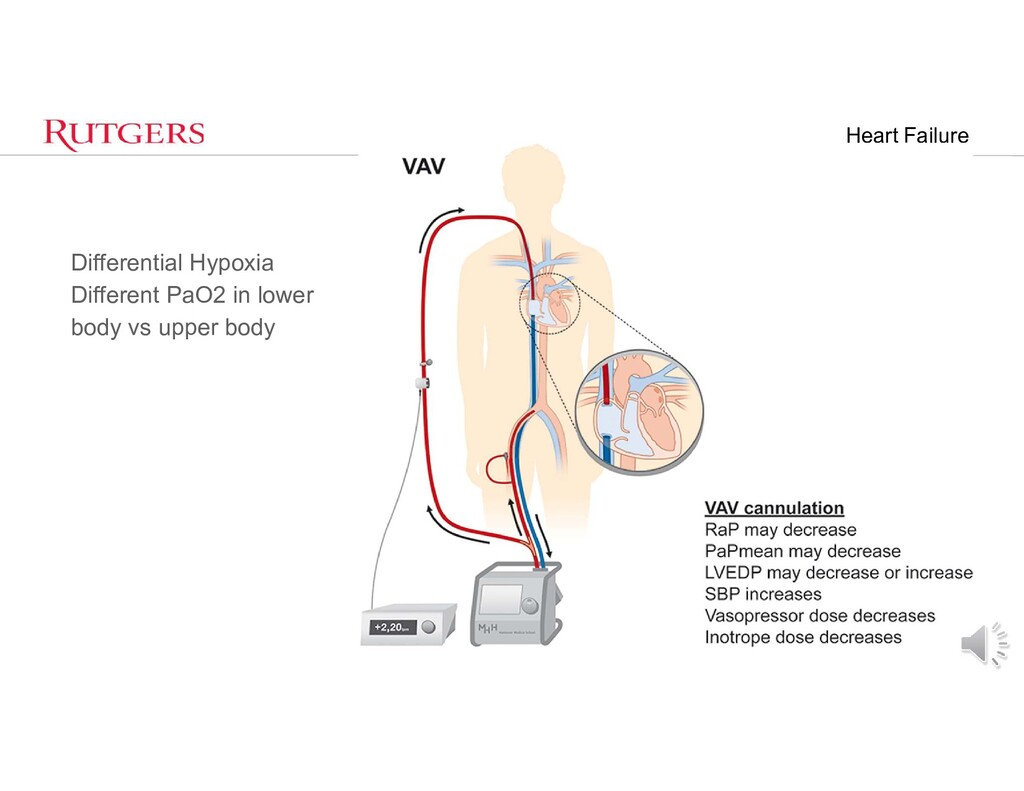
cannulae placed in the right common femoral vein for drainage and right IJ for infusion. • Alternatively, a dual-lumen catheter is inserted into the right internal jugular vein, draining blood from the superior and inferior vena cavae and returning it to the right atrium. – Veno-arterial (VA) • Venous Cannula placed in Right CFV for drainage and Arterial Cannula placed into RFA. • Central ECMO – If Chest is open – Cannulate RA and Ascending Aorta
- Weaning from CPB - Left Main Disease - High Risk PCI Contraindications - Severe AI - Aortic Dissection - Severe Vascular Disease - Sepsis - Aortic/Aortafemoral Grafts - AAA
as LVAD or RVAD or ECMO • Requires Anticoagulation – Usually heparin infusion • LV – Inflow to device from LV Apex – Outflow to Ascending Aorta • RV – Inflow to device from RA – Outflow to Pulmonary Artery
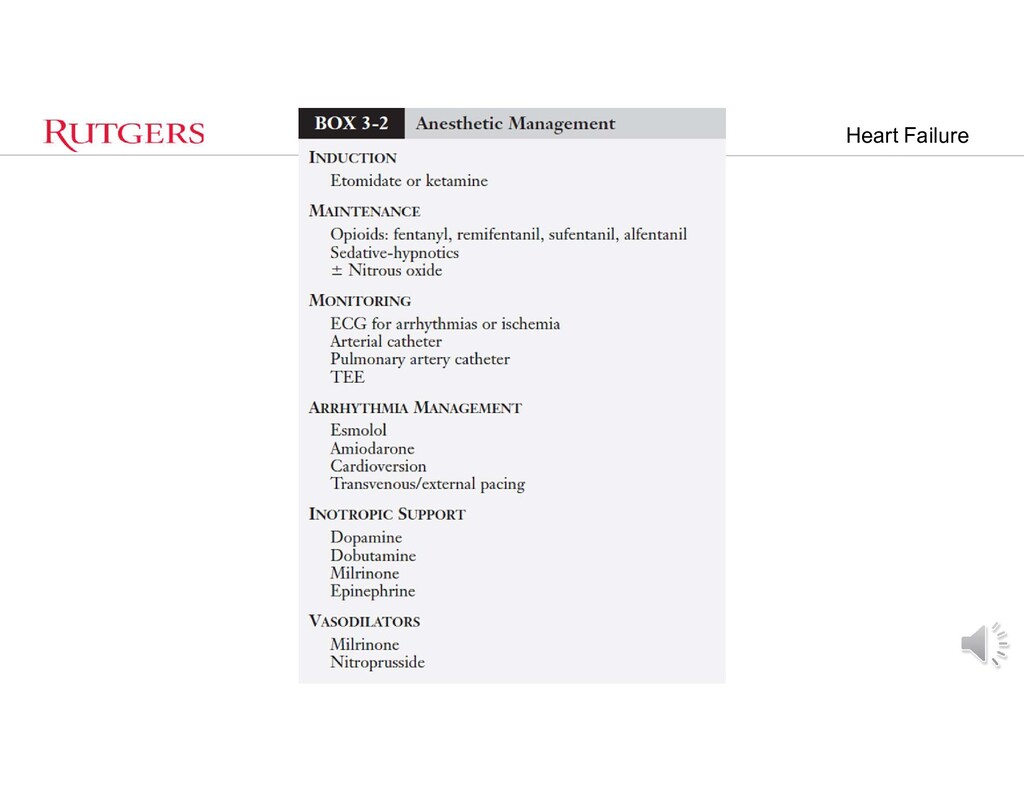
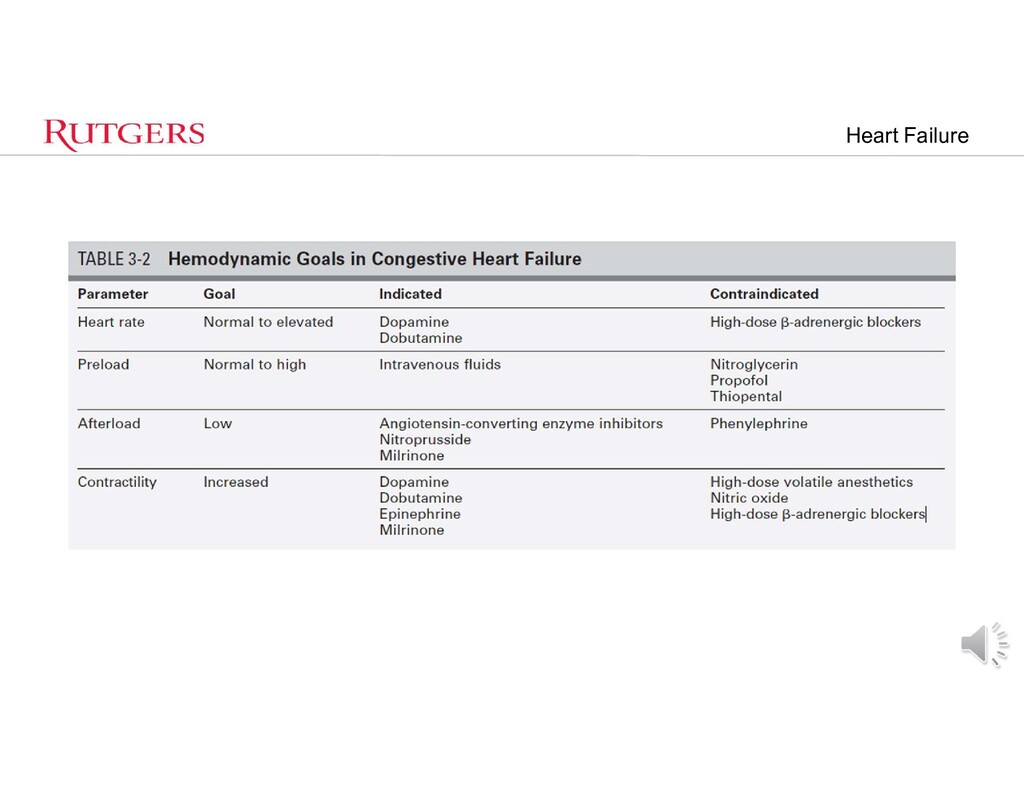
high catecholamine state • Removal of sympathetic tone may lead to CV collapse – Hypercarbia, hypoxemia, hypotension, Tachy/Brady/loss of Sinus • Renal or Hepatic Insufficiency – Affect anesthetic drug choices • Intravascular volume – What is optimization? • DRUGS – Ephedrine – Phenylephrine – Epi/Levo – Vasopressin – Milrinone
doses fentanyl or sufentanil with NMB • Amnesia? • Chest wall rigidity? • Significant Bradycardia • Etomidate – No change in contractility • Propofol – Induction with decreases in SVR
• Myocardial depressants – Iso/Des causes more decreases in SVR than SEVO • Ketamine – 1 – 2.5 mg/kg IV • Hemodynaic stability with analgesia and amnesia • Sympathetic Side effects • PERICARDIAL TAMPONADE DRUG OF CHOICE
cardiomyopathy (DCM) presented for open reduction and internal fixation of a tibial fracture. He had been in a motor vehicle accident. • Past medical history included alcohol abuse, orthopnea, dyspnea on exertion, and several episodes of pulmonary edema. The patient’s medications included digoxin, furosemide, and captopril. Physical examination revealed bibasilar rales and S3 gallop. A gated blood pool scan showed a left ventricular ejection fraction of 15%. Cardiac catheterization indicated a cardiac index of 1.8 L/min/m2, 2+ mitral regurgitation, and no coronary artery disease.
account dysfunctional RV • GA usual choice – Patients anticoagulated • Superficial regional blocks or Bier Block • Intubation/Extubation criteria unchanged – Old LVAD considered Full Stomach • Extubate early – Avoid post op VAP – NO REASON TO KEEP INTUBATED
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}