True Art of Anesthesia Case Conference, Rutgers Robert Wood Johnson University Hospital Department of Anesthesiology September 16, 2020 Christopher W. Fjotland, MD Assistant Professor & Chief Division of Neuroanesthesiology & Division of Head and Neck Anesthesia & Advanced Airway Management Co-director of Medical Education Department of Anesthesiology & Perioperative Medicine Rutgers Robert Wood Johnson University Hospital Communications Board Member, Director of Content & Assistant Editor Society for Neuroscience in Anesthesiology and Critical Care
What is an awake craniotomy? • Surgery that is performed on the brain while the patient is in a state of awareness • Cooperation with functional testing of the cortex • Indications • Eloquent cortex preservation (tumor or ictal foci resection) • Epilepsy surgery • Deep brain stimulator placement • Minimally invasive surgery • Benefits (Reduce) • Size of resection • Surgical time • Post-operative neurological deficits • Early post-operative nausea and vomiting • Hospital stay • Post-operative opioids
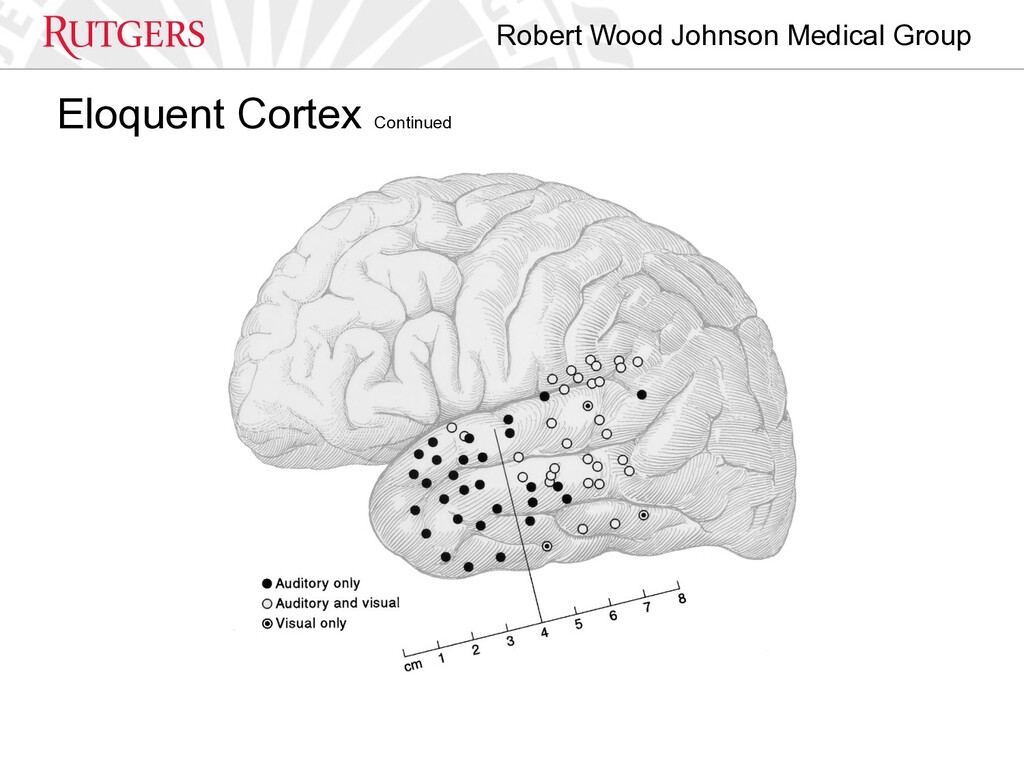
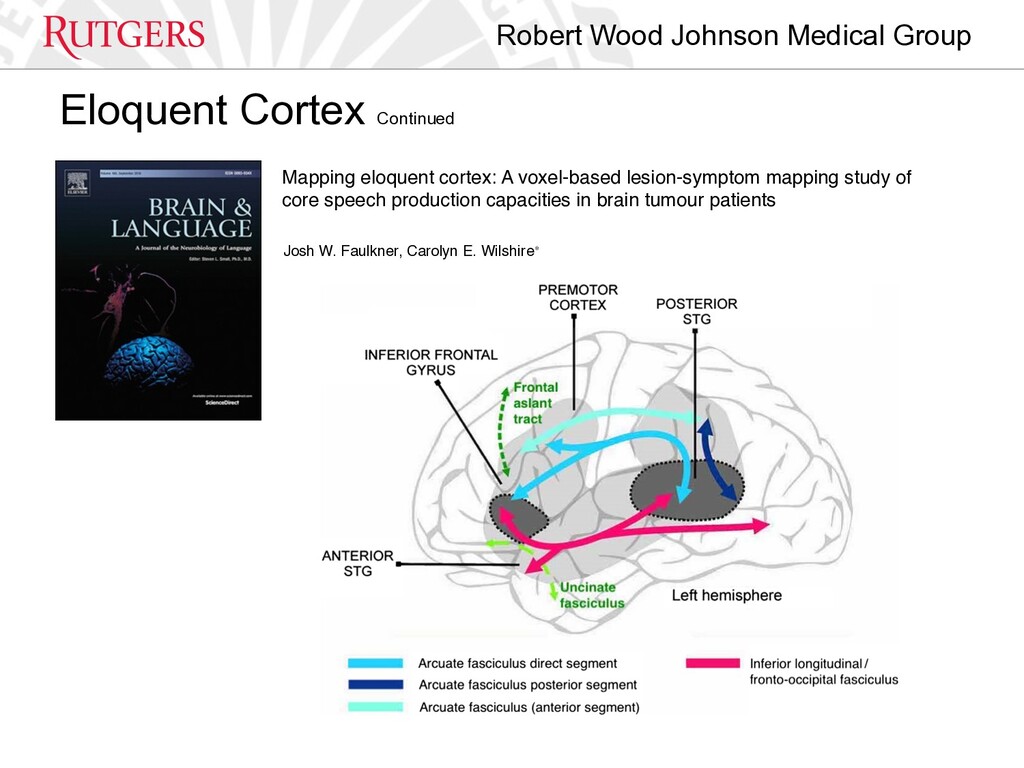
lesion-symptom mapping study of core speech production capacities in brain tumour patients Josh W. Faulkner, Carolyn E. Wilshire⁎ Eloquent Cortex Continued
rapport • Very clearly/honestly describe the perioperative process • Set realistic expectations • YOU are their advocate • Make it clear that they have options intra-operatively • Goals: • Best possible resection • Patient comfortable • Patient safety
Pearls • MAC: Varying levels of sedation (very deep until dura is open) • Airway: O2 4L/min via salter nasal cannula • **Appropriate size nasal trumpets w/ lido jelly for lubrication, appropriate size oral airway, appropriate size LMA & video laryngoscope/ETT all readily available** • Access: 2 PIV Monitors: Standard ASA + A-line + Foley • *1 PIV - TIVA* *1 PIV - bolus line* • **TIVA line carrier on a pump set at a constant rate and must be clearly marked with all stop-cocks taped closed to prevent accidental bolus** • Sedation: TIVA: Dexmedetomidine: Load 1mcg/kg over 10 minutes, Maintenance 0.3 mcg/kg/h; Remifentanil: 0.08 mcg/kg/min. Carrier (NS): 200 cc/h. Bolus: Propofol 0.1 mg/kg *titrated very slowly as can work synergistically with Dex/Remi cause obstruction/apnea with low doses* • Scalp Block: 0.25% Bupivacaine (~80cc total *under toxic dose) • Anti-epileptic: Levetiracetam 500-1000mg, Special: +/- Mannitol 0.5-1g/kg, +/- Furosemide, +/- Dexamethasone • **The brain will be “tight” (secondary to hypoventilation) and so a pre-op discussion with the surgeon should occur as far as how to handle that** (positioning - reverse trendelenburg, minimize head turn will help) • Antibiotic: Cefazolin 2g (3g >120kg) • Ice cold saline irrigation on the field & additional irrigation on ice • Continue TIVA sedation until dural opening, then turn off all drips including carrier. Patient expected to emerge over 7-8 minutes. • **Important to have a propofol syringe on the bolus line ready for administration, if needed**
• Nausea, Vomiting & Aspiration • Propofol > mixed agent sedation • Prevention: prophylactic antiemetic • Treatment: (RAPID) Metoclopramide, ondansetron. Additional local anesthetic to dura. • If aspiration does occur these patients should be intubated with the use of video laryngoscopy and thoroughly suctioned
• Brain swelling • Prevention: Optimize positioning (head up, less head turn), early mannitol 0.5-1 g/kg +/- furosemide • Treatment: Wean sedation to respiratory rate of 8-12 BPM, controlled hypotension, steepen reverse trendelenburg or back-up, consider re-dose mannitol or add furosemide, discuss possible CSF drainage from the surgical field, consider waking the patient up to increase RR
• Anxiety, disinhibition & patient movement • Prevention: Patient selection & preoperative counseling! Careful/ patient specific anesthetic selection. • Treatment: reorienting the patient on emergence, reassuring, PROPOFOL —> deepen sedation and re-attempt emergence, consider continuing Dexmedetomidine drip during “awake” portion, consider converting to general anesthesia vs continuing deep sedation
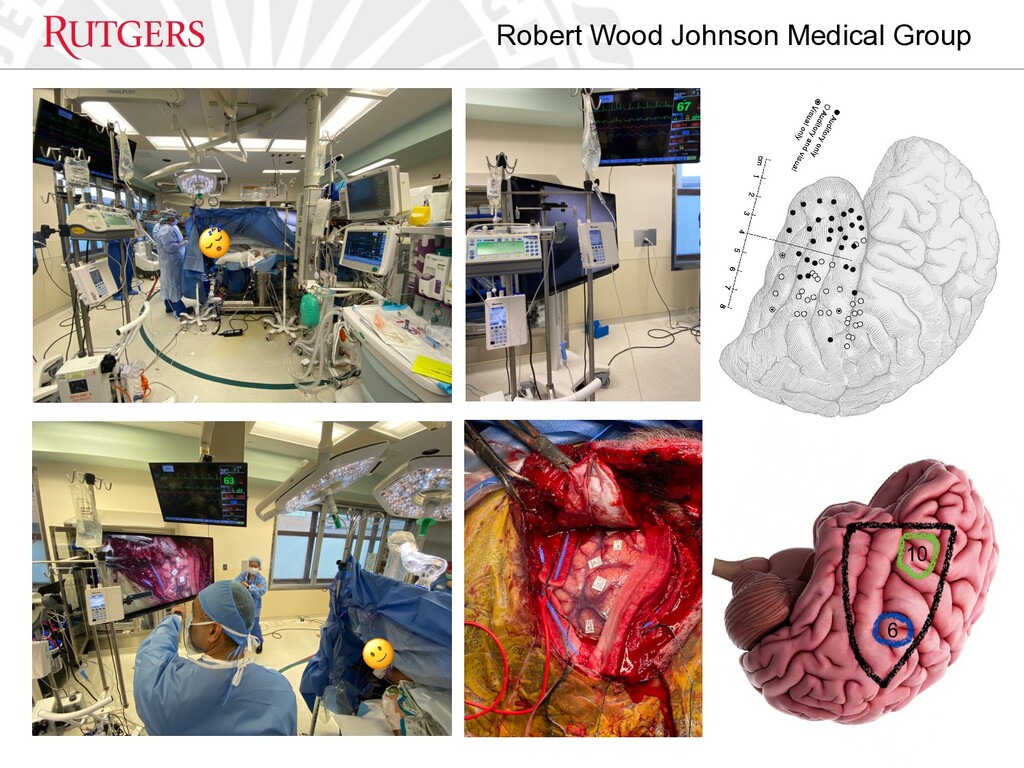
• Seizure • Most common during cortical mapping • Vigilance is critical! - communication with neuromonitoring technologist and surgeon • Prevention: prophylactic antiepileptic, early recognition of aura or seizure-like activity (patient or iEEG), use of ice cold irrigation between cortical stimulation, breaks between cortical stimulation (30 seconds-1 minute) • Treatment: Ice cold irrigation on the brain immediately followed by propofol (0.75-1.25 mg/kg), assess EEG for resolution, attempt re-emergence, repeat with increased dose of propofol if persists, consider re-dose antiepileptic, benzodiazepine, consider converting to GA
Indications: • Neurological d/o causing an alteration in function but not accompanied by gross structural or anatomical changes • Movement d/o (Parkinson’s, dystonia, essential tremor, Tourette’s) • Psychiatric d/o (depression, OCD, anorexia) • Other (chronic pain, epilepsy, Alzheimer’s, dementia) • Improve quality of life
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}