succinylcholine phase I and phase II blockade? 2. What conditions can lead to life-threatening hyperkalemia with succinylcholine administration? 3. Which medications commonly administered in the perioperative period can lead to enhanced action of nondepolarizing neuromuscular blocking drugs? 4. What are the potential adverse outcomes from residual neuromuscular blockade that may present in the post anesthesia care unit (PACU)? 5. What clinical and peripheral nerve stimulation tests most accurately predict adequate reversal of nondepolarizing NMBDs? 6. How does the mechanism of action of sugammadex differ from neostigmine, when used to antagonize nondepolarizing NMBD activity?
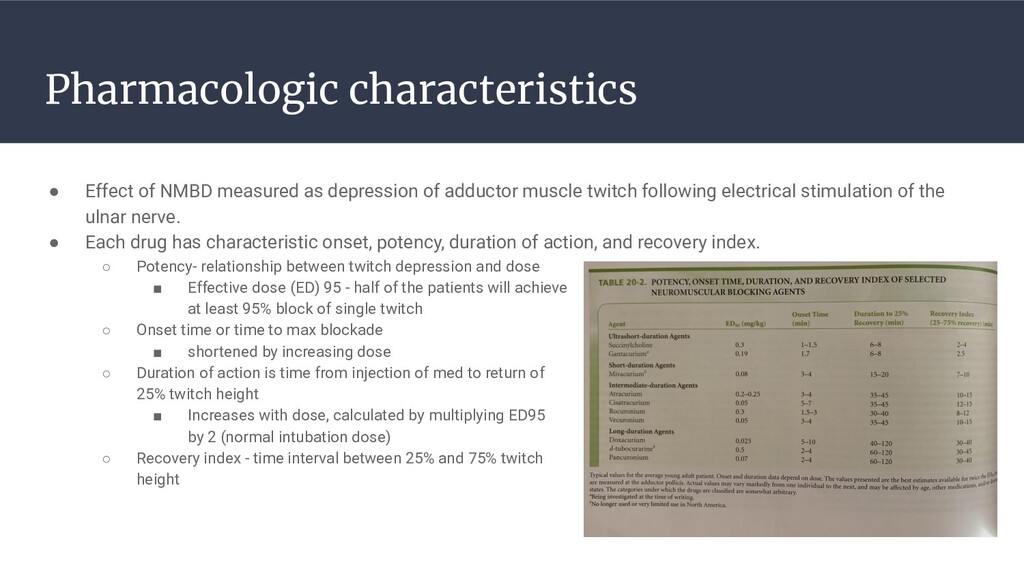
adductor muscle twitch following electrical stimulation of the ulnar nerve. • Each drug has characteristic onset, potency, duration of action, and recovery index. ◦ Potency- relationship between twitch depression and dose ▪ Effective dose (ED) 95 - half of the patients will achieve at least 95% block of single twitch ◦ Onset time or time to max blockade ▪ shortened by increasing dose ◦ Duration of action is time from injection of med to return of 25% twitch height ▪ Increases with dose, calculated by multiplying ED95 by 2 (normal intubation dose) ◦ Recovery index - time interval between 25% and 75% twitch height
RSI because of rapid onset and short duration of action • Interact with acetylcholine receptors by binding to both alpha subunits of the postsynaptic receptor preventing access to the receptors by Ach and depolarization the motor end plate. • Depolarization results in fasciculations prior to onset of paralysis ◦ Small dose of nondepolarizing drugs are effective in reducing the incidence of fasciculations • Can present with exaggerated sustained increase in tension in certain muscles, most commonly the masseter, resulting in masseter muscle spasm which can make intubation more difficult • Blockade can be potentiated by inhibitors of acetylcholinesterase, such as neostigmine and edrophonium, resulting in Phase II block • Rapidly hydrolyzed by plasma cholinesterase (pseudocholinesterase), elimination half life <1 min • Intubating dose 1-2mg/kg, based of actual body weight • larger more central muscles response first (diaphragm, laryngeal m., masseter), then adductor pollicis muscle, larger central muscles recover faster also, diaphragm recovers and spontaneous ventilation resumes after 5 mins
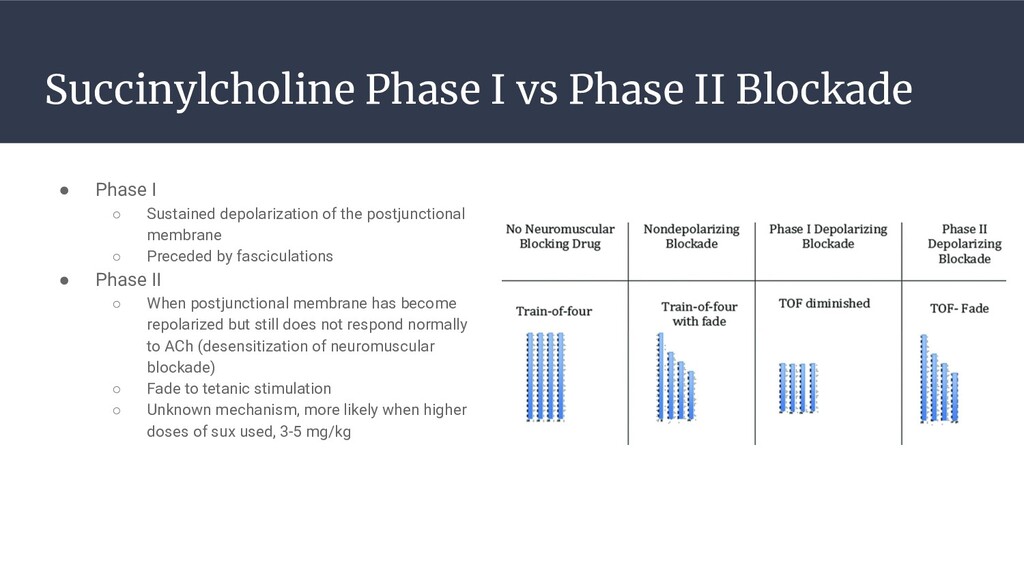
◦ Sustained depolarization of the postjunctional membrane ◦ Preceded by fasciculations • Phase II ◦ When postjunctional membrane has become repolarized but still does not respond normally to ACh (desensitization of neuromuscular blockade) ◦ Fade to tetanic stimulation ◦ Unknown mechanism, more likely when higher doses of sux used, 3-5 mg/kg
number of endogenous and exogenous causes such as pregnancy, liver disease, uremia, malnutrition, burns, plasmapheresis, and OCPs, leading to slight, clinically unimportant increase of duration of action of sux • Reduced by neostigmine and pyridostigmine increasing duration of action of sux • Atypical Plasma Cholinesterase ◦ Diagnosed by determining the dibucaine number ◦ Dibucaine is an amide local anesthetic that inhibits normal plasma activity by about 80%, atypical enzyme is inhibited about 20%; reflects the quality of plasma cholinesterase not quantity ◦ Dibucaine number 80 represents normal plasma cholinesterase function ◦ Heterozygous abnormal allele, dibucaine number 50-60, duration of action slightly prolonged (20-30 mins) ◦ Homozygous atypical allele, dibucaine number 20-30, have prolonged paralysis (2-6 hrs) after usual dose of sux
soluble, do not cross BBB or placenta • Bind to at least one of the two alpha subunits of the postsynaptic receptor preventing access to the receptor by Ach and does not produce opening of the receptor ( no depolarization) • Compete with Ach for same binding site • Can be antagonized by anticholinesterase agents like neostigmine • Dose requirements increased in burn patients secondary to increased protein binding and upregulation of receptors • Dose for obese pt calculated using lean body mass • The more potent the drug the longer the onset of action
termination half life about 20 mins • Degraded via nonspecific ester hydrolysis (tissue esterases) and Hofmann reaction (non enzymatic degradation with a rate that increases as temp and/or pH increase) • Laudanosine ◦ end product from degradation ◦ known to cause seizures (in animals, inconclusive human studies) ◦ Excreted in kidneys • Histamine release with larger doses >0.5mg/kg Cisatracurium • Potent isomer of atracurium with less histamine release • Degraded by Hofmann and ester hydrolysis • Intubating dose 0.15-0.2mg/kg and duration of action about an hour
onset (within 90 sec at dose of 0.6 mg/kg) • Eliminated by redistribution, most of the drug is excreted unchanged in bile, urine, and feces • Slightly prolonged duration of action in pt’s with renal or hepatic failure • MCC of anaphylactic reaction in the OR (along with vec) • Drug of choice for RSI if sux CI. (1 mg/kg) Vecuronium • Intermediate duration agent • Slower onset of action than roc • 60% excreted in kidneys
slower onset of action • Clearance decreased in renal and hepatic dysfunction • Associated with increased HR, BP, and CO • More likely to have residual paralysis and more difficult to reverse
blockade • Local anesthetics can potentiate the effects for depolarizing and nondepolarizing NMB drugs • Combo of two NDNMB agents is either additive or synergistic, depending on the two drugs involved ◦ Atracurium and cisatracurium are additive (half ED95 of atracurium plus half ED95 of cis will produce >95% block) ◦ Rocuronium and cisatracurium are synergistic (only ¼ ED95 of both drugs needs to be given to produce 95% block) ◦ Duration of action of the second agent given becomes that of the first because loading dose of first drug greater than maintenance dose of second, so receptors mostly blocked by first drug when second drug given • Depolarizing agents with nondepolarizing can result in potentiation or antagonism ◦ If NDNMB given before sux it is antagonizing, decreasing the potency of sux ◦ Depending on degree of nondepolarizing block, sux given if blockade is deep can antagonize the block, if given when the block is shallow may potentiate the block ◦ If anticholinesterase is given then the effect of sux is potentiated because of inhibition of plasma cholinesterase • Aminoglycosides and streptomycin can prolong blockade • Acute administration of phenytoin produced augmentation of NMB, chronic phenytoin shortens block • Magnesium can potentiate blockade by decreasing calcium • Metoclopramide inhibits plasma cholinesterase and prolongs action of sux and mivacurium
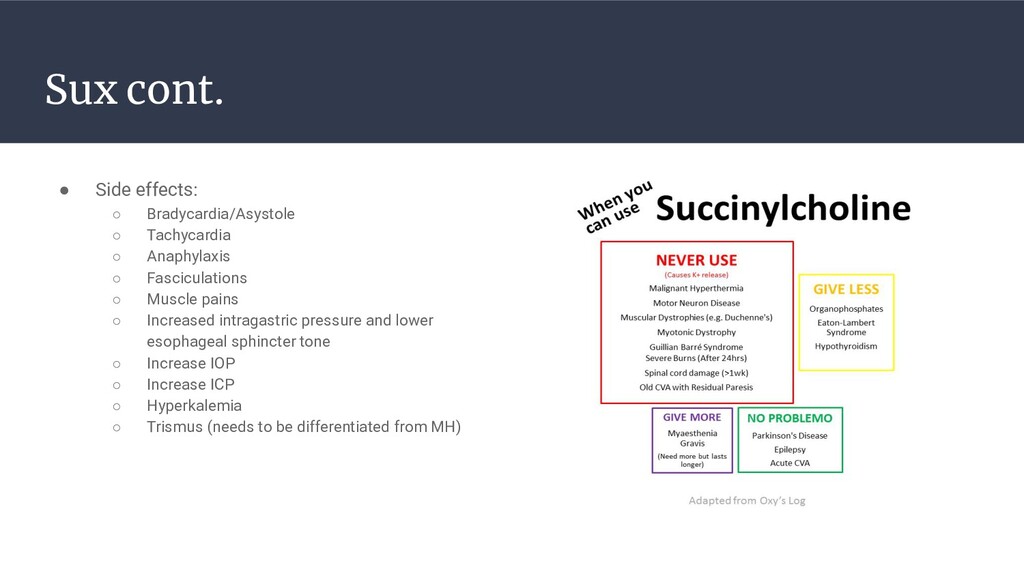
◦ Resistant to sux, sensitive to nondepolarizing drugs • Lambert Eaton Myasthenic Syndrome ◦ Sensitive to both sux and nondepolarizing drugs • Myotonia ◦ Sux CI, results in prolonged muscle contraction and exaggerated hyperkalemia • Muscular Dystrophy ◦ Hyperkalemia and rhabdomyolysis with sux administration • UMN Lesions ◦ Result in extrajunctional receptor proliferation ◦ Exaggerated hyperkalemia resulting in cardiac arrest with sux ◦ Resistance to nondepolarizing drugs below the level of the lesion • Burns ◦ Proliferation of extrajunctional receptors 24 hr after a burn results in exaggerated hyperkalemia with sux administration ◦ Resistance to nondepolarizing drugs • Central Hypothermia ◦ May slow metabolism of neuromuscular blocking drug, prolonging blockade
intervals >10 secs (<0.1 Hz); clinical use limited • Tetanus type of stimulation using 50 Hz frequency ◦ Tetanus with fade indicates residual neuromuscular blockade, if no fade is present then and response is sustained then neuromuscular blockade is absent ◦ Main disadvantage of this mode of stimulation is post tetanic facilitation which is an enhanced response to any type of stimulation for a short period of time after tetanus • Train of four uses 2 Hz stimulation ◦ >90% receptors blocked with single twitch visible ◦ 80-90% when two twitches visible ◦ 70-80% when three twitches visible ◦ all four twitched become visible when the blockade is 65-75%
profound neuromuscular blockade present there is no response to TOF or tetany, can apply tetanus and then TOF, if one post tetanic twitch presents then estimated time for twitch to reappear is 15-30 mins. • Double burst stimulation ◦ two short tetanic stimulations (three impulses at 50 Hz separated by 750ms) and by evaluating ratio of second to first response ◦ TOF may be difficult to detect by visual or tactile means, double burst may be easier to detect manually
ulnar nerve reflects upper airway muscle function for extubation (post tibial nerve stimulated behind the internal malleolus is comparable to adductor pollicis) • Facial nerve around the eye is a good indicator of intubating conditions because it reflects blockage or laryngeal adductors , innervated the corrugator supercilii which moves the eyebrow
TOF >0.6), tongue protrusion, hand grip, more sensitive test is ability to hold the jaw shut and prevent removal of tongue depressor or oral airway (correlates with TOF >0.86) • Residual paralysis is a common finding in the pacu and can present as oxygen desaturation, airway obstruction, and muscle weakness especially when reversal agent is not administered
concentration at the neuromuscular junction • Neostigmine ◦ Works on all cholinergic synapses in the PNS, potent parasympathomimetic activity is attenuated or abolished by the administration of an antimuscarinic agent, such as atropine (½ neo dose) or glycopyrrolate (⅕ neo dose) ◦ Ceiling effect, inability of larger dose to produce increasing effect ◦ Can only be given twitch is present, if given with no twitches leads to prolonged blockade ◦ Peak effect at 5 mins, duration of action 1 to 2 hrs ◦ Dose 0.03-0.07 mg/kg • Edrophonium ◦ Reaches peak in 1-2 mins but less effective than neostigmine • Pyridostigmine ◦ Fallen out of favor secondary to longer onset of action than neostigmine
• Gamma-cyclodextrin, made up of eight sugars arranged in a ring to make a center to accommodate the rocuronium molecule • Devoid of cardiovascular and other major side effects • Dose depends on degree of blockade, dosed on TBW ◦ 2 mg/kg if 2 or more twitches present ◦ 4 mg/kg if post tetanic twitches 2 or more ◦ 16 mg/kg for failed intubation and rapid reversal of roc RSI dose • Renally excreted, terminal half life approx 2 hrs • CI in patients with known hypersensitivity reactions • Use with caution in renal failure and pediatric patients • Leads to transient effect on hemostasis, increased PT
succinylcholine phase I and phase II blockade? 2. What conditions can lead to life-threatening hyperkalemia with succinylcholine administration? 3. Which medications commonly administered in the perioperative period can lead to enhanced action of nondepolarizing neuromuscular blocking drugs? 4. What are the potential adverse outcomes from residual neuromuscular blockade that may present in the post anesthesia care unit (PACU)? 5. What clinical and peripheral nerve stimulation tests most accurately predict adequate reversal of nondepolarizing NMBDs? 6. How does the mechanism of action of sugammadex differ from neostigmine, when used to antagonize nondepolarizing NMBD activity?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}