evacuation of hematoma • Patient in sitting / head raised position • Have equipment ready for difficult airway and have a variety of ETT sizes • Prep and drape neck prior to securing airway (for emergent decompression and surgical airway) • Maintain spontaneous ventilation and avoid muscle relaxants • Intubation by most experienced anesthesiologist
patient meets standard extubation criteria and has adequate cuff leak • Consider laryngoscopy to directly visualize presence/absence of airway edema • Dexamethasone to reduce airway edema • If extubating, avoid bucking movements • PONV prophylaxis is encouraged
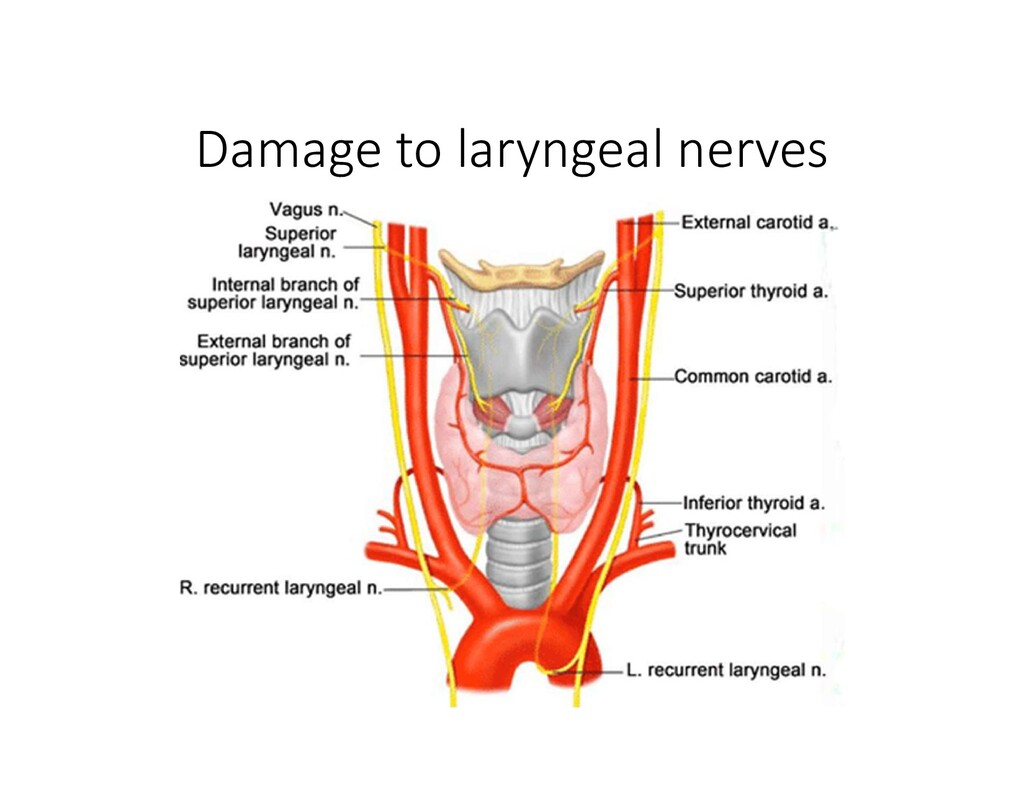
the most common nerve injury after thyroidectomy • Risk factors for RLN injury after thyroidectomy: • Thyroid cancer, total thyroidectomy, re-operation for recurrent goiter, not identifying the RLN • Cardiovocal syndrome (Ortner’s syndrome) • Mitral stenosis -> LA dilation -> compression of L RLN • Left RLN nerve palsy can also be caused by thoracic aortic aneurysms, pulmonary HTN, or enlarged pulm A.
after thyroidectomy • Timing • Signs of hypocalcemia typically do not appear until 24- 72hrs post-op, however, they can appear as early as 1- 3hrs post-op • Laryngeal muscles are very sensitive to hypocalcemia • Stridor -> laryngospasm may be first sign of surgically induced hypoparathyroidism
on trachea by goiter • Prolonged pressure may cause atrophy and erosion of cartilaginous tracheal rings • Leads to tracheal collapse and airway obstruction • May necessitate reintubation
of an Expanding Neck Hematoma in the PACU”. EC Anaesthesia 5.12s (2019): 37-44. • Bajwa SJ, Sehgal V. Anesthesia and thyroid surgery: The never ending challenges. Indian J Endocrinol Metab. 2013;17(2):228-234. • Zakaria HM, Al Awad NA, Al Kreedes AS, et al. Recurrent laryngeal nerve injury in thyroid surgery. Oman Med J. 2011;26(1):34-38. doi:10.5001/omj.2011.09 • Dixon JL, et al. A novel method for the management of post- thyroidectomy or parathyroidectomy hematoma: a single-institution experience after over 4,000 central neck operations. World J Surg. 2014;38(6):1262-1267. • Miller, Ronald D. Miller's Anesthesia. 7th ed. Philadelphia, PA: Churchill Livingstone/Elsevier, 2010.14;38(6):207-211 & 443-445 • Michael Goldenberg, Sonia Vaida. Anesthetic Management of Post- Thyroidectomy Complications. Anesthesiology News: Clinical Anesthesiology. 2019. Accessed online 5/2020. • Truong A, Truong DT (2011) Vocal Cord Dysfunction: An Updated Review. Otolaryngol S1:002. Doi: 10.4172/2161-119X.S1-002
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}