anesthetic practice • Develop simple strategies to minimize pollution and waste that anyone can do • Provide an overview of low flow anesthesia • Increase awareness of current and future technologies which may reduce environmental impact Black Canyon of the Gunnison National Park, Montrose, Colorado
America (2014) • US hospitals vs European hospitals • Chemical purchasing • 10% of total US greenhouse gas emissions Image: https://levohealth.com/wp-content/uploads/2018/12/levo-health-why- is-healthcare-marketing-important-1-1200x801.jpg
US lacks comprehensive Climate Control Legislature • The Department for Human Health and Services offers little guidance on ecological practice • Few policy-derived financial or other incentives to be responsible • Immense pressure towards single-use and wasteful products Images: https://static.grainger.com/rp/s/is/image/Grainger/1TTV5_AS01?$mdmain$ https://www.teleflex.com/usa/product-areas/anesthesia/airway-management/laryngoscopes /single-use-laryngoscopes/Polaris-MAC3_DispoLED_-4153130_Left.jpg
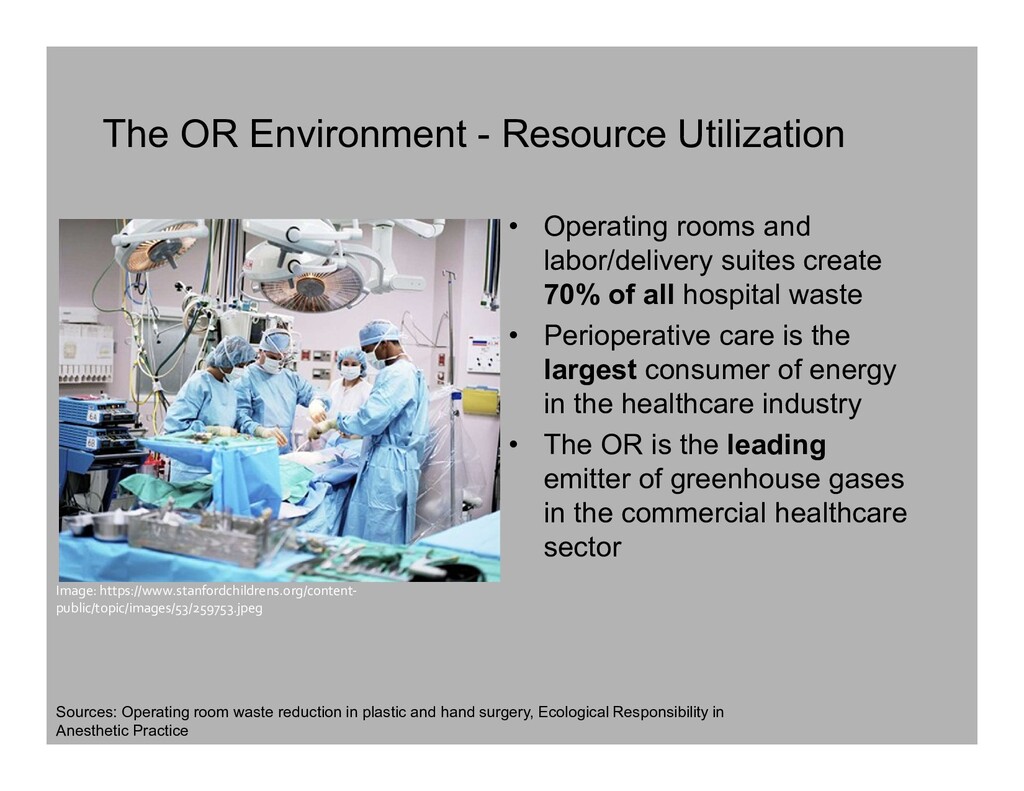
labor/delivery suites create 70% of all hospital waste • Perioperative care is the largest consumer of energy in the healthcare industry • The OR is the leading emitter of greenhouse gases in the commercial healthcare sector Image: https://www.stanfordchildrens.org/content- public/topic/images/53/259753.jpeg Sources: Operating room waste reduction in plastic and hand surgery, Ecological Responsibility in Anesthetic Practice
On average: • ~60% of a hospital’s revenue • 40-60% of an organization’s supply costs • 30% of a facility’s waste, and 66% of regulated medical waste • 3-6x more energy per ft2 than elsewhere in the facility Hocking Hills, Logan, OH
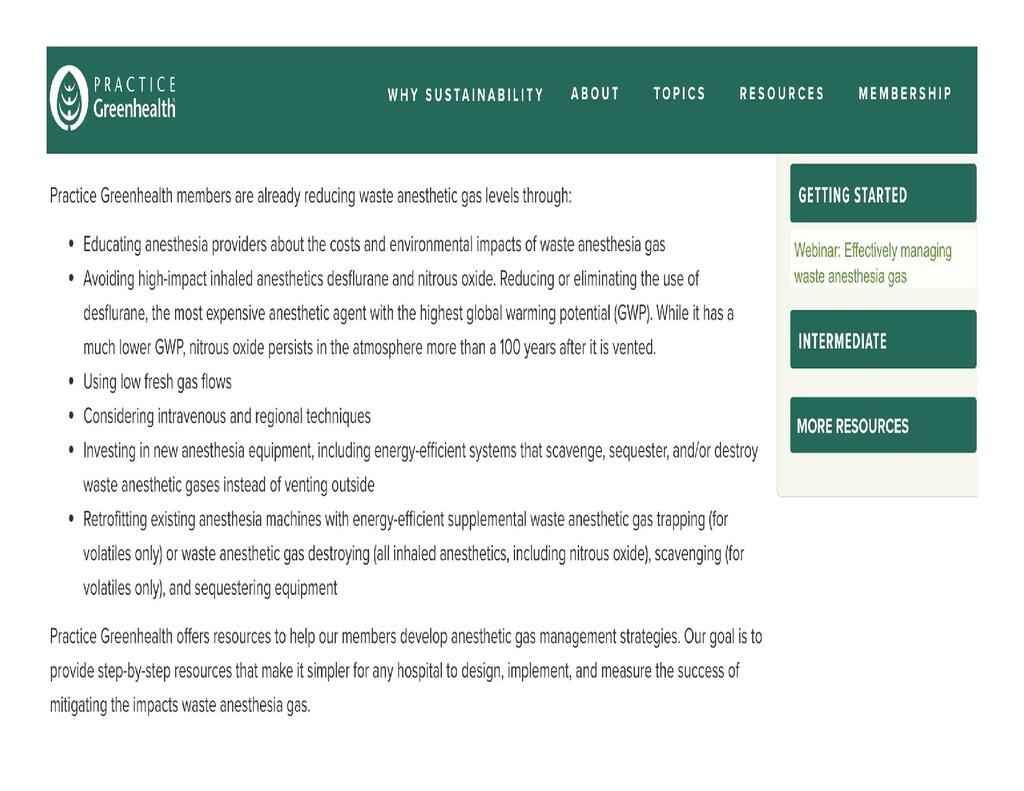
Hospital saves nearly $240,000 annually by making sure anesthesiologists are aware of the environmental impact of vented anesthetic gases. https://practicegreenhealth.org/topics/greening-operating- room/anesthetic-gas Narvik Fjord, Norway
and leadership. It may be appropriate for anesthesiologists to take the lead in focusing health care systems on environmentally sustainable practices.” – Sherman. Ecological Responsibility in Anesthesia Practice. International Anesthesiology Clinics. 2010;48(3):139-151. Lower Calf Creek Falls, Escalante, Utah
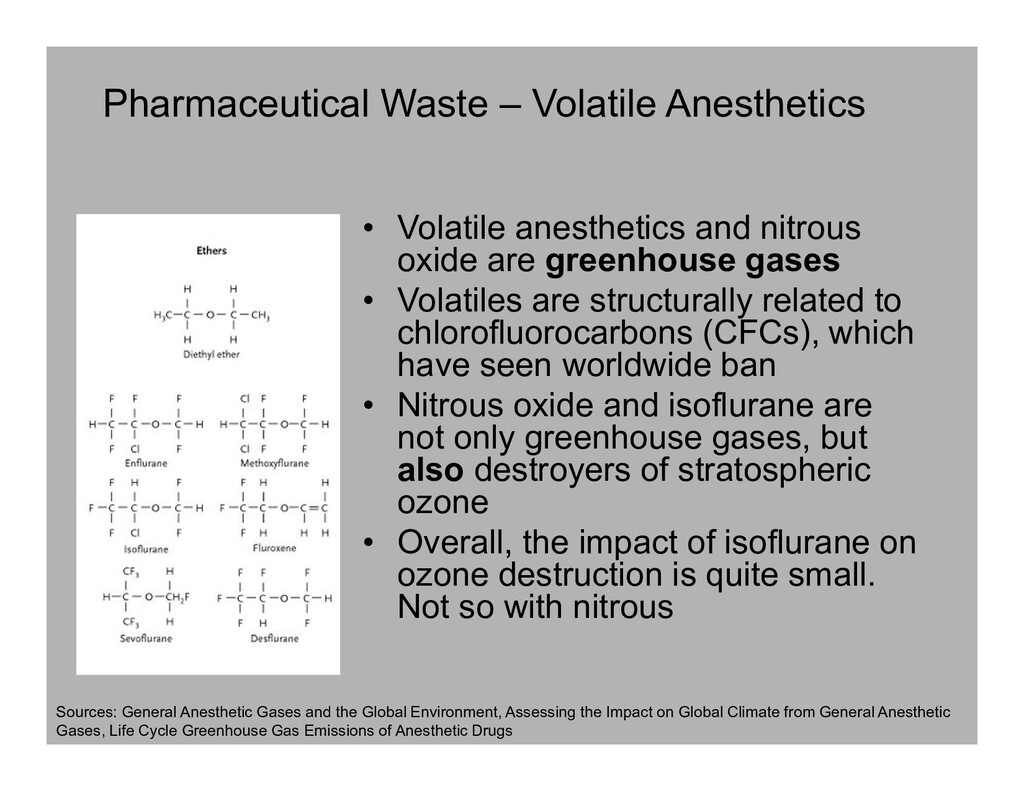
oxide are greenhouse gases • Volatiles are structurally related to chlorofluorocarbons (CFCs), which have seen worldwide ban • Nitrous oxide and isoflurane are not only greenhouse gases, but also destroyers of stratospheric ozone • Overall, the impact of isoflurane on ozone destruction is quite small. Not so with nitrous Sources: General Anesthetic Gases and the Global Environment, Assessing the Impact on Global Climate from General Anesthetic Gases, Life Cycle Greenhouse Gas Emissions of Anesthetic Drugs
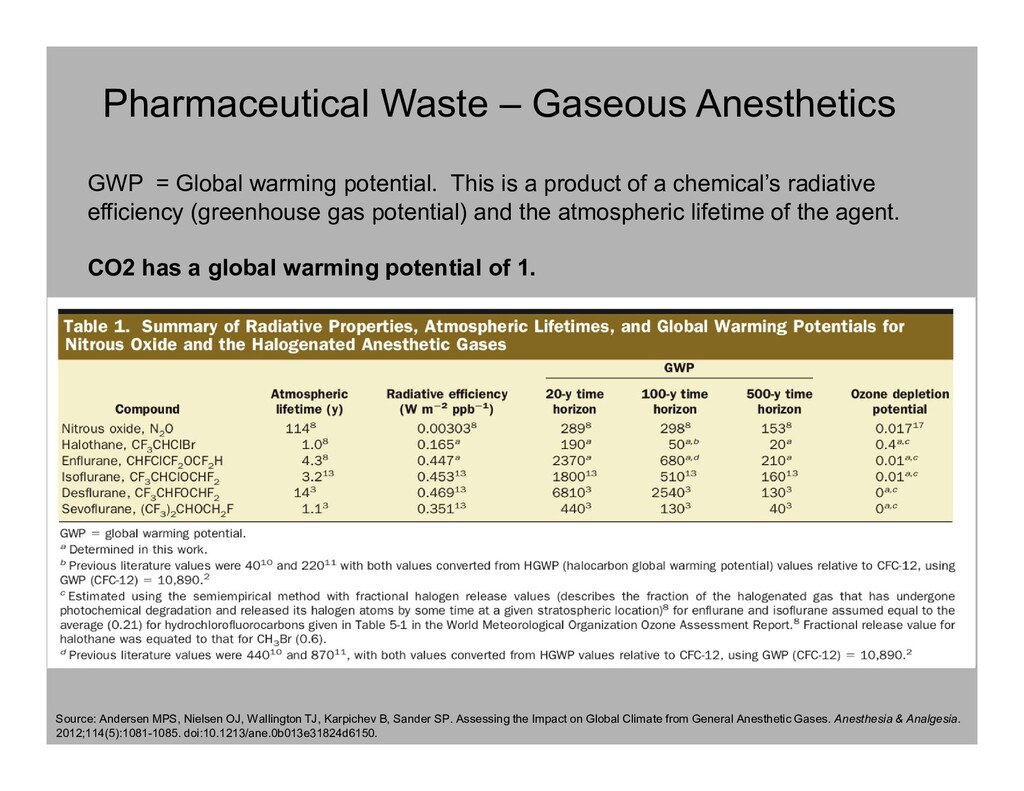
Wallington TJ, Karpichev B, Sander SP. Assessing the Impact on Global Climate from General Anesthetic Gases. Anesthesia & Analgesia. 2012;114(5):1081-1085. doi:10.1213/ane.0b013e31824d6150. GWP = Global warming potential. This is a product of a chemical’s radiative efficiency (greenhouse gas potential) and the atmospheric lifetime of the agent. CO2 has a global warming potential of 1.
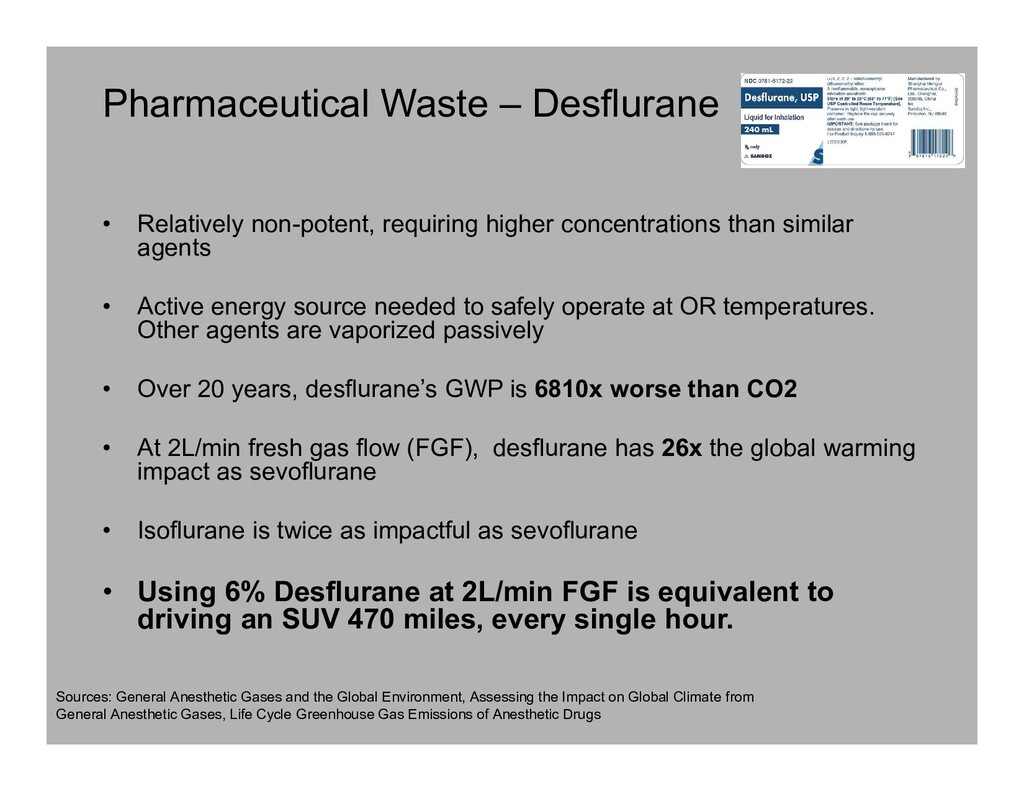
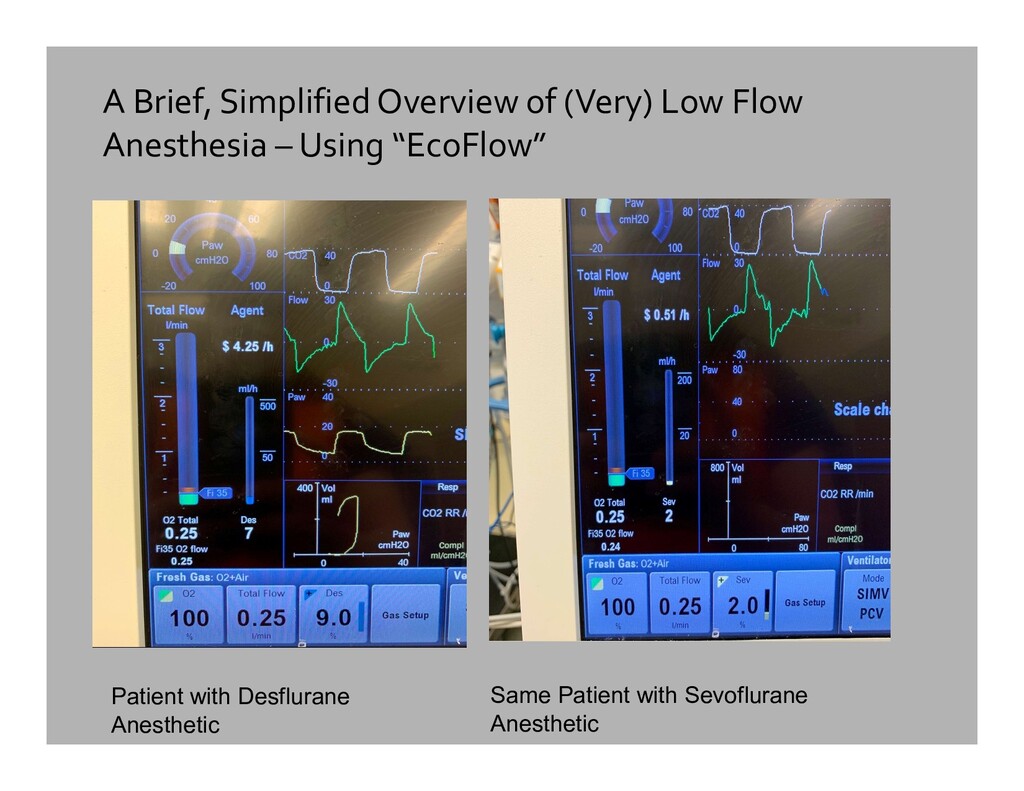
than similar agents • Active energy source needed to safely operate at OR temperatures. Other agents are vaporized passively • Over 20 years, desflurane’s GWP is 6810x worse than CO2 • At 2L/min fresh gas flow (FGF), desflurane has 26x the global warming impact as sevoflurane • Isoflurane is twice as impactful as sevoflurane • Using 6% Desflurane at 2L/min FGF is equivalent to driving an SUV 470 miles, every single hour. Sources: General Anesthetic Gases and the Global Environment, Assessing the Impact on Global Climate from General Anesthetic Gases, Life Cycle Greenhouse Gas Emissions of Anesthetic Drugs
most widely used inhaled anesthetic worldwide • Used at high concentrations due to high MAC • Both a greenhouse gas and ozone depleter • Long-stable half life in the atmosphere of >100 years • The addition of 60% nitrous oxide to sevoflurane or isoflurane to equal 1 MAC worsens the impact of sevoflurane 6-fold, and isoflurane 3-fold • One MAC of Nitrous/Desflurane has a GWP nearly equivalent to desflurane alone. Thus no ecological benefit Sources: General Anesthetic Gases and the Global Environment, Assessing the Impact on Global Climate from General Anesthetic Gases, Life Cycle Greenhouse Gas Emissions of Anesthetic Drugs
that of CO2 • N2O widely used in dental offices, L+D suites, and Operating Rooms • N2O, CO2 , and Methane are the 3 most important long-lived gases among all addressed by the Kyoto Protocol Sources: General Anesthetic Gases and the Global Environment, Assessing the Impact on Global Climate from General Anesthetic Gases, Life Cycle Greenhouse Gas Emissions of Anesthetic Drugs Arches National Park, Moab, Utah
• WAGD lines are just another “vacuum line”. They exhaust to the atmosphere • There is usually no recirculation, scavenging, filtering, or recycling unless additional systems are installed • All fresh gas flow and exhaled “stale” gas containing volatile anesthetics leave the hospital unchanged Why have a WAGD line? Theoretical over sharing a suction line for waste anesthetics: - No compromise of suctioning power - Theoretically lower risk of fire than a shared surgical suction system (per the manufacturer) Source: https://beaconmedaes.com/index.php?option=com_co ntent&view=article&id=56&Itemid=67S
hazard • Does not degrade, accumulates in fat, toxic to aquatic life, requires incineration to be destroyed • Incineration releases dioxins, CO2, and harmful carbon derivatives • 50-60% of all propofol goes unused and wasted • Propofol is the most widely wasted pharmaceutical in the OR • However, the overall environmental footprint of propofol is ~10,000 times less than desflurane Source: Propofol wastage in anesthesia
waste/ year (2014) • 85% of this waste is unregulated and enters public waste stream • $40.3 billion/year spent on disposing medical waste • Over 90% of “red bag waste” found to be uncontaminated • Sharps bins typically contain ~50% non-sharps by volume Sources: Operating room waste reduction in plastic and hand surgery, Medical Waste in the Environment, Environmental Impacts of Surgical Procedures Image: https://ehs.stanford.edu/wp-content/uploads/Biohazard-Waste-Bag-in-a-Hard-Sided-Leak-Proof-Container.jpg
• Ambu bag • Syringes • Volatile anesthetic bottles • Oral airways • Central line/arterial line/neuraxial kits • Atomizers • Exterior wrappers • Albuterol adapters • Etc…. Image: https://ichef.bbci.co.uk/news/624/cpsprodpb/BAA6/production/ _103528774_plastic_explained_v4_640-nc.png Most medical plastic is not labeled with a recyclable symbol. One study found <20% of items had an ID symbol. Source: Managing barriers to recycling in the operating room
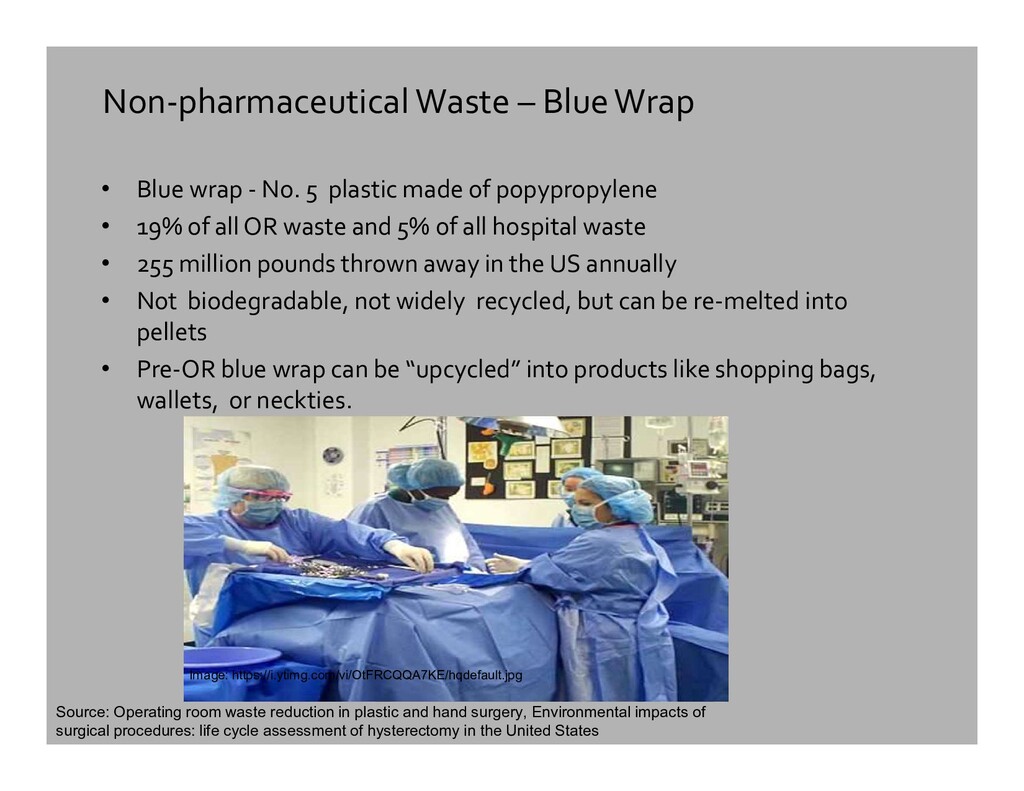
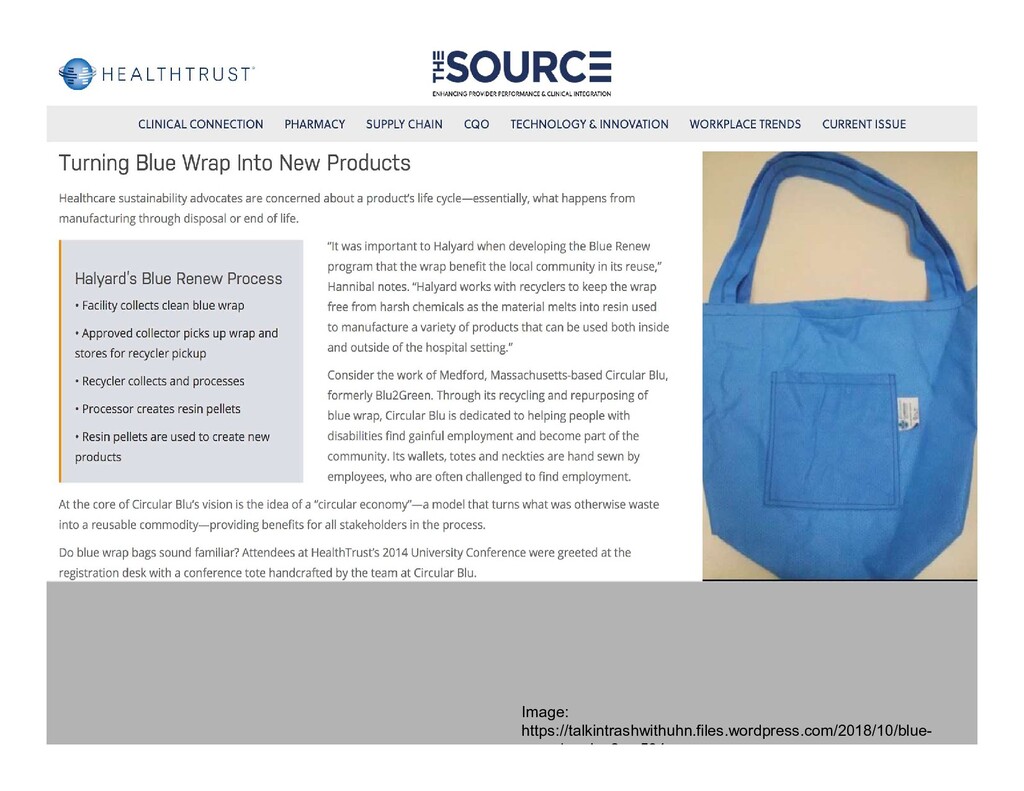
5 plastic made of popypropylene • 19% of all OR waste and 5% of all hospital waste • 255 million pounds thrown away in the US annually • Not biodegradable, not widely recycled, but can be re-melted into pellets • Pre-OR blue wrap can be “upcycled” into products like shopping bags, wallets, or neckties. Image: https://i.ytimg.com/vi/OtFRCQQA7KE/hqdefault.jpg Source: Operating room waste reduction in plastic and hand surgery, Environmental impacts of surgical procedures: life cycle assessment of hysterectomy in the United States
at 4 campuses • 524 participants • 56.7% reported being unclear which OR items are recyclable • 47.7% thought the greatest barrier to recycling was knowledge • After implementing a robust recycling and education program, a cost savings of 10.3% was achieved in sharps waste disposal alone
Impact, Environmentally and Financially: Source: Environmental impacts of surgical procedures: life cycle assessment of hysterectomy in the United State
those who have not attended this lecture, including perioperative staff • Encourage more TIVA, balanced IV/volatile anesthetics, and regional anesthetics (spinal, epidural, PNB+sedation) • Limit nitrous use to the “second gas effect”. Induction/emergence only • Substantially limit or eliminate desflurane vaporizers from ORs • Limit desflurane indications only to bariatric cases/morbidly obese patients • Encourage using smaller size vials or “compounded” drug syringes to reduce drug waste. • More recycle bins, more signs, more education • Sort plastic waste for recycling: breathing circuits, empty syringes, blue wrap • Eliminate unneeded items from custom line and block kits
– Hackensack – 7 consecutive years of awards for green initiatives, including sustainable food purchasing. • Hackensack Meridan – Jersey Shore – Commitment to sustainable energy acquisition, reduction in serving meat. • Overlook Medical Center – comprehensive blue wrap recycling program • Boston Medical Center – created a co-generation power plant which provides 43% of the hospital’s electric needs, saves $1.5 million per year, and can provide heat and electricity during a disaster. Bold goal of becoming carbon neutral by the end of 2020. • Cleveland Clinic – Sourced 30% of their food locally and sustainably. Saved more than $4m in 2017 through “Greening the OR strategies”
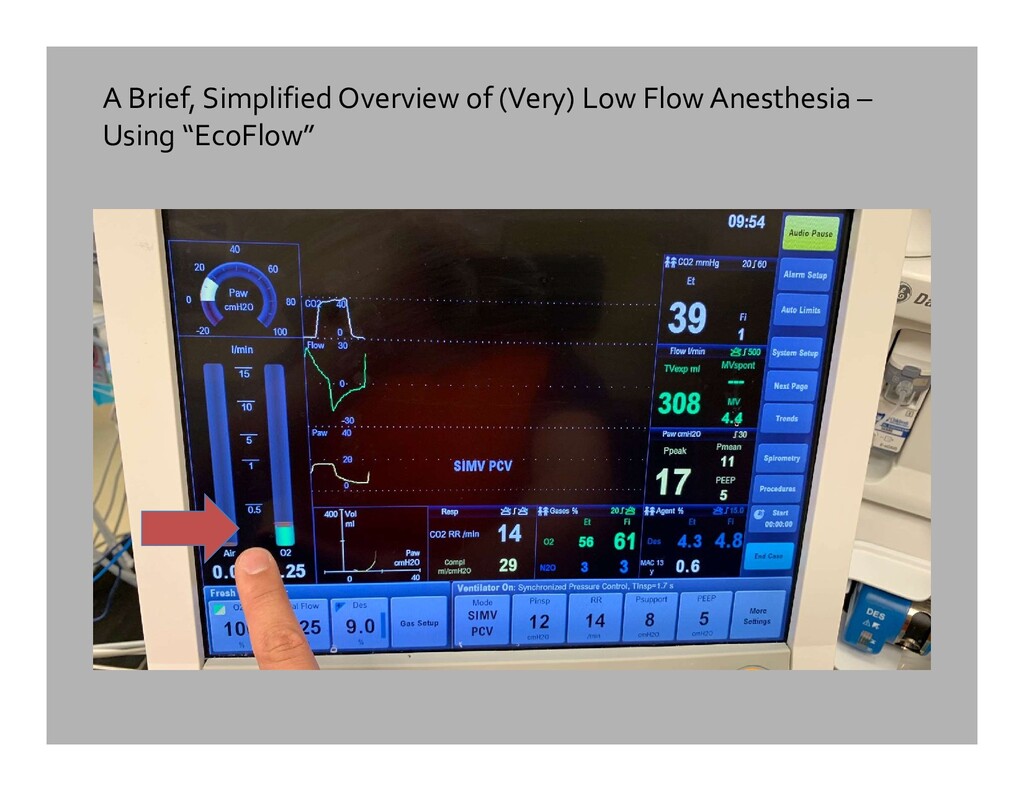
leaky endotracheal tubes • Must increase flows to quickly change volatile concentration (like briefly increasing IV drip rate to give a medication) • Delivered anesthetic concentrations will differ from what was “dialed in”. Passive vaporizers are inaccurate at very low and very high flows. • Minimum fresh O2 needed is about 250 ml/min in adults (10 ml/kg3/4). • Minimum fresh O2 is 14ml/kg3/4 if patient under 20kg. Source: Size DOES Matter: A Calculation of Differences Between Children and Adults.
in plastic and hand surgery. Plastic Surgery. 2015;23(4). doi:10.4172/plastic-surgery.1000941. • Andersen MPS, Nielsen OJ, Wallington TJ, Karpichev B, Sander SP. Assessing the Impact on Global Climate from General Anesthetic Gases. Anesthesia & Analgesia. 2012;114(5):1081-1085. doi:10.1213/ane.0b013e31824d6150. • Azouz S, Boyll P, Swanson M, Castel N, Maffi T, Rebecca AM. Managing barriers to recycling in the operating room. The American Journal of Surgery. 2019;217(4):634-638. doi:10.1016/j.amjsurg.2018.06.020. • Goldberg ME, Vekeman D, Torjman MC, Seltzer JL, Kynes T. Medical Waste in the Environment. Survey of Anesthesiology. 1997;61(4):253. doi:10.1097/00132586-199708000-00065. • Ishizawa Y. General Anesthetic Gases and the Global Environment. Anesthesia & Analgesia. 2011;112(1):213-217. doi:10.1213/ane.0b013e3181fe02c2. • Holzman, RS. Size DOES Matter: A Calculation of Differences Between Children and Adults. Boston Children’s Hospital/Harvard Medical School, 2000. • Mankes RF. Propofol Wastage in Anesthesia. Anesthesia & Analgesia. 2012;114(5):1091-1092. doi:10.1213/ane.0b013e31824ea491. • Ryan S, Sherman J. Sustainable Anesthesia. Anesthesia & Analgesia. 2012;114(5):921-923. doi:10.1213/ane.0b013e31824fcea6. • Sherman J, Le C, Lamers V, Eckelman M. Life Cycle Greenhouse Gas Emissions of Anesthetic Drugs. Anesthesia & Analgesia. 2012;114(5):1086-1090. doi:10.1213/ane.0b013e31824f6940. • Sherman JD, Ryan S. Ecological Responsibility in Anesthesia Practice. International Anesthesiology Clinics. 2010;48(3):139-151. doi:10.1097/aia.0b013e3181ea7587. • Thiel CL, Eckelman M, Guido R, et al. Environmental impacts of surgical procedures: life cycle assessment of hysterectomy in the United States. Environ Sci Technol. 2015;49(3):1779–1786. doi:10.1021/es504719g
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}