the nervous system to sensory or motor stimulation. • EPs reflect the functional integrity of neural pathway in anesthetized patients undergoing surgical procedures that place the nervous system structures in jeopardy. • Somatosensory evoked potentials (SSEPs), brainstem auditory evoked potentials (BAEPs), visual evoked potentials (VEPs), and motor evoked potentials are amongst the different types of interoperative EPs monitored.
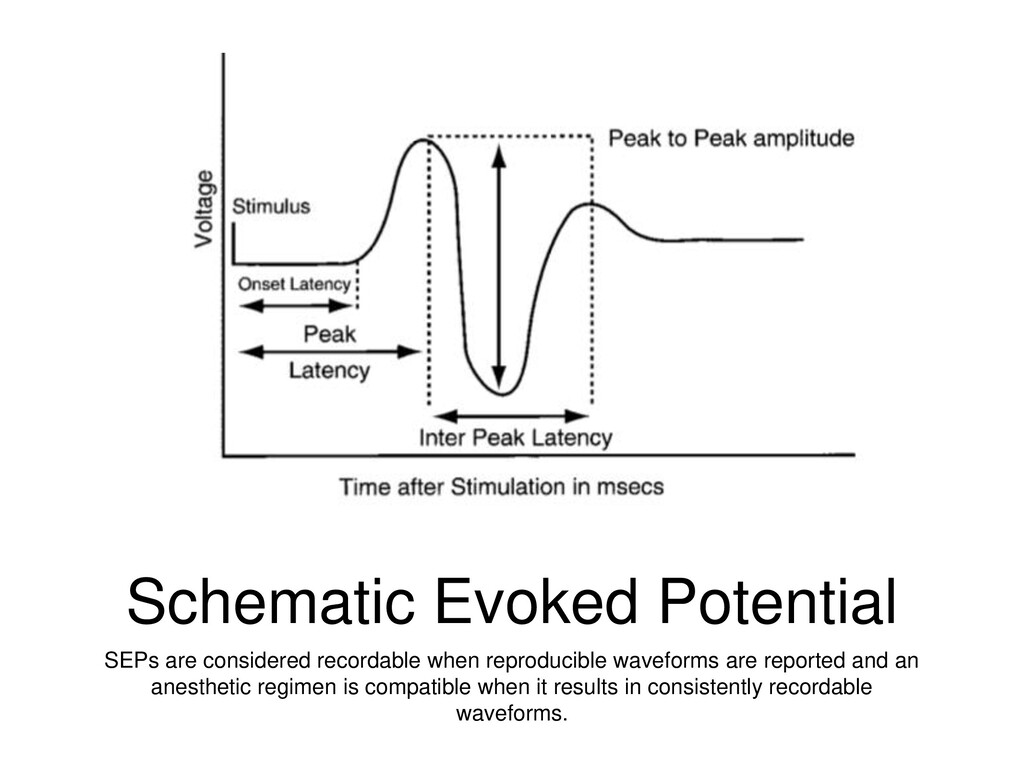
1. Surgical injury 2. Ischemia of specific neural pathway 3. Nonspecific physiologic or pharmacologic influences • Physiological factors: temperature, BP, Hct, acid-base balance, O2 and CO2 tensions • Key terms describing waveforms: amplitude is the waves’ peak to peak voltage difference. latency is time from stimulus to the peak of the response. Inter peak latency is the interval between peaks of interest
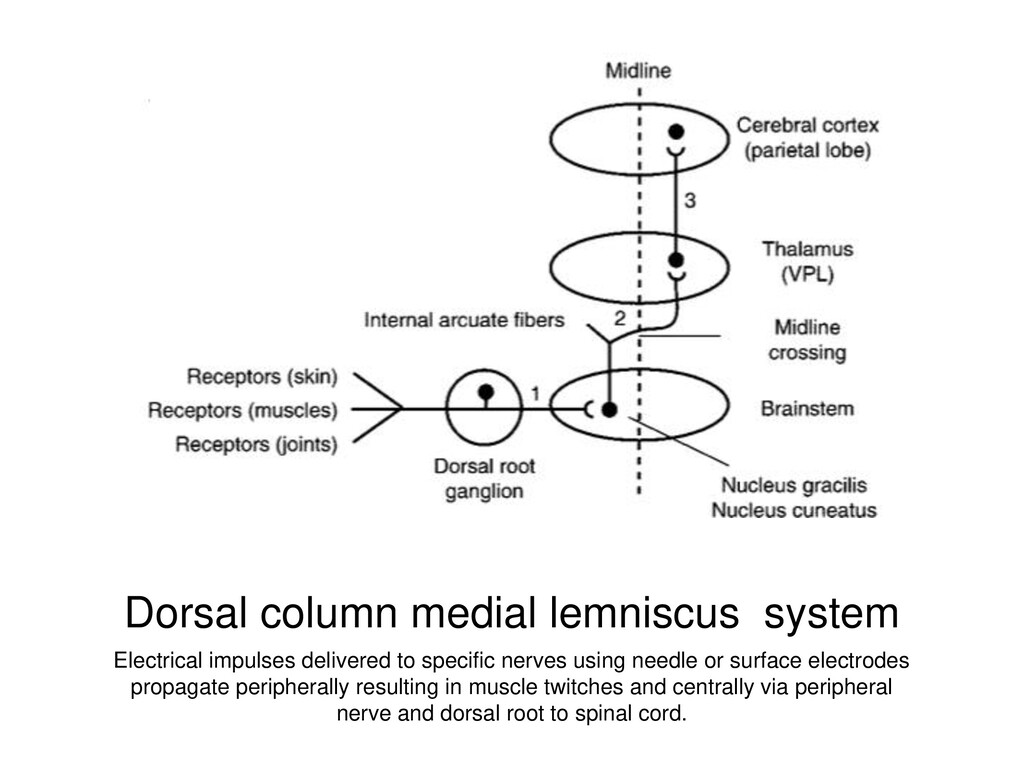
nerves using needle or surface electrodes propagate peripherally resulting in muscle twitches and centrally via peripheral nerve and dorsal root to spinal cord.
fossa after posterior tibial nerve stimulation and at Erb’s point above the clinical after medical nerve stimulation • Spinal potentials recorded over the cervical and lumbar spinous processes confirm the delivery of the stimulus to the central neural axis • Subcortical component of the SSEP is recorded over the second cervical vertebra ** USEFUL intra-op because not very susceptible to anesthetic effects • Cortical SSEPs are corded from the scalp overlying the contralateral primary sensory cortex • What constitutes a significant change? Decrease in amplitude 50% or greater and increase in latency of 10% or greater
effect greater on synaptic transmission than axonal conduction Satisfactory SSEP monitoring possible w/ 0.5-1.0 MAC halothane, enflurane, or isoflurane. Sevo up to 1.5MAC Des up to 1.0 MAC • Nitrous potentiates the depressant effect of volatile anesthetics • Barbituates produce a dose dependent increase in latency and decrease in amplitude • Etomidate dramatically decreases subcortical amplitude up to 50% • Ketamine increase cortical SSEP amplitude as does Etomidate • Propofol effect on SSEP is similar to barbituates. Dose of up to 2.5mg/kg produces no changes in amplitude of cortical and subcortical amplitude • Benzodiazepines have mild to moderate depressant effect with dose 0.2-0.3 mg/kg associated with no reduction in amplitude with slight latency prolongation
changes in SSEP amplitude/latency whether in analgesic or anesthetic doses • Administration of subarachnoid meperidine produced 60% decrease in cortical posterior tibial SSEP amplitude, attributed to local anesthetic like effect of meperidine. • Clonidine and dexmedetomidine affect SSEPs minimally at sedative doses • Regional administration block sensory pathway • Neurmomuscular blockade do not influence SSEP but improve waveform by favorably increasing signal to noise ratio
could be consistently recorded at temps as low at 19 C. This level of hypothermia results in cession of cortical electrical activity • Mild hyperthermia causes SSEP latencies to decrease 5-7% with no change in amplitude • Hypocapnea and Mild Hypoxia to PETO2 of 48 mmHg does not compromise SSEP monitoring but shorten SSEP latency by 2-4% • Hypotension progressively decreases SSEP amplitude without affecting latency.
has been discussed • Practical conclusions that reflect the relative importance of these effects on the ability to reliably monitor neurological pathway during the peri operative period can be deduced
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}