Wood Johnson Medical School Department of Anesthesiology CA-1 Lecture August 5, 2020 Keith P. Lewis, R.Ph., M.D. Professor and Chair Department of Anesthesiology & Perioperative Medicine Rutgers Robert Wood Johnson Medical School
of Washington 1976 “The Pharmacist’s Effect on Digoxin Usage and Toxicity” Keith P. Lewis, University of Rhode Island 1975 Tish Knobf, Ph.D., RN Joseph Bertino, M.D. Ellison “Jeep” Pierce, M.D. PATIENT SAFETY: A LIFETIME PASSION
IHI as “The prevention of harm to patients.” Emphasis is placed on the system of care that (1) prevents errors; (2) learns from errors that do occur; and (3) is built on a culture of safety that includes healthcare professionals, organization, and patients. Institute of Healthcare Improvement
of practices from other high risk agencies has resulted in anesthesiology much safer than 50 years ago • APSF (1985): Non profit corporation with a vision that “no patient shall be harmed by anesthesia” • 6 Sigma Defect Rate: 3.4 defects per million • Mortality Rate: 1/250,000 (2005)
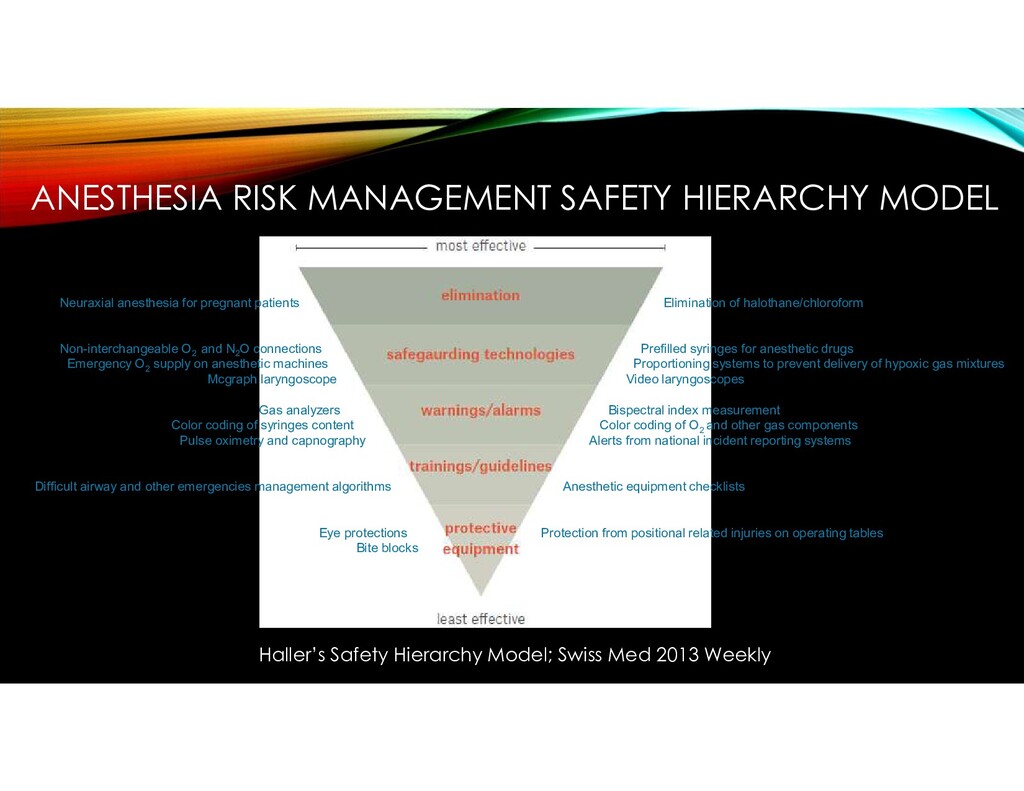
patients Elimination of halothane/chloroform Non-interchangeable O2 and N2 O connections Prefilled syringes for anesthetic drugs Emergency O2 supply on anesthetic machines Proportioning systems to prevent delivery of hypoxic gas mixtures Mcgraph laryngoscope Video laryngoscopes Gas analyzers Bispectral index measurement Color coding of syringes content Color coding of O2 and other gas components Pulse oximetry and capnography Alerts from national incident reporting systems Difficult airway and other emergencies management algorithms Anesthetic equipment checklists Eye protections Protection from positional related injuries on operating tables Bite blocks Haller’s Safety Hierarchy Model; Swiss Med 2013 Weekly
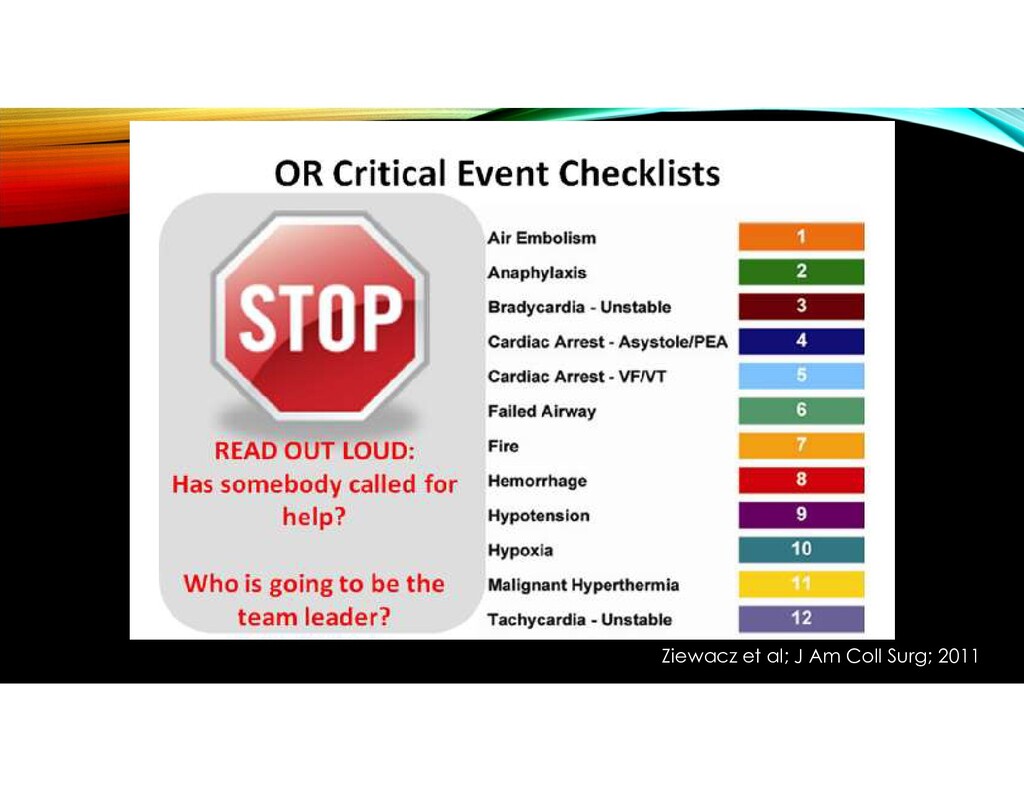
Developed checklists • 12 of the most frequent OR crises • Evidence-based metrics of essential care • Checklists resulted in a 6-fold increase in adherence to critical steps in management • Patient harm persists despite QI and patient safety initiatives J Am Coll Surg 2011;213:212-219, Gawande
• Modern Graphic Design • Interactive Hybrid Publication (Printed & Digital) • Narrated Clinical Vignettes (Based on Real Cases) • QR Code Enabled Videos • Animated Explanations • Safety Pearls at the End of Each Chapter • Slide Sets for Selected Chapters
important addition to the literature on patient safety.” Howard Bauchner, MD Editor in Chief of JAMA and The JAMA Network (2011-) Senior Vice-President, American Medical Association
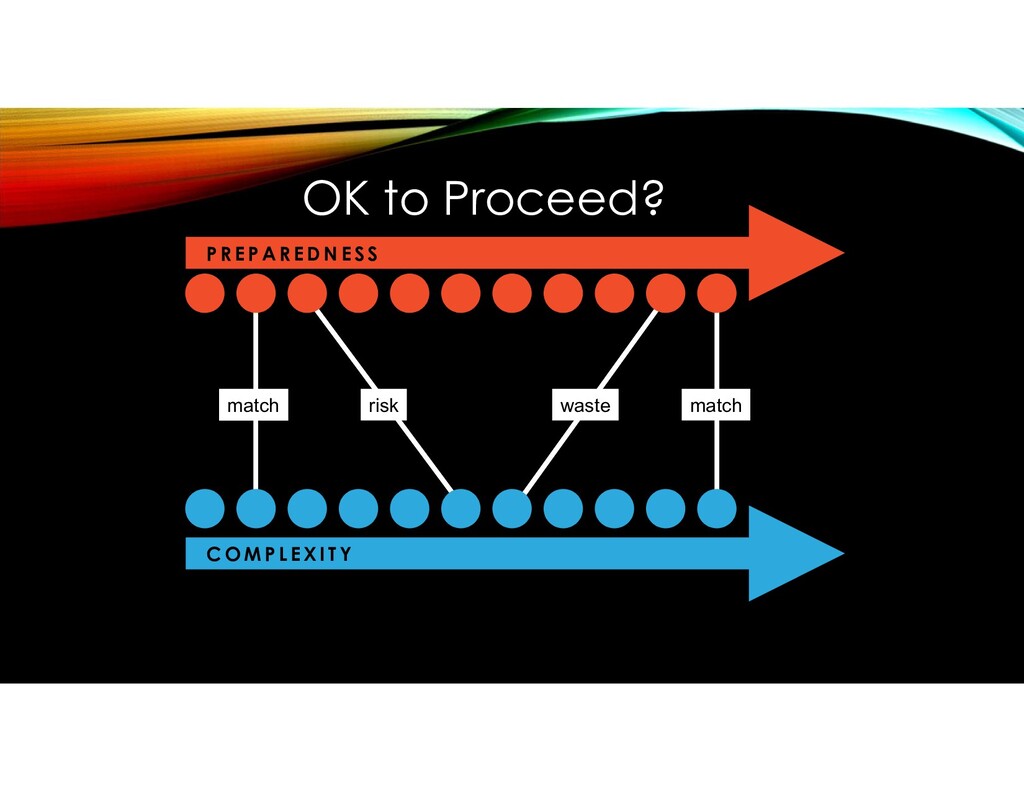
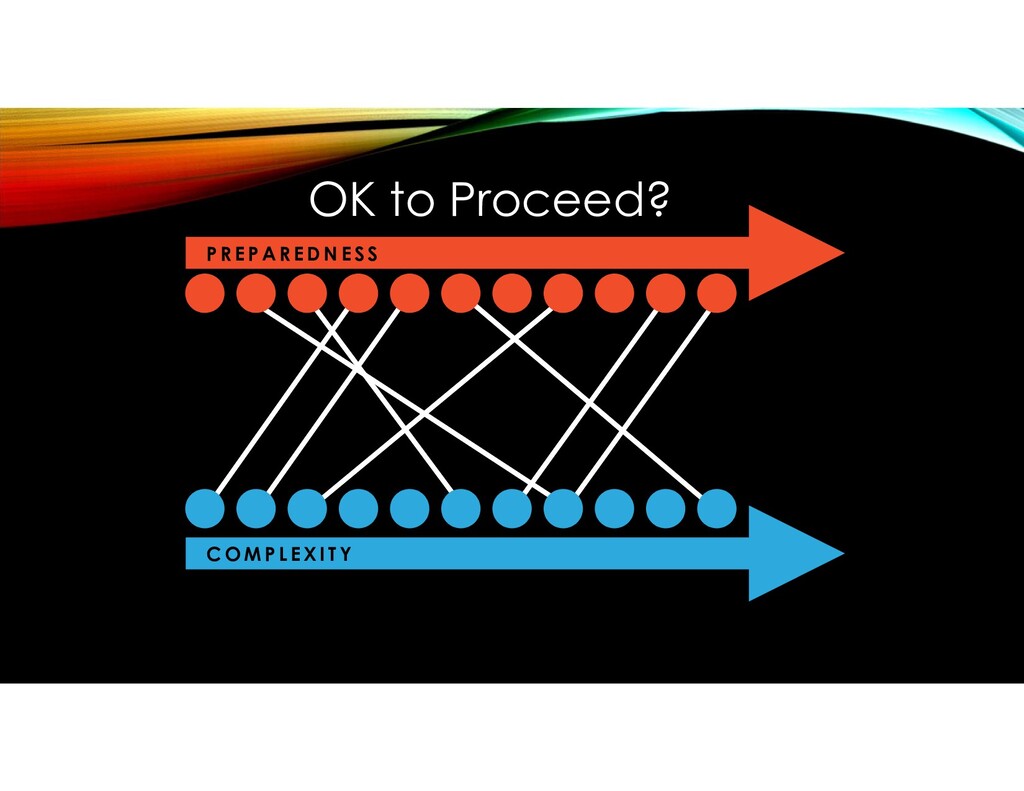
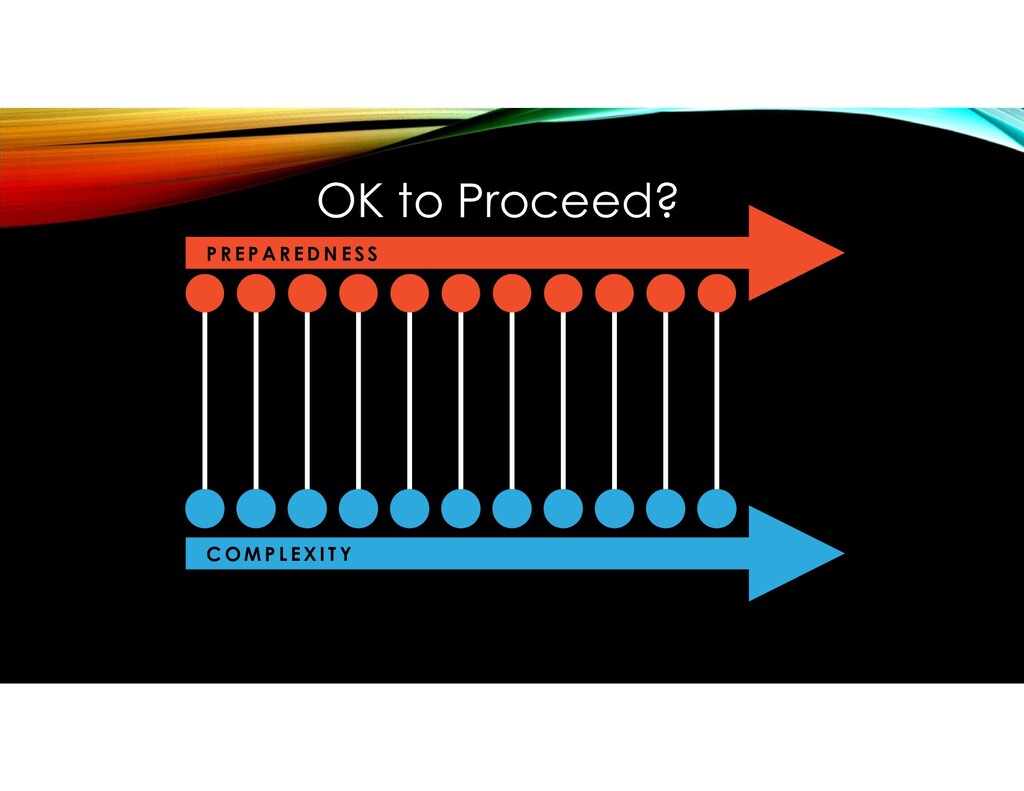
| Melissa Nadler | Pamela Huang 2 Patient Safety: An Intertwined History Rafael Ortega | Orlando Suero 3 The Role of Digital Media in Medical Education Vafa Akhtar-Khavari | Rafael Ortega 4 Making Patient Safety Part of Your Daily Culture James Moses | Scott Friedman 5 The OK to Proceed Model Keith Lewis | Rafael Ortega
Fixation Errors Rafael Ortega 7 Communication Breakdown Robert Canelli | Pamela Huang 8 Medication Errors Kevin Horbowicz 9 Workforce Planning Nancy Gaden | Keith Lewis 10 Fatigue and Sleep Deprivation Jeffrey Schneider | Elizabeth Wallace 11 Physician Burnout David Henderson | Laura Dieppa-Perea | Brandon Newsome 18 Overlapping Procedures Jennifer Tseng | Victoria Race | Gabriel Diaz 19 Noise and Distractions Alik Farber | Steven Pike 20 Social Determinants of Health Thea James | Naillid Felipe 21 Overtreatment William Creevy | Ravin Davidoff 12 The Impaired Practitioner Bobby Chang | Sahitya Puttreddy | Savan Parker 13 Time of the Day James Holsapple 14 Procedural Sedation Christopher Conley | Stephen Schepel 15 Trainees and Procedures Frank Schembri | Aravind Ajakumar Menon 16 Breaches in Infection Control Carol Sulis | Cathy Korn 17 The Proceduralist Ravin Davidoff | Robert DeMayo | Nir Ayalon
Surgical Fires Scharukh Jalisi | Samuel Rubin | Anthony Khalifeh 41 The Difficult Airway Gregory Grillone | Chelsea Troiano | Kevin Wong 42 Pressure Injuries Linda Alexander | Janet Crimlisk | Nancy Gaden 43 Wrong-Site, Wrong-Procedure, Wrong-Patient Errors Eduard Vaynberg | Rachel Achu 44 Retained Surgical Items Jason Hall | Feroze Sidhwa
Katzanek 46 Equipment Sequestration Allison Marshall | Jane Damata 47 Root Cause Analysis Laura Harrington | Allison Marshall 48 Disclosure Angela Jackson | Estela Chen Gonzalez 49 Emotional Support for the Second Victim Scott Friedman 50 The Patient as Our Safety Champion Kate Walsh | Estela Chen Gonzalez 51 The Road Ahead Alastair Bell | Keith Lewis 52 Celebrating Successes Keith Lewis | Robert Canelli | Rafael Ortega
practice…..and another fatal outcome was reported previously, after the anaesthetic team fixated on the patient – a young boy – and his failure to respond to treatment of bronchospasm, instead of checking the equipment, where in fact the problem was located.” Fioratou, Flin, Glavin. No simple fix for fixation errors: cognitive processes and their clinical applications. Anesthesia: 2010: 65(1): 61-69
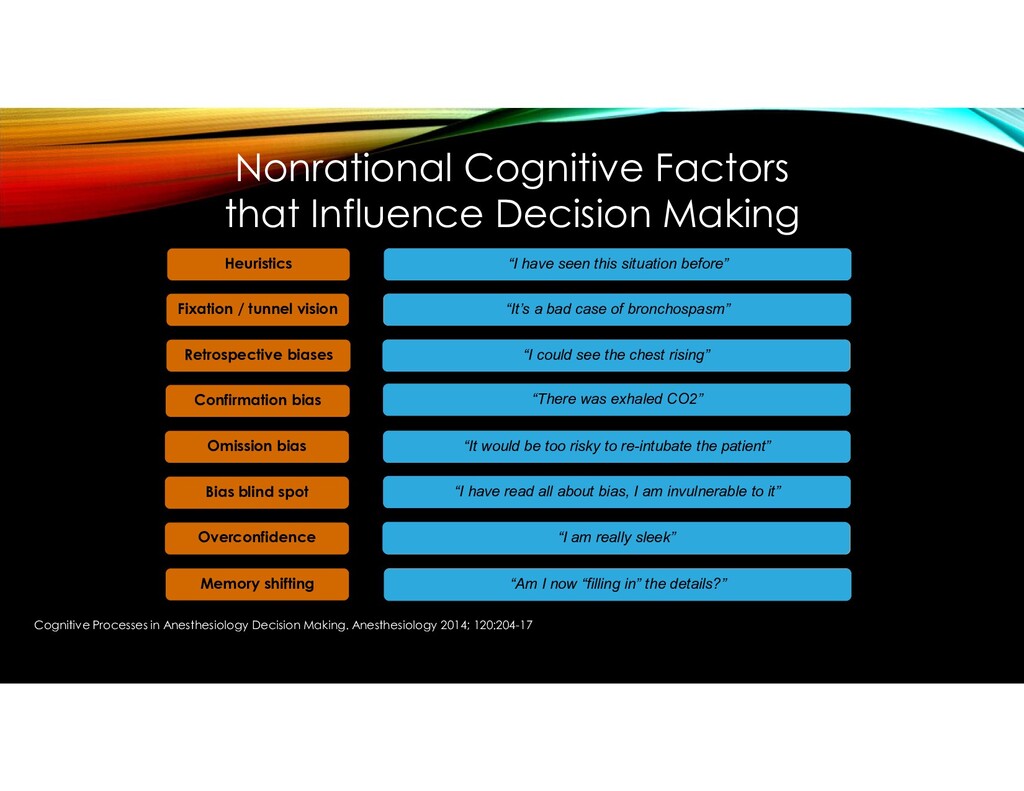
tunnel vision Retrospective biases Confirmation bias Omission bias Bias blind spot Overconfidence Memory shifting Focusing on a single feature, disregarding other aspects Viewing events differently once the outcome is known Seeking information that supports a diagnosis Omission rather than action, out of fear of causing harm Flawed sense of invulnerability to bias High self-assessment with regard to positive traits Failure to accurately recall information “I have seen this situation before” “It’s a bad case of bronchospasm” “I could see the chest rising” “There was exhaled CO2” “It would be too risky to re-intubate the patient” “I have read all about bias, I am invulnerable to it” “I am really sleek” “Am I now “filling in” the details?” Nonrational Cognitive Factors that Influence Decision Making Cognitive Processes in Anesthesiology Decision Making. Anesthesiology 2014; 120:204-17
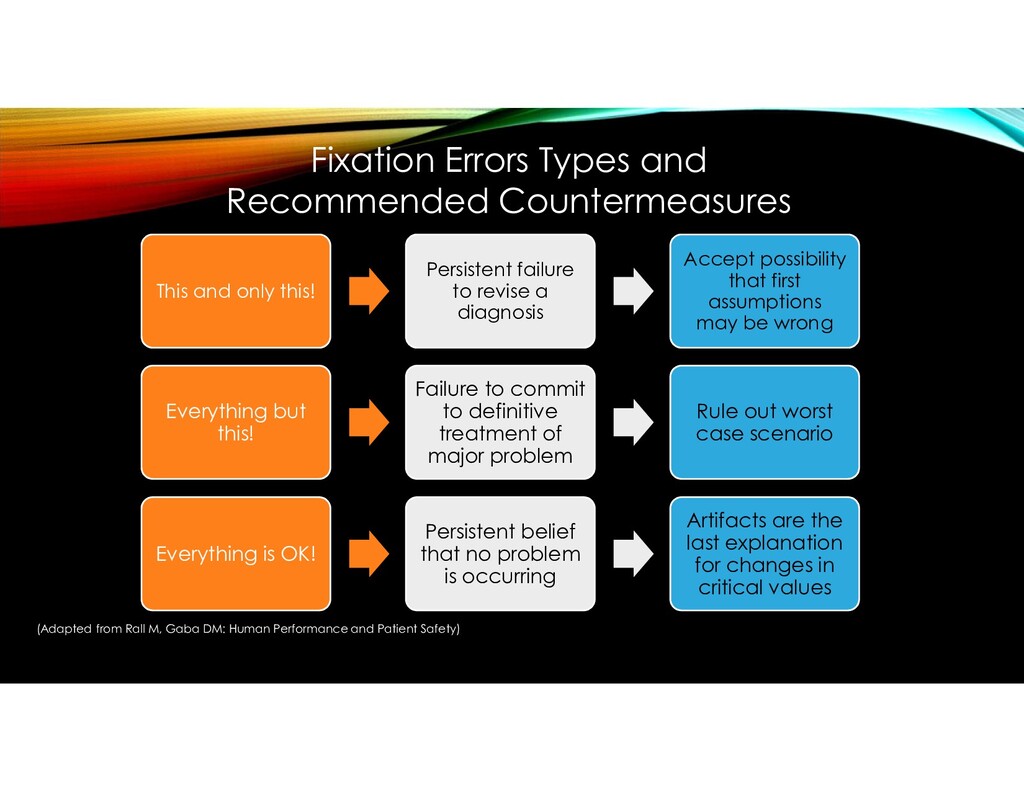
Accept possibility that first assumptions may be wrong Everything but this! Failure to commit to definitive treatment of major problem Rule out worst case scenario Everything is OK! Persistent belief that no problem is occurring Artifacts are the last explanation for changes in critical values Fixation Errors Types and Recommended Countermeasures (Adapted from Rall M, Gaba DM: Human Performance and Patient Safety)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}