for defending the host against infections. However, immune responses are themselves However, immune responses are themselves capable of causing tissue injury and disease.
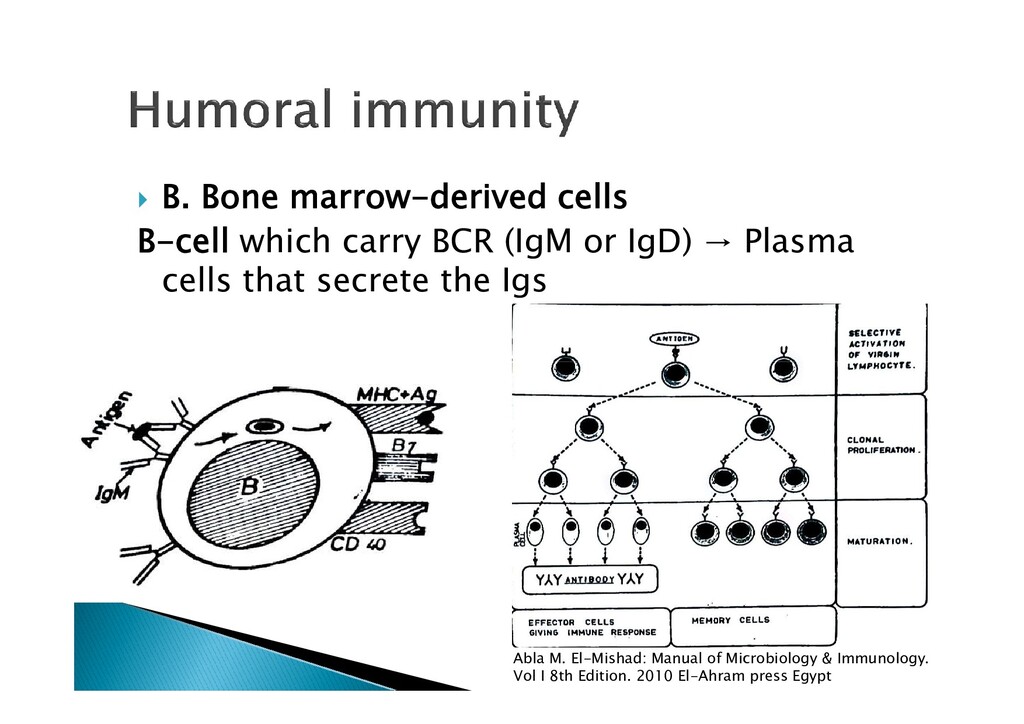
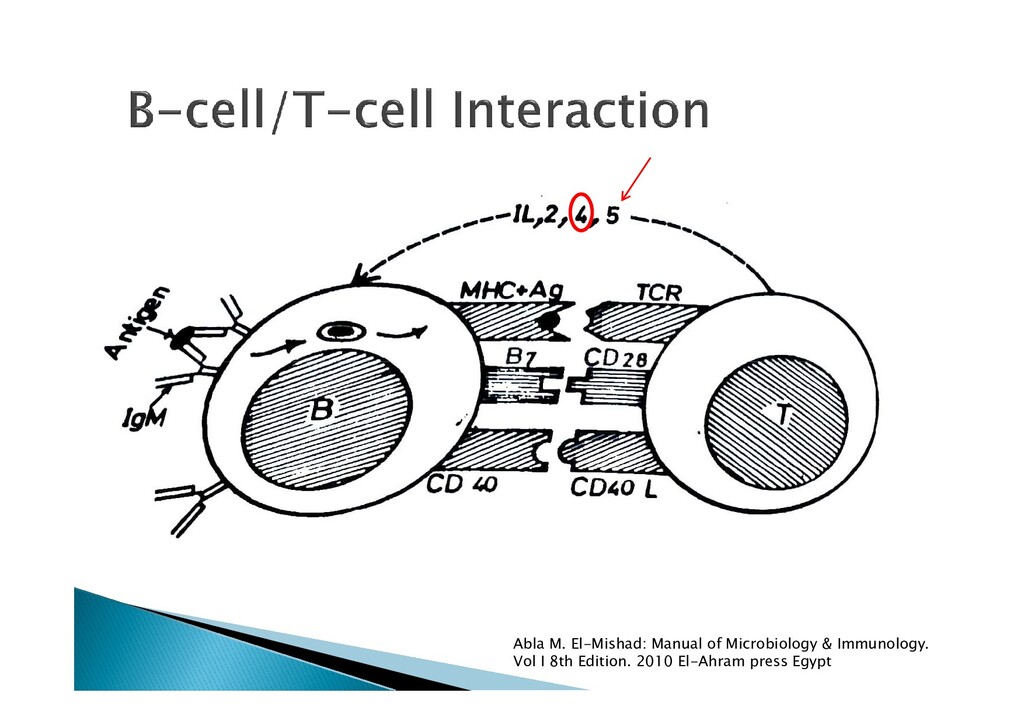
MHC restriction rule (rule of 8). They include TH1, TH2, TH17 and T(reg). They all arise from mother TH0 TH0 2) CD8+ T cells: functionally are also known as cytotoxic T (Tc) Abla M. El-Mishad: Manual of Microbiology & Immunology. Vol I 8th Edition. 2010 El-Ahram press Egypt
mycobacteria, and some parasites. 2. TH2 cells → interleukin (IL)-4, IL-5, IL-13 2. TH2 cells → interleukin (IL)-4, IL-5, IL-13 and also protect against parasitic infections. 3. Tregs (or regulatory T cells) are a subset of T cells that mediate tolerance to both self- antigens and exogenous antigens. Abla M. El-Mishad: Manual of Microbiology & Immunology. Vol I 8th Edition. 2010 El-Ahram press Egypt
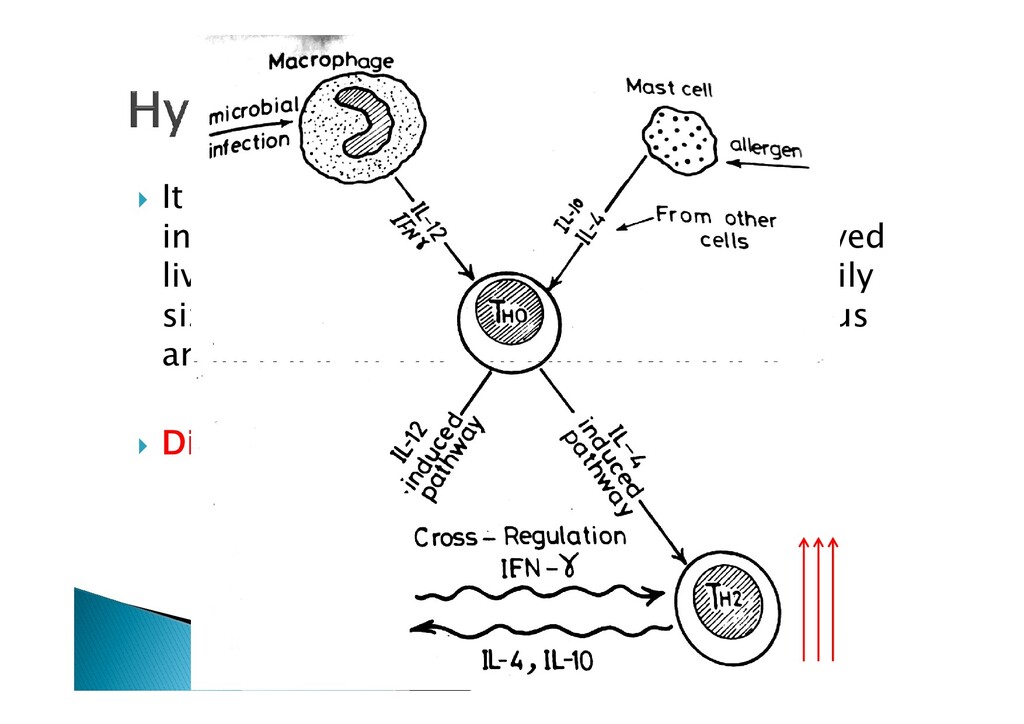
childhood due to improved living standards, hygiene, and smaller family size results in less TH1 stimulation and thus an increase in TH2-mediated diseases. an increase in TH2-mediated diseases. Dirt is good for you!
childhood due to improved living standards, hygiene, and smaller family size results in less TH1 stimulation and thus an increase in TH2-mediated diseases. an increase in TH2-mediated diseases. Dirt is good for you!
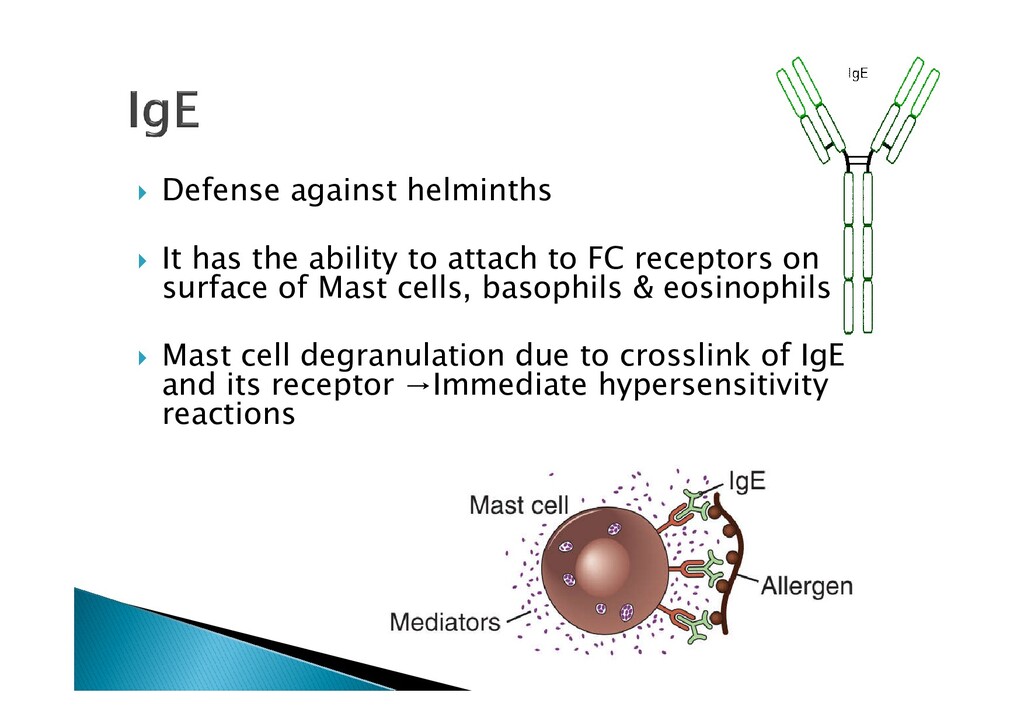
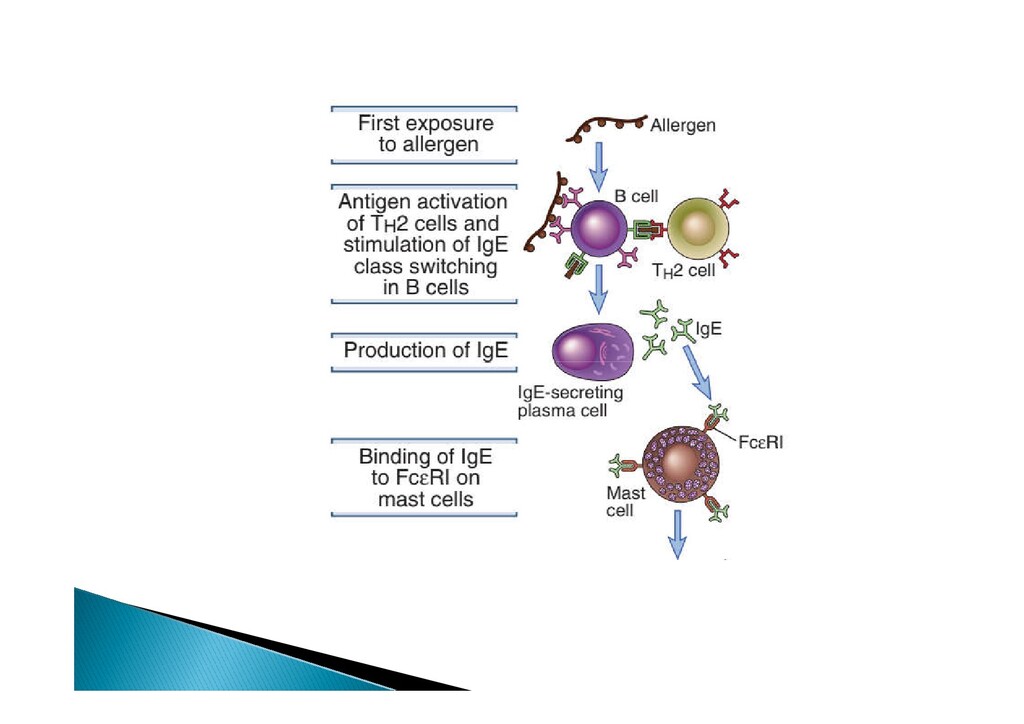
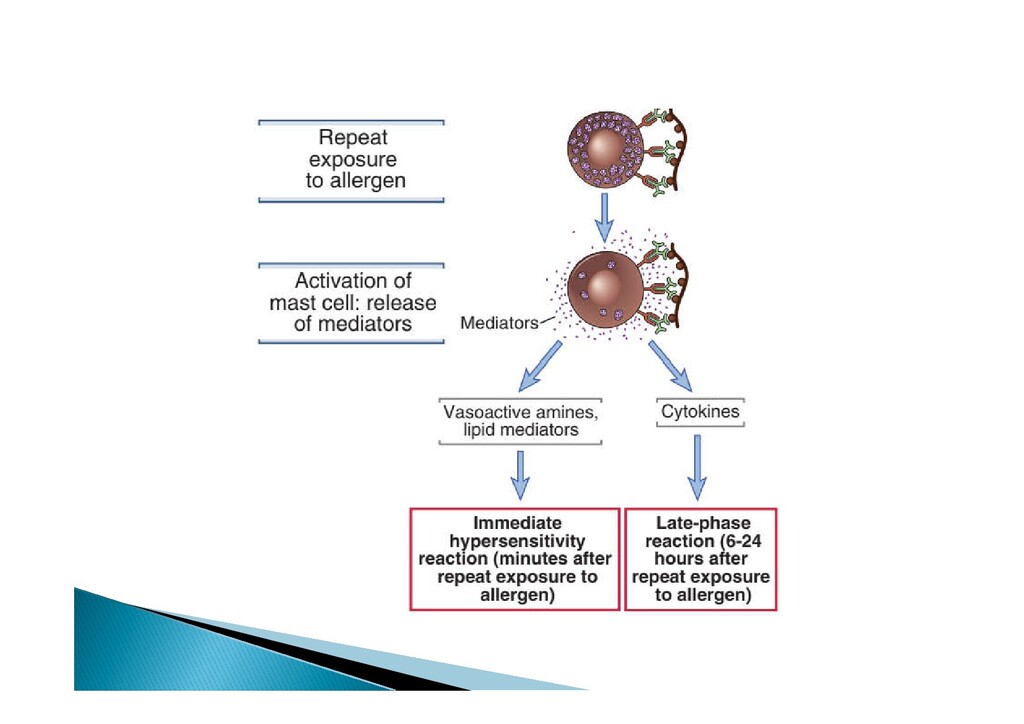
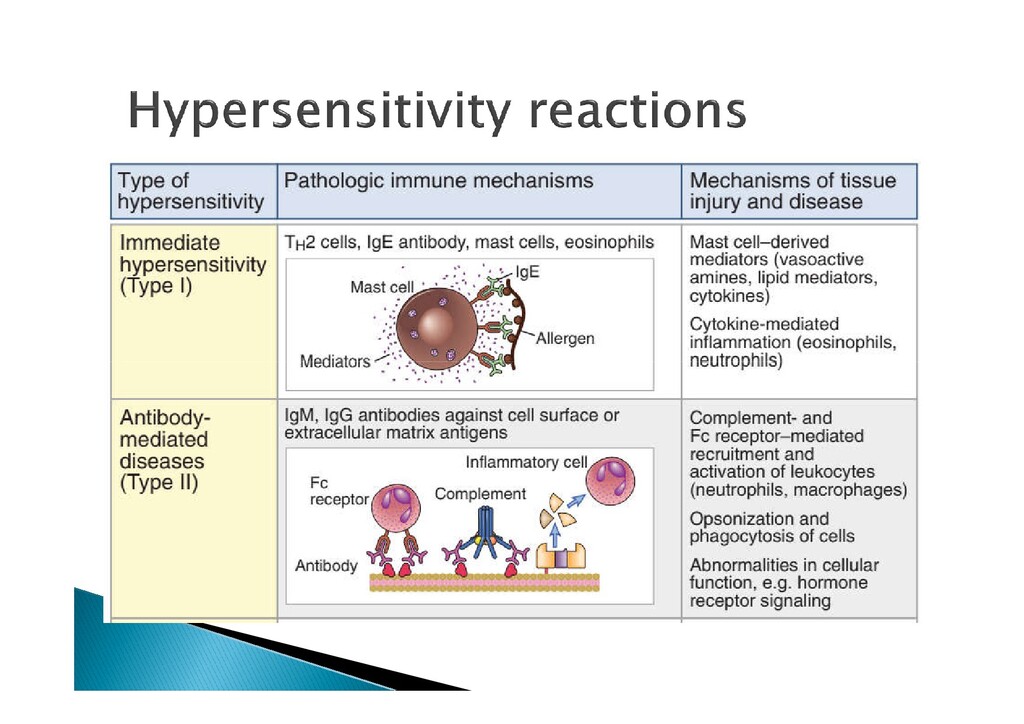
attach to FC receptors on surface of Mast cells, basophils & eosinophils Mast cell degranulation due to crosslink of IgE Mast cell degranulation due to crosslink of IgE and its receptor →Immediate hypersensitivity reactions
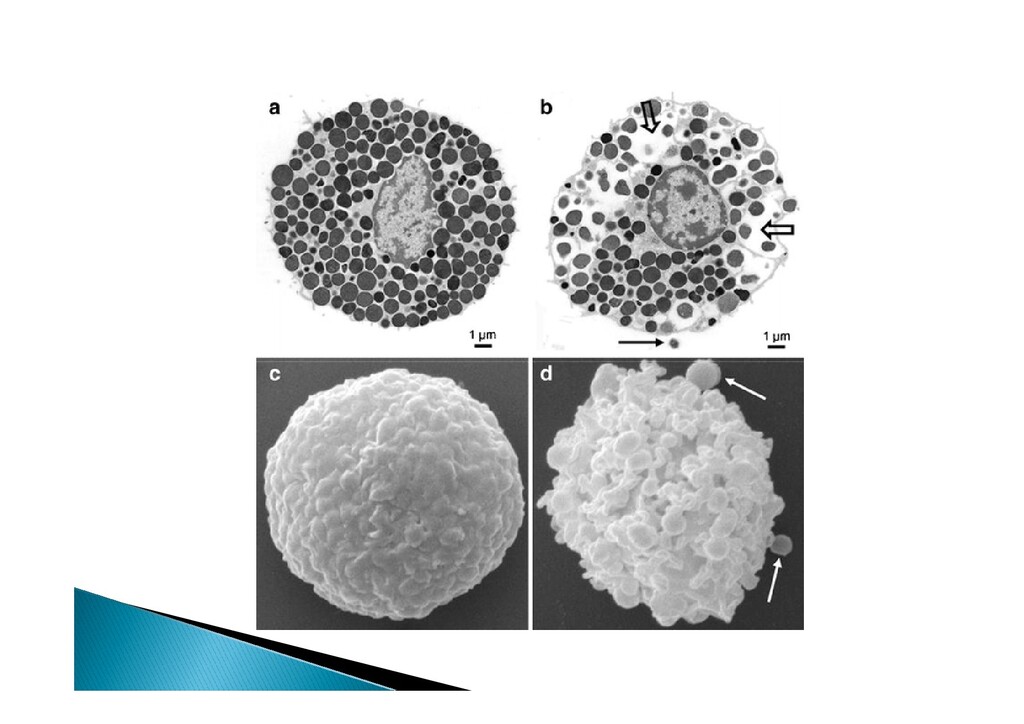
peripheral tissues Full cytoplasmic granules containing acidic proteoglycans that bind to basic dyes. It release many mediators upon activation It release many mediators upon activation and few hours later further mediators being synthesized Many cytokines are also formed: e.g. IL-3, IL- 4, IL-13, IL-5, IL-6 and TNF-α Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
anaphylactic 2. Non IgE mediated pathway = formerly anaphylactoid anaphylactoid Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
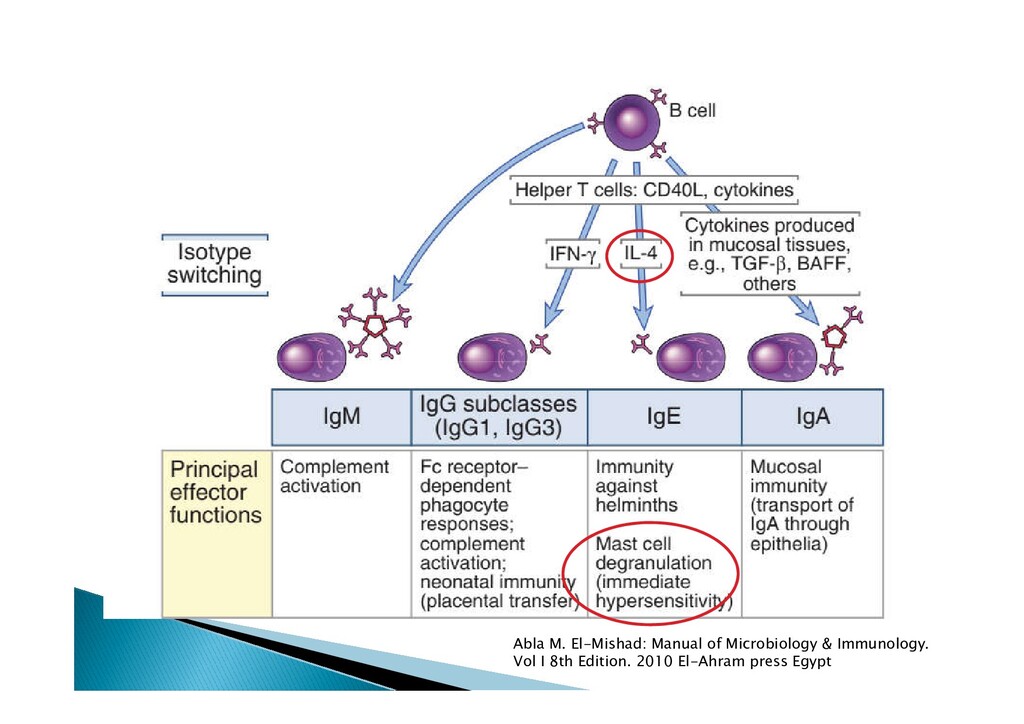
and ↓↓ TH1 Ig Class Switching to IgE which is directed to mast cells, eosinophil that are ready to be armed withem → Immediate type armed withem → Immediate type hypersensitivity. Inhibit other aspects of CMI
Proliferation of B-cells Targeting it show promising results in asthma management. Source: TH2 cells Stimulate mucosal production from respiratory epithelium. Play a role in BA
proteins commonly encountered in a person’s environment. Examples include dust mite, pollen, and Examples include dust mite, pollen, and animal dander. Some chemicals are able to elicit an immune response by binding to self- proteins creating a hapten–carrier conjugate. This is seen in penicillin allergy.
an immune response by itself. It could do only when attached to a large carrier such as a protein. Abla M. El-Mishad: Manual of Microbiology & Immunology. Vol I 8th Edition. 2010 El-Ahram press Egypt
an immune response by itself. It could do only when attached to a large carrier such as a protein. Abla M. El-Mishad: Manual of Microbiology & Immunology. Vol I 8th Edition. 2010 El-Ahram press Egypt
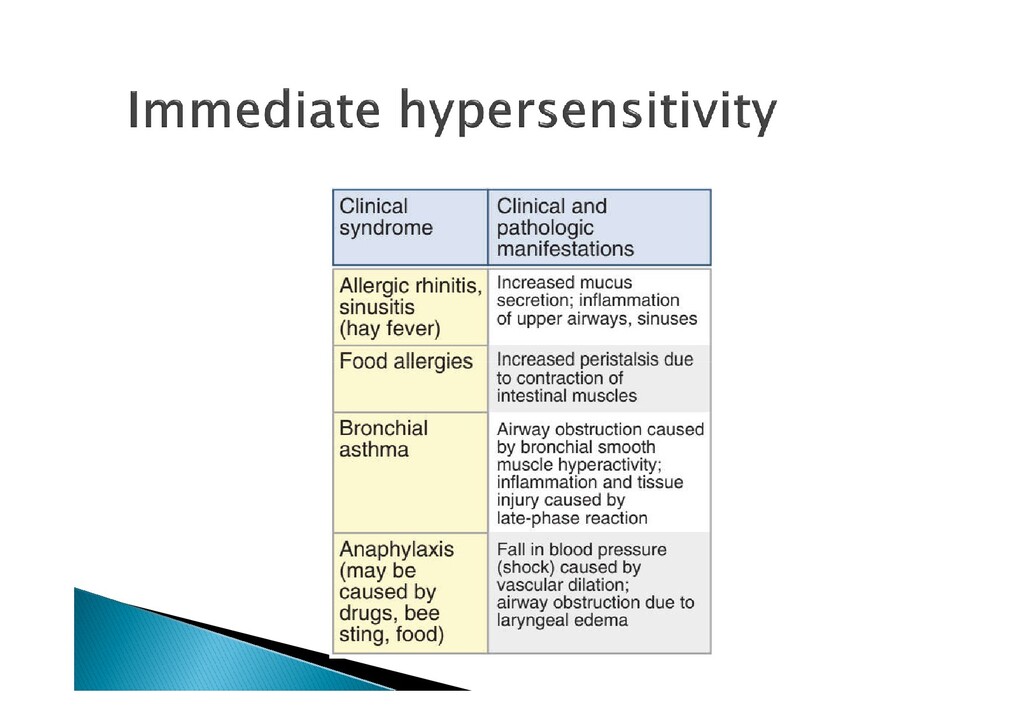
regulatory activities Immediate type hypersensitivity Isotype: class of Ig e.g. IgG, IgE, etc… Isotype: class of Ig e.g. IgG, IgE, etc… Class switching: switch from producing one Ig to another one. Hapten
Mostly caused by airborne allergens e.g. Mostly caused by airborne allergens e.g. allergic rhinits, allergic conjunctivitis & allergic asthma Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
factors. Seasonal variation of symptoms: Are ther Seasonal variation of symptoms: Are ther times in the years where your symptoms are worse or not? Prior response to medications Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
2) Work exposures. 3) Hobbies, sports, etc. 4) Presence of water damage at home or work place or visible mold. place or visible mold. 5) Presence of pets: how many, how far, within or outside house. Do you get worse when you are around your pets? 6) Age of mattress/bedding. 7) Age of carpeting at home Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
parental history of allergic rhinitis increases a 6-year old’s odds of allergic rhinitis by 1.84 A parental history of asthma increases a 6- year old’s odds of asthma by 2.72 A maternal history of eczema or atopy increases a 6-month old’s risk of eczema by 1.58 and 1.99, respectively. Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
can lead to appropriate testing, which may further help to confirm or exclude suspected foods. exclude suspected foods. Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
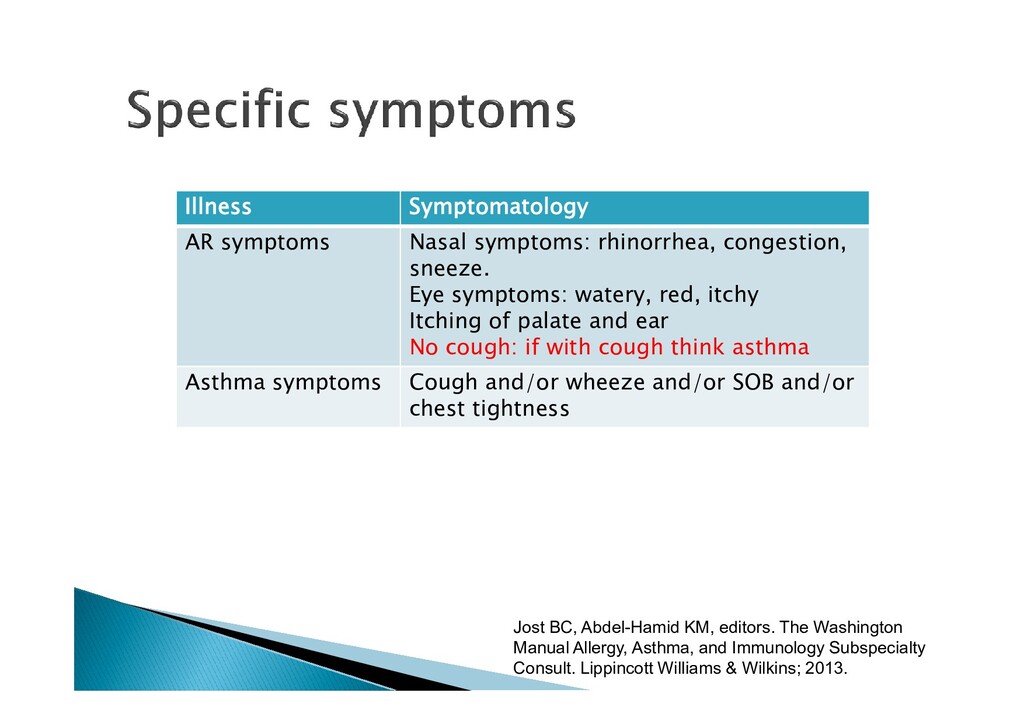
symptoms: watery, red, itchy Itching of palate and ear No cough: if with cough think asthma Asthma symptoms Cough and/or wheeze and/or SOB and/or chest tightness Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
Prolonged expiratory phase Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
pressure Angioedema is edema of the subcutaneous tissue; nonpruritic and often painful. tissue; nonpruritic and often painful. Scratch marks Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
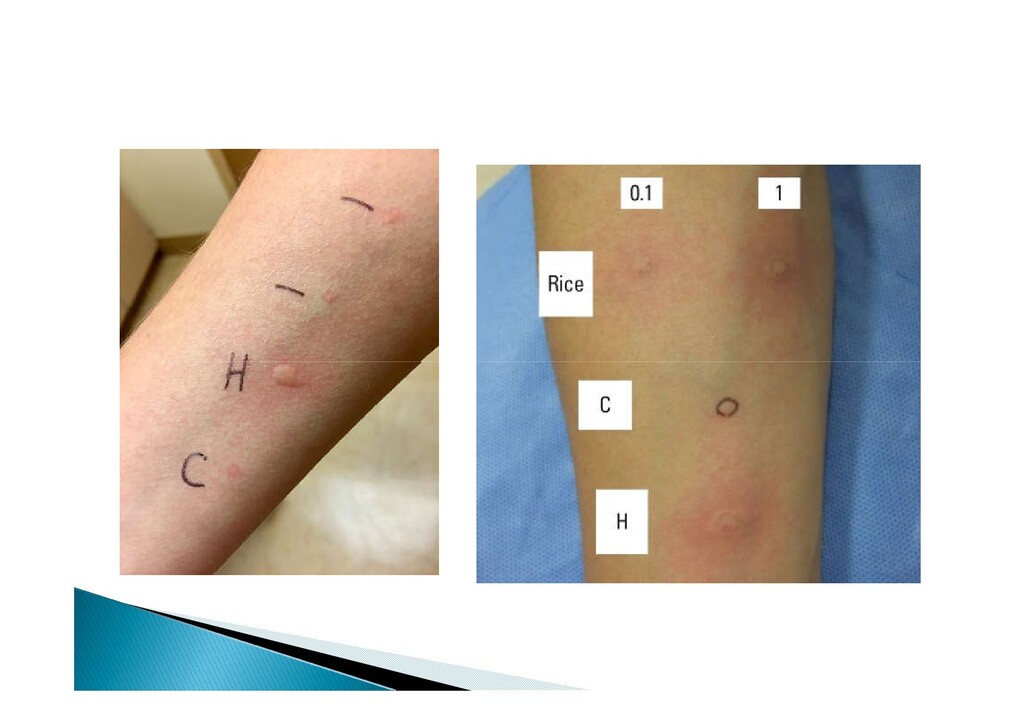
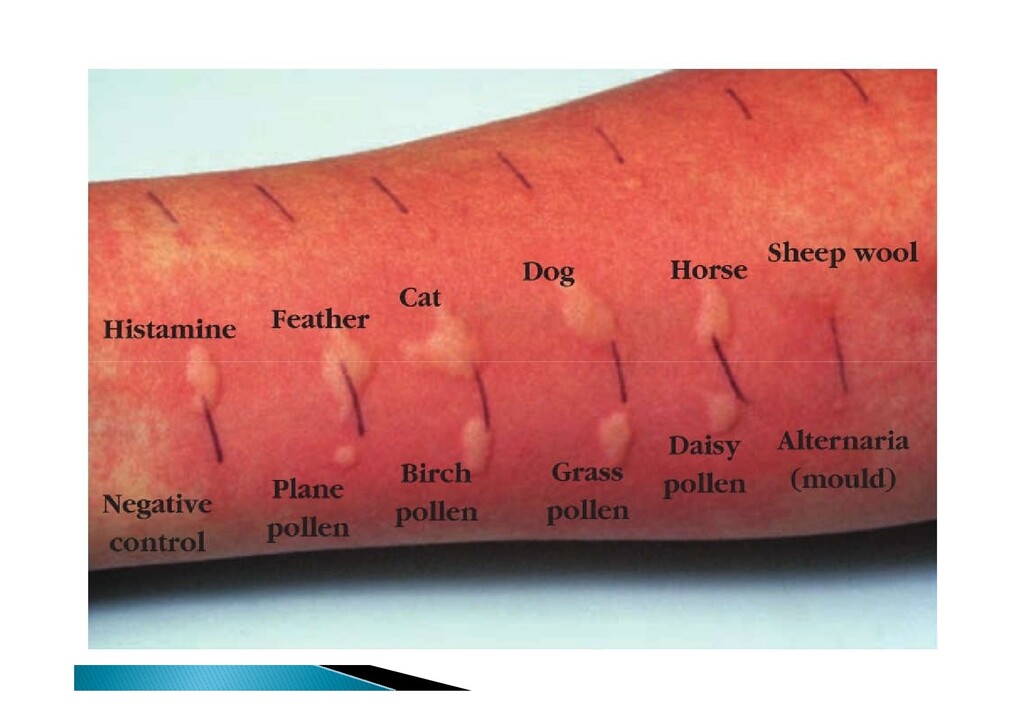
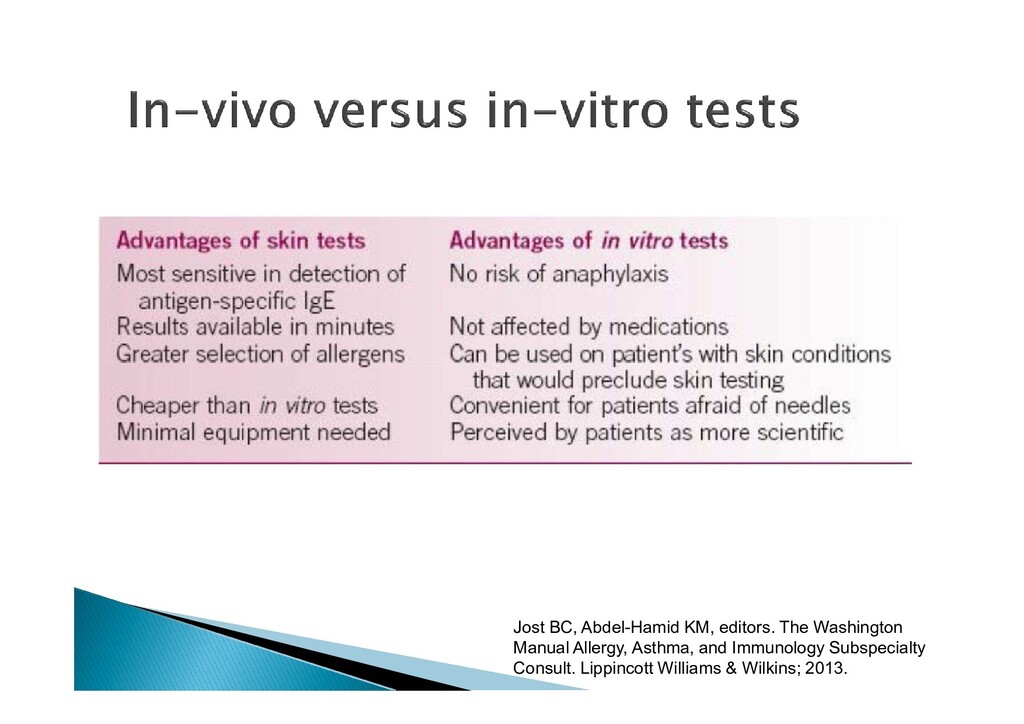
specific method to test for allergic sensitivity. Epicutaneous versus intradermal = in vivo measure of the presence of an = in vivo measure of the presence of an antigen-specific IgE. “wheal and flair” reaction. Resuscitation equipments available
specific method to test for allergic sensitivity. Epicutaneous versus intradermal = in vivo measure of the presence of an 1. Asthma (both to aeroallergens and occupational allergens) 2. Rhinitis 3. Conjunctivitis 4. Food allergy 5. Certain drug allergies 6. Insect hypersensitivity = in vivo measure of the presence of an antigen-specific IgE. “wheal and flair” reaction. Resuscitation equipments available 6. Insect hypersensitivity 7. Allergic bronchopulmonary aspergillosis 8. Local anesthetics Skin testing is usually postponed for 4– 6 weeks after the acute event.
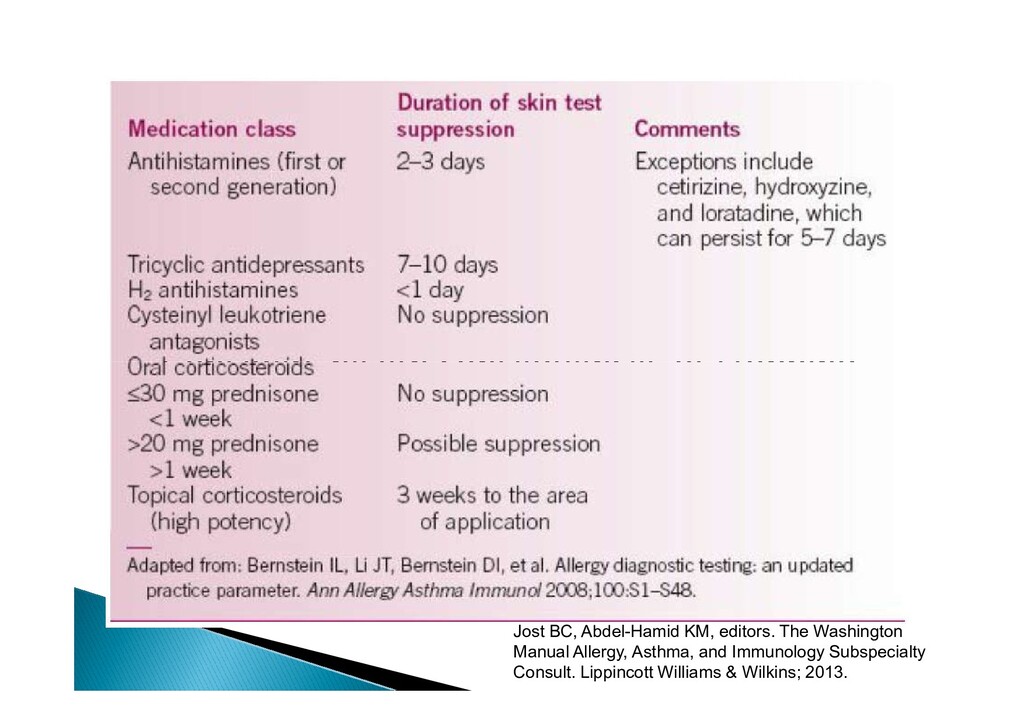
due to antihistaminic effects. Considers health consequences of stopping Considers health consequences of stopping important drug e.g. TCAs Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
due to antihistaminic effects. Considers health consequences of stopping Considers health consequences of stopping important drug e.g. TCAs Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
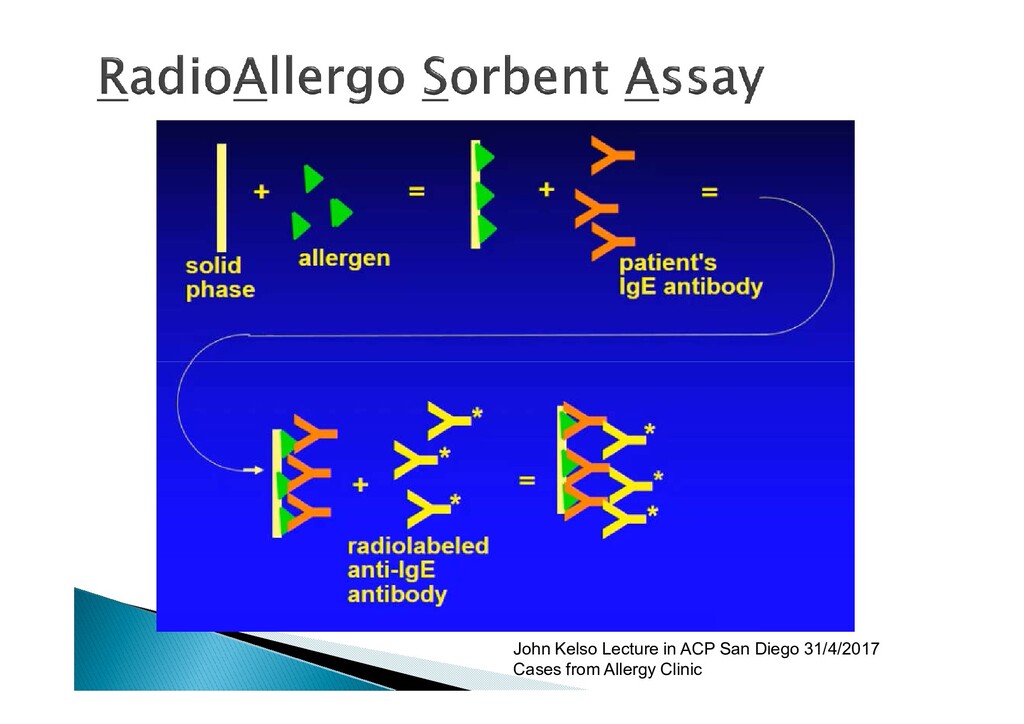
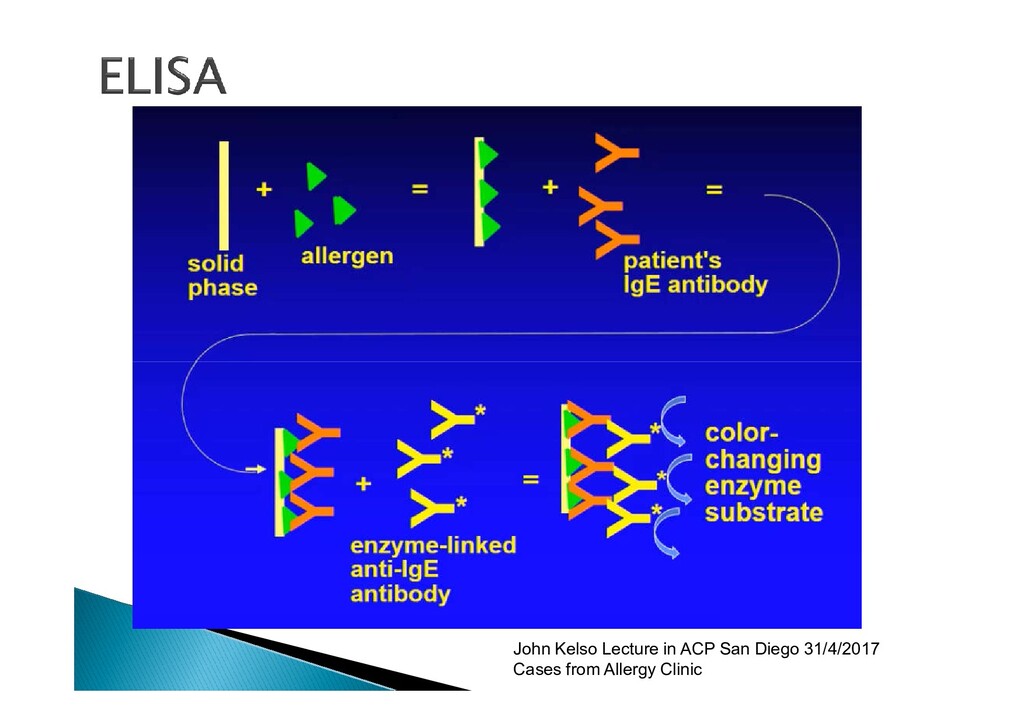
B. Radioallergosorbent test [RAST] and ImmunoCAP) is designed to screen for the presence of allergen-specific immunoglobulin E (IgE) in the patient’s the presence of allergen-specific immunoglobulin E (IgE) in the patient’s serum = lower sensitivity and specificity compared to epicutaneous skin testing but are helpful in instances where skin testing cannot be performed. Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
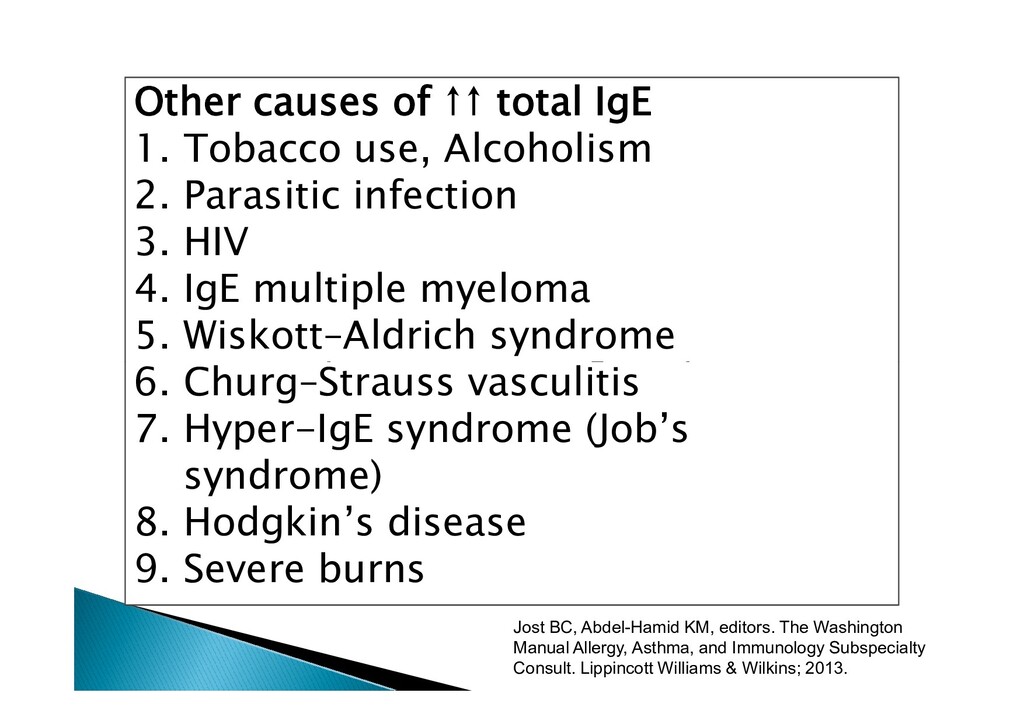
B. Radioallergosorbent test [RAST] and ImmunoCAP) is designed to screen for the presence of allergen-specific immunoglobulin E (IgE) in the patient’s Other causes of ↑↑ total IgE 1. Tobacco use, Alcoholism 2. Parasitic infection 3. HIV 4. IgE multiple myeloma 5. Wiskott–Aldrich syndrome 6. Churg–Strauss vasculitis the presence of allergen-specific immunoglobulin E (IgE) in the patient’s serum = lower sensitivity and specificity compared to epicutaneous skin testing but are helpful in instances where skin testing cannot be performed. 5. Wiskott–Aldrich syndrome 6. Churg–Strauss vasculitis 7. Hyper-IgE syndrome (Job’s syndrome) 8. Hodgkin’s disease 9. Severe burns Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
rapid onset. Anaphylaxis is a medical emergency. Anaphylaxis is a medical emergency. Jost BC, Abdel-Hamid KM, editors. The Washington Manual Allergy, Asthma, and Immunology Subspecialty Consult. Lippincott Williams & Wilkins; 2013.
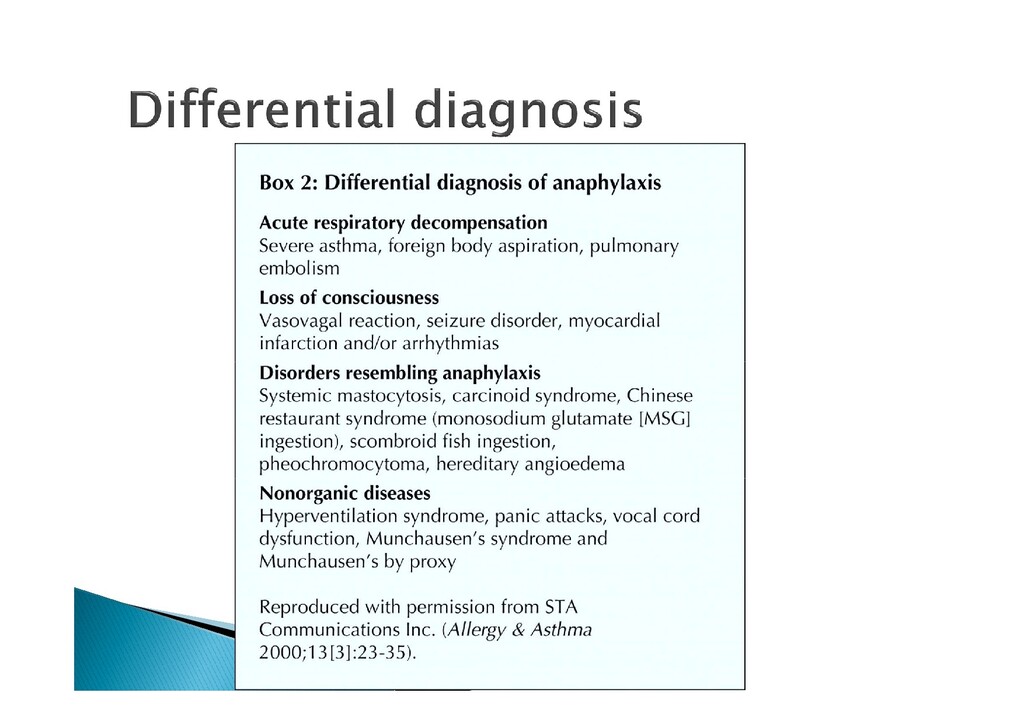
ingestion: eating mackerel and other related oily fish that are ‘off’ (scombroid poisoning due to are ‘off’ (scombroid poisoning due to breakdown of muscle histidine to histamine via bacterial spoilage). 5. Mastocytosis can also manifest with anaphylaxis.
(up to 70%): Rhinorrhea/sneezing, cough, choking, stridor, wheeze, bronchospasm, and laryngeal edema. and laryngeal edema. Cardiovascular (up to 45%): Hypotension, tachycardia, arrhythmia, myocardial infarction, and syncope. Gastrointestinal/genitourinary (up to 45%): Abdominal or uterine cramping, diarrhea, nausea, and vomiting.
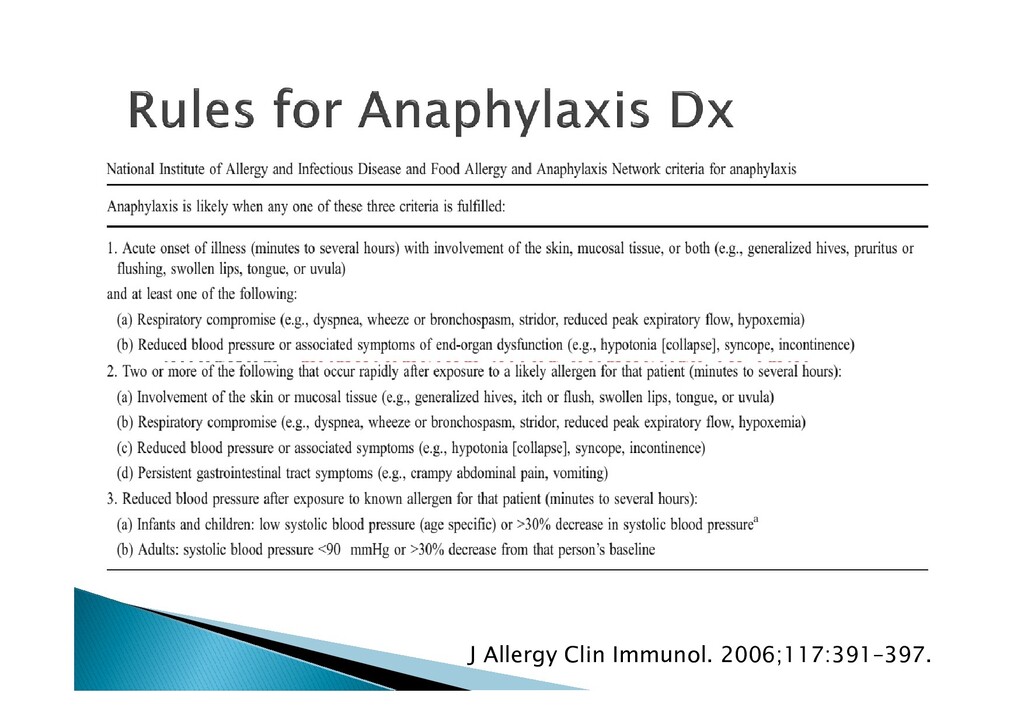
is an acute onset of symptoms in two organ systems, especially in the setting of an exposure to a possible provoking antigen. If the patient has a known allergy to a particular allergen, hypotension after exposure to that allergen, hypotension after exposure to that antigen is enough to make the diagnosis of anaphylaxis. A delayed reaction can occur in some individuals (biphasic reaction), leading to recurrence of symptoms 4–8 hours after the initial event. J Allergy Clin Immunol. 2006;117:391–397.
with recurrent anaphylaxis. Total tryptase will be elevated persistently even when patient is asymptomatic. asymptomatic. Protracted anaphylaxis requiring many hours of active resuscitation occurs in as many as 28% of patients → mostly due to fear of epinephrine adminstration.
history of shrimp allergy and it is OK to have regular fish as he has tried this before but without any problem After few spoons of delicious rice and fish, he After few spoons of delicious rice and fish, he started to experience intense facial swelling, wheeze and palpitation.
to test for related food stuff. 1/3 of patients allergic to true nuts are allergic to peanut and vice versa. allergic to peanut and vice versa. Significant cross reactivity within shellfish. No cross reactivity between shellfish & regular fish e.g. salmon, tuna…etc… The patient found some shrimp in his meal !!!
tyramine (headaches, hypertension in patients on MAOIs), alcohol Toxic: scombrotoxin (histamine from spoiled mackerel), green potatoes, flatoxins (peanuts) Enzyme deficiencies: lactase deficiency (common in Asians; diarrhoea due to laxative effect of lactose), also sucrase and maltase deficiency.
Test for suspected foods not all foods that the patients eat regularly. Commercial reagents are available If not, stab lancet into food and then into patient = Very dangerous. Test for related food (with known cross- reactivity)
4 symptoms… A, B, C… Resuscitation (IV line + fluid) & monitoring Resuscitation (IV line + fluid) & monitoring (vitals) Immediate epinephrine given intramuscularly in a dose of 0.3–0.5 mg (0.5–1mL of 1:1000) for an adult. The dose can be repeated if required.
4 symptoms… A, B, C… Resuscitation (IV line + fluid) & monitoring Don’t fear of IM adrenaline It is life saving Most cases of prolonged anaphylaxis and death are due to inadequate epinephrine use Resuscitation (IV line + fluid) & monitoring (vitals) Immediate epinephrine given intramuscularly in a dose of 0.3–0.5 mg (0.5–1mL of 1:1000) for an adult. The dose can be repeated if required. anaphylaxis and death are due to inadequate epinephrine use
bolus of hydrocortisone (100–200mg) should be given. should be given. Cochrane Reviews of antihistamines and steroids in the treatment of anaphylaxis conclude that evidence is lacking for both, but custom and practice recommend continued use.
bolus of hydrocortisone (100–200mg) should be given. If the previous and current reaction only hives, give antihistamine & CS and observe should be given. Cochrane Reviews of antihistamines and steroids in the treatment of anaphylaxis conclude that evidence is lacking for both, but custom and practice recommend continued use. If any respiratory or CV symptoms = use epinephrine pen + go to ER If prior history is severe = Epipen + ER
Latex allergic patients = worsen in hospital Learn patients to use Epinephrine pen (even if Learn patients to use Epinephrine pen (even if first presentation is only hives) + be prepared to treat accidental ingestion. Avoid allergens + dietician consult.
to 2-4 hours (especially for parenteral one) Inquire about what happened before? When? And after how many doses Most adverse drug reaction termed Nature of reactions: hives, GI, resp or cardiac Most adverse drug reaction termed allergic by public
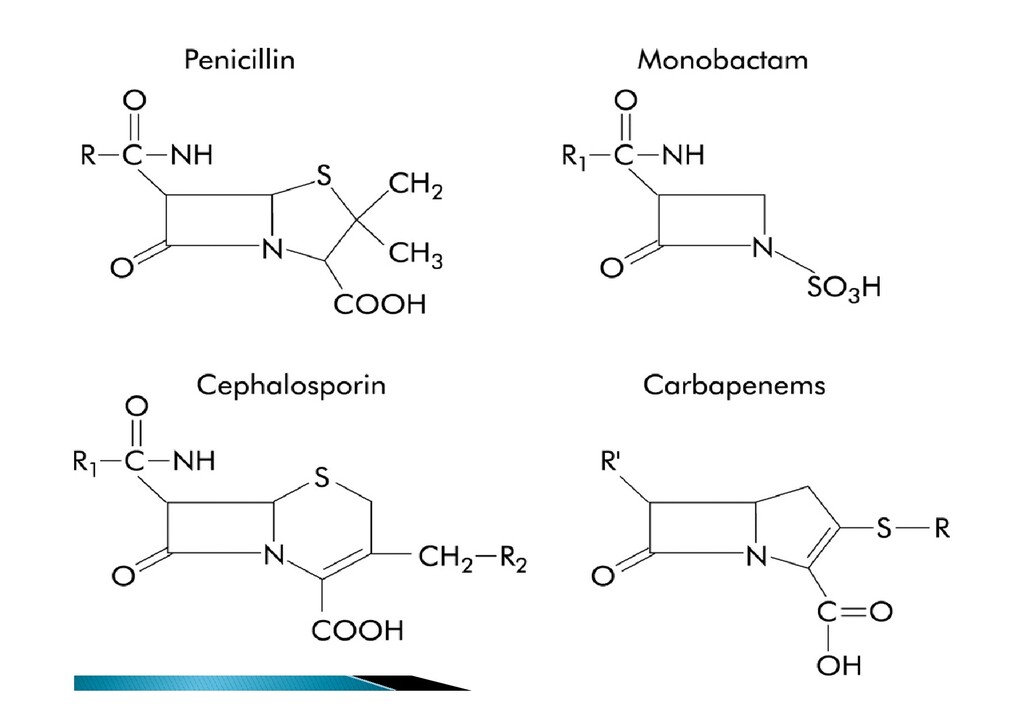
to 2-4 hours (especially for parenteral one) Inquire about what happened before? When? And after how many doses Most adverse drug reaction termed Occasional patients react on apparent first exposure and it has been suggested that sensitization may occur through antibiotics Nature of reactions: hives, GI, resp or cardiac Most adverse drug reaction termed allergic by public may occur through antibiotics present in food. All four types of Gell and Coombs’ hypersensitivity reactions may occur with penicillin, together with reactions of uncertain significance such as Stevens– Johnson syndrome.
<10% of those have positive skin tests <10% of patients labeled allergic are currently <10% of patients labeled allergic are currently not Either wrongly diagnosed or penicillin allergy tend to wane over time
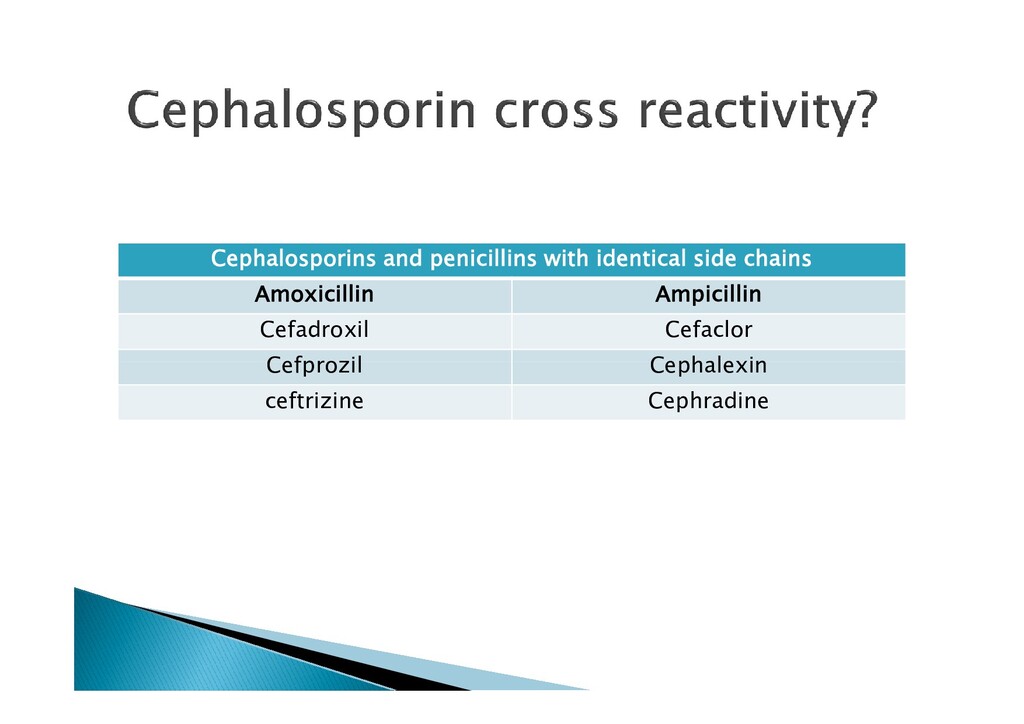
commercially available Minor determinants (penicilloate & penilloate) are not commercially available. are not commercially available. % of patients are positive only to minor determinant → i.e. will be missed Amoxicillin has ch.ch. side chain to which patients may be allergic to.
1/10,000 of therapeutic dose every 15 1/10,000 of therapeutic dose every 15 minutes till full dose acomplished Anaphylaxis may occur It is temporary option: i.e. if interrupted you should start again)
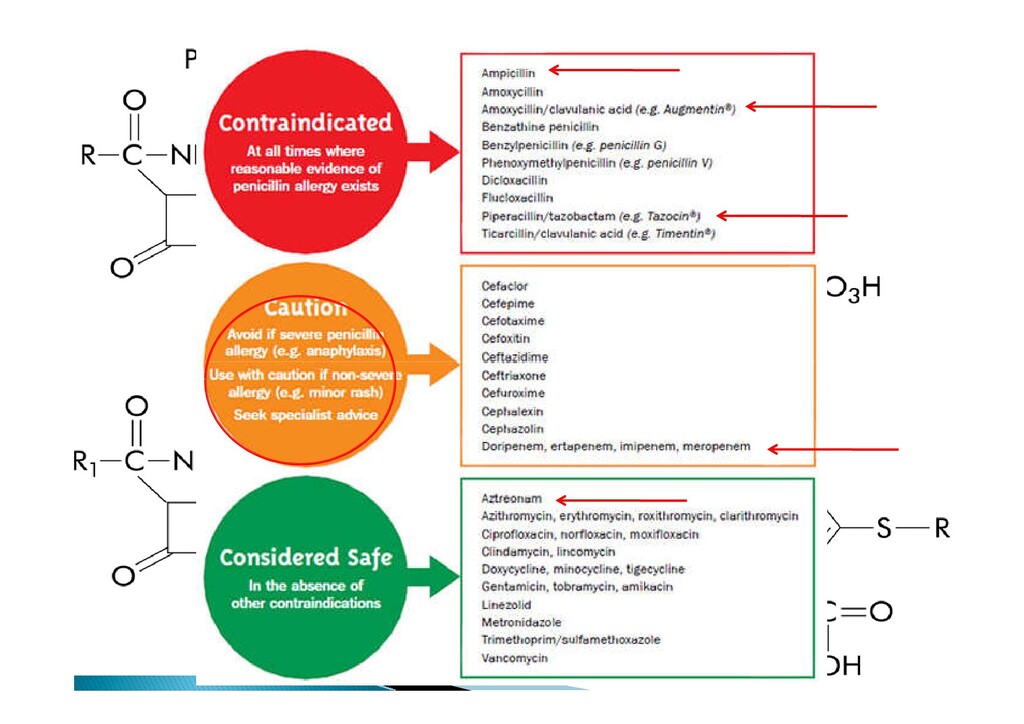
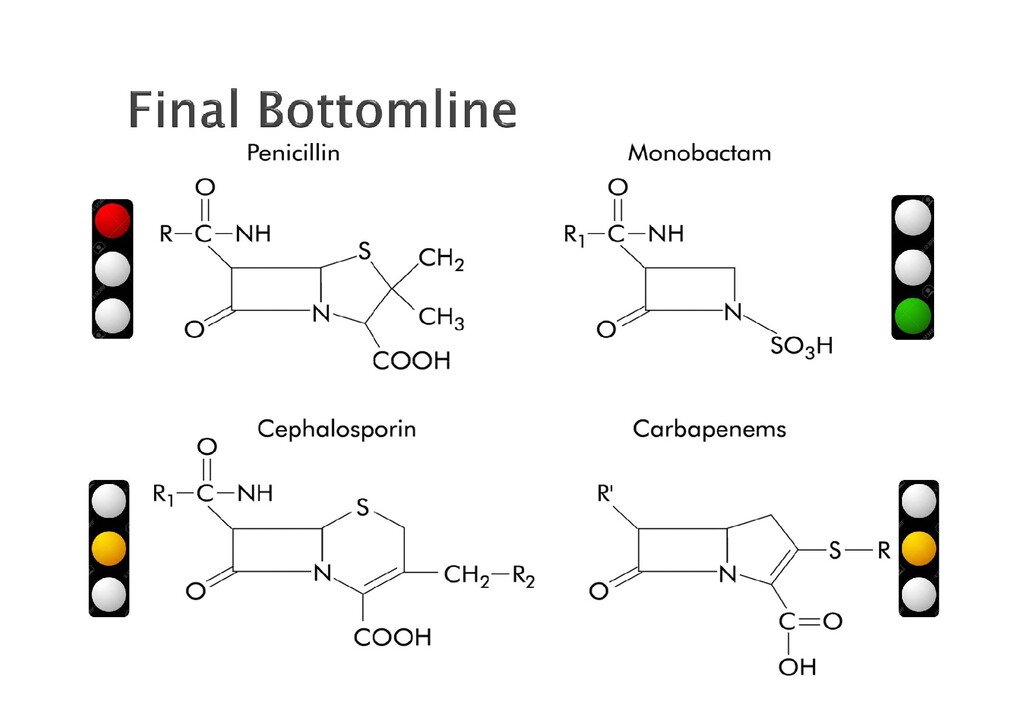
reactivity are due to similarity of side chains chains Patients can be independently cephalosporin allergic. It can not be anticipated but be cautious
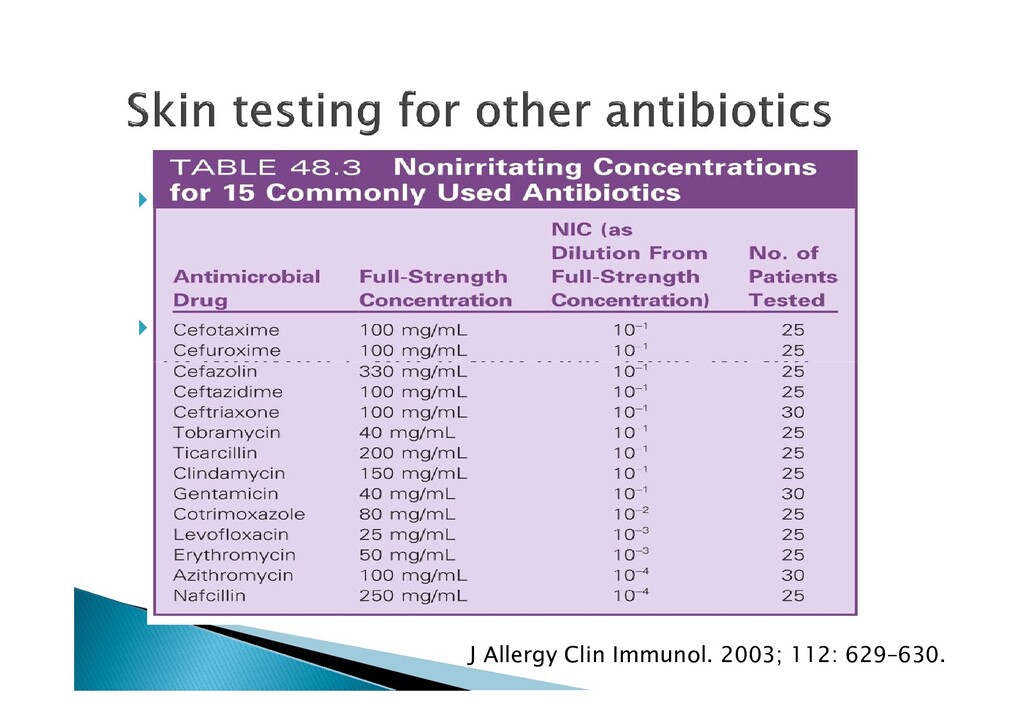
is available If utilized, they are only helpful if positive (dangerous), but if negative, they are not (dangerous), but if negative, they are not reassuring. J Allergy Clin Immunol. 2003; 112: 629–630.
is available If utilized, they are only helpful if positive (dangerous), but if negative, they are not (dangerous), but if negative, they are not reassuring. J Allergy Clin Immunol. 2003; 112: 629–630.
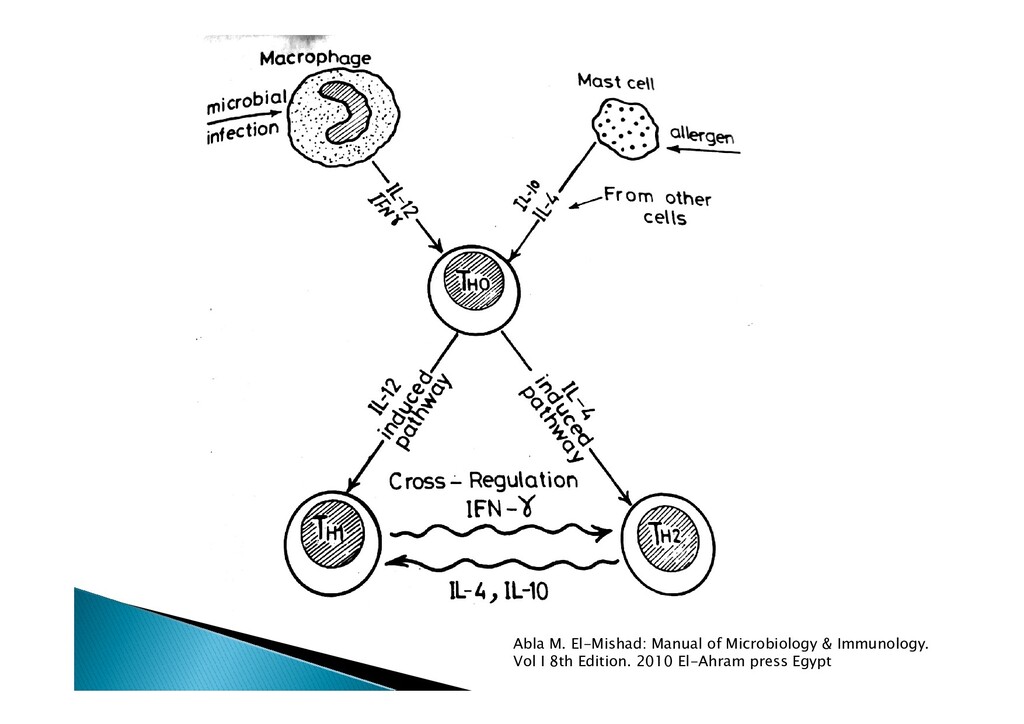
housing + hygiene theory No one is born allergic to anything, you only inherit the susceptibility to be allergic, i.e. inherit the susceptibility to be allergic, i.e. genetic background + environmental trigger. TH2 cells direct the immune system towards allergic type of response
mast cells, IgE, IL-4, 5, 13 IgE mediated mast cell degranualtion type of allergy are immediate up to 2-4 hours allergy are immediate up to 2-4 hours Proper history taking and look for allergy hits Tests of allergy are available, ask for it
adrenaline, it is lifesaving Virtually all food can cause allergy, but take Virtually all food can cause allergy, but take care of common food allergen, and take care of cross reactivity Be ready of any accidental ingestion
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}