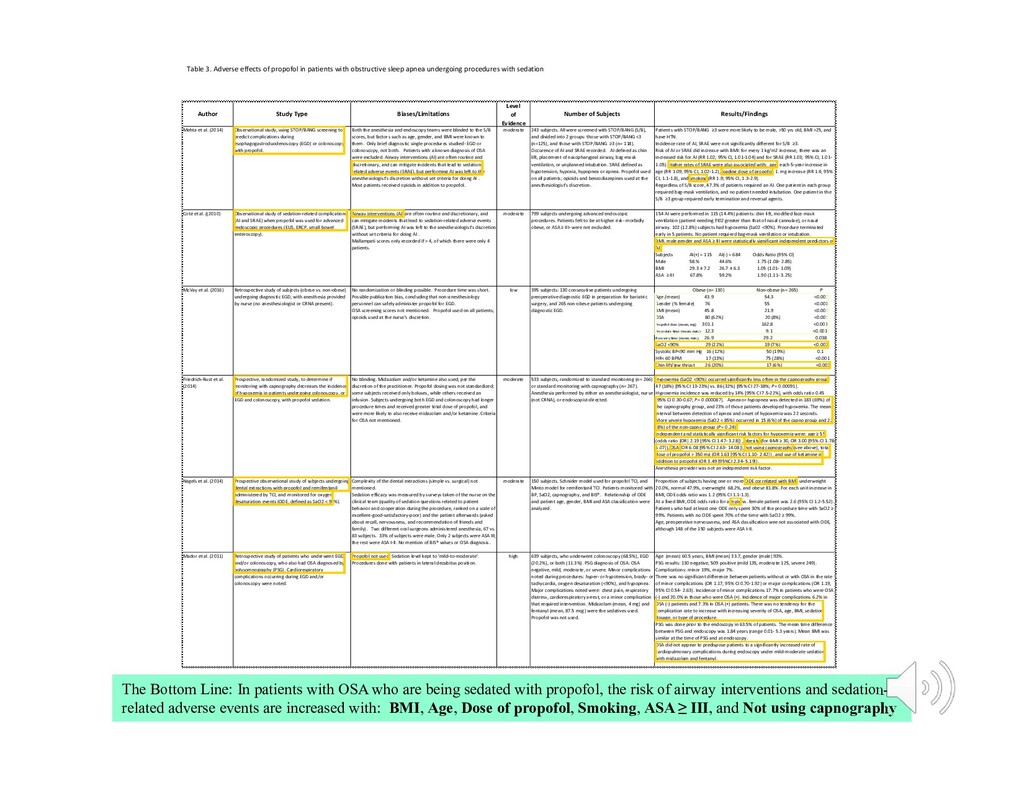
sleep apnea undergoing procedures with sedation Author Study Type Biases/Limitations Level of Evidence Number of Subjects Results/Findings Mehta et al. (2014) Observational study, using STOP/BANG screening to predict complications during esophagogastroduodenoscopy (EGD) or colonoscopy with propofol. Both the anesthesia and endoscopy teams were blinded to the S/B scores, but factors such as age, gender, and BMI were known to them. Only brief diagnostic single procedures studied- EGD or colonoscopy, not both. Patients with a known diagnosis of OSA were excluded. Airway interventions (AI) are often routine and discretionary, and can mitigate incidents that lead to sedation- related adverse events (SRAE), but performing AI was left to the anesthesiologist's discretion without set criteria for doing AI . Most patients received opioids in addition to propofol. moderate 243 subjects. All were screened with STOP/BANG (S/B), and divided into 2 groups: those with STOP/BANG <3 (n=125), and those with STOP/BANG ≥3 (n= 118). Occurence of AI and SRAE recorded. AI defined as chin lift, placement of nasopharygeal airway, bag-mask ventilation, or unplanned intubation. SRAE defined as hypotension, hypoxia, hypopnea or apnea. Propofol used on all patients; opioids and benzodiazepines used at the anesthesiologist's discretion. Patients with STOP/BANG ≥3 were more likely to be male, >50 yrs old, BMI >25, and have HTN. Incidence rate of AI, SRAE were not significantly different for S/B ≥3. Risk of AI or SRAE did increase with BMI: for every 1 kg/m2 increase, there was an increased risk for AI (RR 1.02; 95% CI, 1.01-1.04) and for SRAE (RR 1.03; 95% CI, 1.01- 1.05). Higher rates of SRAE were also associated with: age; each 5-year increase in age (RR 1.09; 95% CI, 1.02-1.2), loading dose of propofol; 1. mg increase (RR 1.4; 95% CI, 1.1-1.8), and smoking (RR 1.9; 95% CI, 1.3-2.9). Regardless of S/B score, 47.3% of patients required an AI. One patient in each group required bag-mask ventilation, and no patient needed intubation. One patient in the S/B ≥3 group required early termination and reversal agents. Coté et al. ((2010) Observational study of sedation-related complications (AI and SRAE) when propofol was used for advanced endoscopic procedures (EUS, ERCP, small bowel enteroscopy). Airway interventions (AI) are often routine and discretionary, and can mitigate incidents that lead to sedation-related adverse events (SRAE), but performing AI was left to the anesthesiologist's discretion without set criteria for doing AI . Mallampati scores only recorded if > 4, of which there were only 4 patients. moderate 799 subjects undergoing advanced endoscopic procedures. Patients felt to be at higher risk- morbidly obese, or ASA ≥ III- were not excluded. 154 AI were performed in 115 (14.4%) patients: chin lift, modified face mask ventilation (patient needing FI02 greater than that of nasal cannulae), or nasal airway. 102 (12.8%) subjects had hypoxemia (Sa02 <90%). Procedure terminated early in 5 patients. No patient required bag-mask ventilation or intubation. BMI, male gender and ASA ≥ III were statistically significant independent predictors of AI. Subjects AI(+) = 115 AI(-) = 684 Odds Ratio (95% CI) Male 58.% 44.6% 1.75 (1.08- 2.85) BMI 29.3 ± 7.2 26.7 ± 6.3 1.05 (1.01- 1.09) ASA ≥ III 67.8% 59.2% 1.90 (1.11- 3.25) McVay et al. (2016) Retrospective study of subjects (obese vs. non-obese) undergoing diagnostic EGD, with anesthesia provided by nurse (no anesthesiologist or CRNA present). No randomization or blinding possible. Procedure time was short. Possible publication bias, concluding that non-anesthesiology personnel can safely administer propofol for EGD. OSA screening scores not mentioned. Propofol used on all patients; opioids used at the nurse's discretion. low 395 subjects: 130 consecutive patients undergoing preoperative diagnostic EGD in preparation for bariatric surgery, and 265 non-obese patients undergoing diagnostic EGD. Obese (n= 130) Non-obese (n= 265) P Age ( mean) 43.9 54.3 <0.001 Gender (% female) 76 55 <0.001 BMI (mean) 45.8 21.9 <0.001 OSA 80 (62%) 20 (8%) <0.001 Propofol dose (mean, mg) 301.1 162.8 <0.001 Procedure time (mean, min.) 12.3 9.1 <0.001 Recovery time (mean, min.) 26.9 29.2 0.038 SaO2 <90% 29 (22%) 19 (7%) <0.001 Systolic BP<90 mm Hg 16 (12%) 50 (19%) 0.1 HR< 60 BPM 17 (13%) 75 (28%) <0.001 Chin lift/jaw thrust 26 (20%) 17 (6%) <0.001 Friedrich-Rust et al. (2014) Prospective, randomized study, to determine if monitoring with capnography decreases the incidence of hypoxemia in patients undergoing colonoscopy, or EGD and colonoscopy, with propofol sedation. No blinding. Midazolam and/or ketamine also used, per the discretion of the practitioner. Propofol dosing was not standardized; some subjects received only boluses, while others received an infusion. Subjects undergoing both EGD and colonoscopy had longer procedure times and received greater total dose of propofol, and were more likely to also receive midazolam and/or ketamine. Criteria for OSA not mentioned. moderate 533 subjects, randomized to standard monitoring (n= 266) or standard monitoring with capnography (n= 267). Anesthesia performed by either an anesthesiologist, nurse (not CRNA), or endoscopist-directed. Hypoxemia (SaO2 <90%) occurred significantly less often in the capnography group: 47 (18%) [95% CI 13-23%] vs. 86 (32%) [95% CI 27-38%; P = 0.00091]. Hypoxemia incidence was reduced by 14% [95% CI 7.5-22%], with odds ratio 0.45 [95% CI 0.30-0.67; P= 0.000087]. Apnea or hypopnea was detected in 183 (69%) of the capnography group, and 23% of those patients developed hypoxemia. The mean interval between detection of apnea and onset of hypoxemia was 22 seconds. More severe hypoxemia (SaO2 < 85%) occurred in 15 (6%) of the capno group and 22 (8%) of the non-capno group (P = 0.24). Independent and statistically significant risk factors for hypoxemia were: age ≥ 55 (odds ratio [OR] 2.19 [95% CI 1.47- 3.28]) , obesity (for BMI ≥ 30, OR 3.00 [95% CI 1.78- 5.07]), OSA (OR 6.08 [95% CI 2.63- 14.08]), not using capnography (see above), total dose of propofol > 350 mg (OR 1.63 [95% CI 1.10- 2.42]) , and use of ketamine in addition to propofol (OR 3.49 [95%CI 2.34- 5.19]). Anesthesia provider was not an independent risk factor. Nagels et al. (2014) Prospective observational study of subjects undergoing dental extractions with propofol and remifentanil administered by TCI, and monitored for oxygen desaturation events (ODE, defined as SaO2 < 94%). Complexity of the dental extractions (simple vs. surgical) not mentioned. Sedation efficacy was measured by surveys taken of the nurse on the clinical team (quality of sedation questions related to patient behavior and cooperation during the procedure, ranked on a scale of excellent-good-satisfactory-poor) and the patient afterwards (asked about recall, nervousness, and recommendation of friends and family). Two different oral surgeons administered anesthesia, 67 vs. 83 subjects. 33% of subjects were male. Only 2 subjects were ASA III; the rest were ASA I-II. No mention of BIS® values or OSA diagnosis. moderate 150 subjects. Schnider model used for propofol TCI, and Minto model for remifentanil TCI. Patients monitored with BP, SaO2, capnography, and BIS®. Relationship of ODE and patient age, gender, BMI and ASA classification were analyzed. Proportion of subjects having one or more ODE correlated with BMI: underweight 20.0%, normal 47.9%, overweight 68.2%, and obese 81.8%. For each unit increase in BMI, ODE odds ratio was 1.2 (95% CI 1.1-1.3). At a fixed BMI, ODE odds ratio for a male vs. female patient was 2.6 (95% CI 1.2-5.52). Patients who had at least one ODE only spent 30% of the procedure time with SaO2 ≥ 99%. Patients with no ODE spent 70% of the time with SaO2 ≥ 99%. Age, preoperative nervousness, and ASA classification wee not associated with ODE, although 148 of the 150 subjects were ASA I-II. Mador et al. (2011) Retrospective study of patients who underwent EGD and/or colonoscopy, who also had OSA diagnosed by polysomnography (PSG). Cardiorespiratory complications occurring during EGD and/or colonoscopy were noted. Propofol not used. Sedation level kept to 'mild-to-moderate'. Procedures done with patients in lateral decubitus position. high 639 subjects, who underwent colonoscopy (68.5%), EGD (20.2%), or both (11.3%). PSG diagnosis of OSA: OSA negative, mild, moderate, or severe. Minor complications noted during procedures: hyper- or hypotension, brady- or tachycardia, oxygen desaturation (<90%), and hypopnea. Major complications noted were: chest pain, respiratory distress, cardiorespiratory arrest, or a minor complication that required intervention. Midazolam (mean, 4 mg) and fentanyl (mean, 87.5 mcg) were the sedatives used. Propofol was not used. Age (mean) 60.5 years, BMI (mean) 33.7, gender (male) 93%. PSG results: 130 negative, 509 positive (mild 135, moderate 125, severe 249). Complications: minor 19%, major 7%. There was no significant difference between patients without or with OSA in the rate of minor complications (OR 1.17, 95% CI 0.70-1.92) or major complications (OR 1.19, 95% CI 0.54- 2.63). Incidence of minor complications 17.7% in patients who were OSA (-) and 20.0% in those who were OSA (+). Incidence of major complications 6.2% in OSA (-) patients and 7.3% in OSA (+) patients. There was no tendency for the complication rate to increase with increasing severity of OSA, age, BMI, sedation dosage, or type of procedure. PSG was done prior to the endoscopy in 63.5% of patients. The mean time difference between PSG and endoscopy was 1.84 years (range 0.01- 5.3 years). Mean BMI was similar at the time of PSG and at endoscopy. OSA did not appear to predispose patients to a significantly increased rate of cardiopulmonary complications during endoscopy under mild-moderate sedation with midazolam and fentanyl. The Bottom Line: In patients with OSA who are being sedated with propofol, the risk of airway interventions and sedation- related adverse events are increased with: BMI, Age, Dose of propofol, Smoking, ASA ≥ III, and Not using capnography
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}