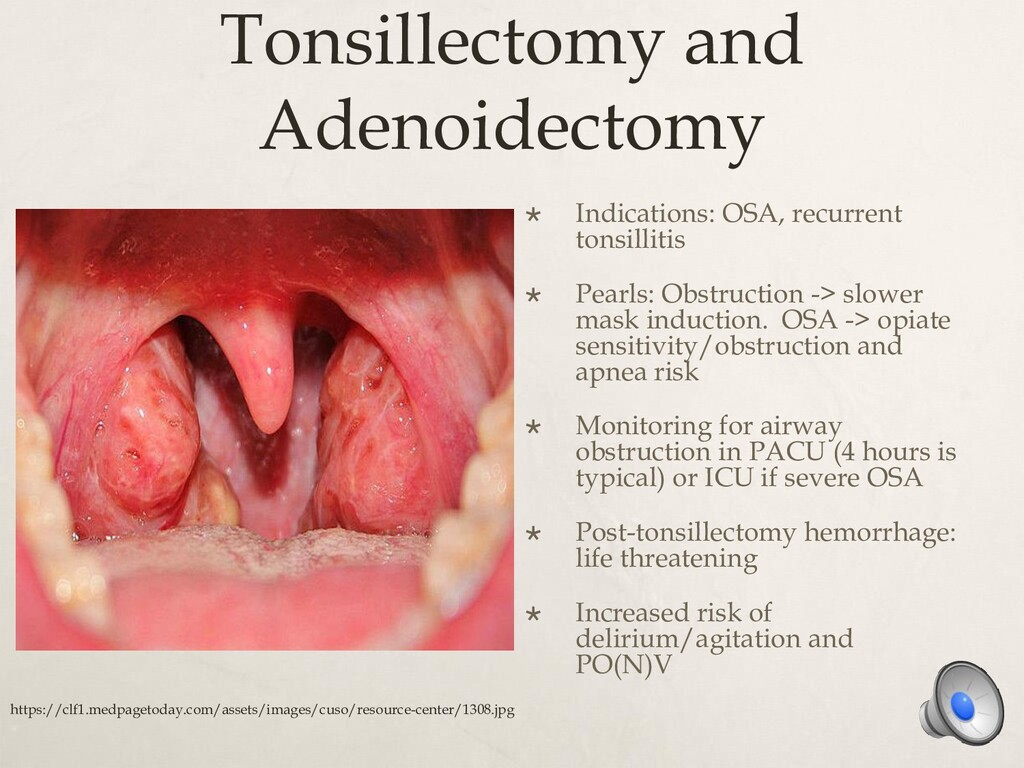
Obstruction -> slower mask induction. OSA -> opiate sensitivity/obstruction and apnea risk Monitoring for airway obstruction in PACU (4 hours is typical) or ICU if severe OSA Post-tonsillectomy hemorrhage: life threatening Increased risk of delirium/agitation and PO(N)V https://clf1.medpagetoday.com/assets/images/cuso/resource-center/1308.jpg
auditory evoked potentials, Tympanoplasty, etc If short procedure and healthy child: mask/no IV is common. IM and intranasal analgesia common May need to eschew paralytics if cranial nerve monitoring. Patient cannot move under microscopy. PO(N)V common due to vestibular stimulation
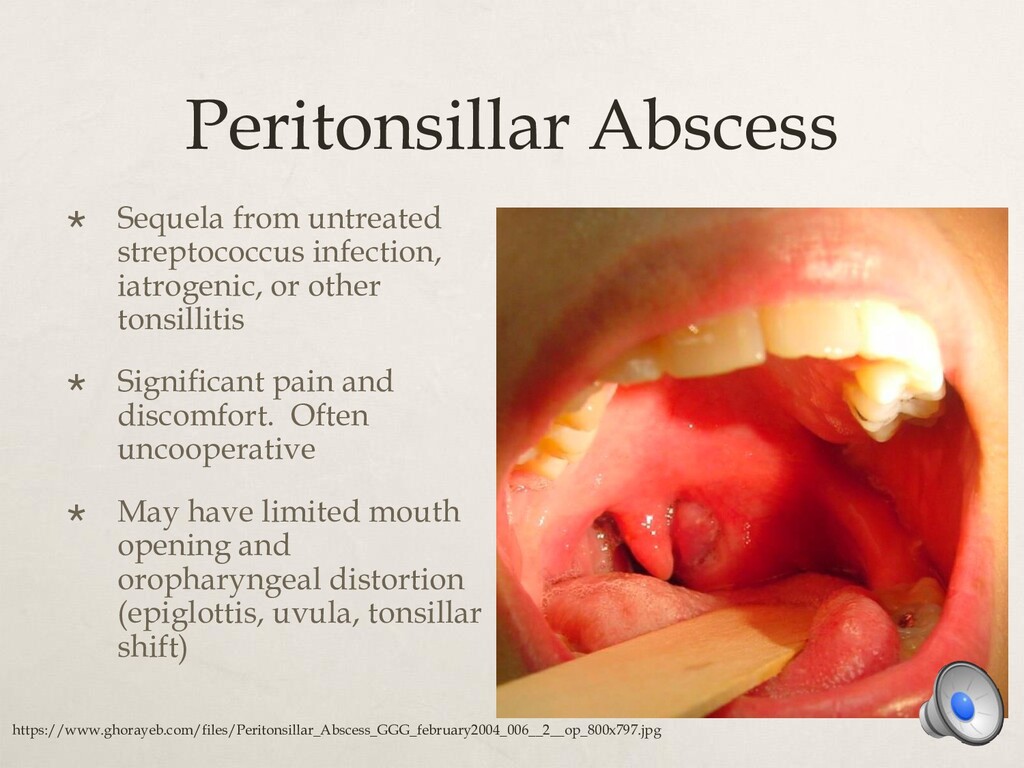
other tonsillitis Significant pain and discomfort. Often uncooperative May have limited mouth opening and oropharyngeal distortion (epiglottis, uvula, tonsillar shift) https://www.ghorayeb.com/files/Peritonsillar_Abscess_GGG_february2004_006__2__op_800x797.jpg
X-Ray findings, evaluation of laryngomalacia or tracheomalacia Anesthetic: Often careful, controlled mask induction -> TIVA with spontaneous ventilation TIVA cocktail varies widely between practitioners and institutions Combinations of propofol, dexmedetomidine, remifentanil, sevoflurane common. Perfect cocktail still being debated! Sometimes paired with sleep endoscopy. Difficult to maintain spontaneous ventilation under general anesthesia that mimics natural sleep. Propofol may over-exaggerate endoscopic findings.
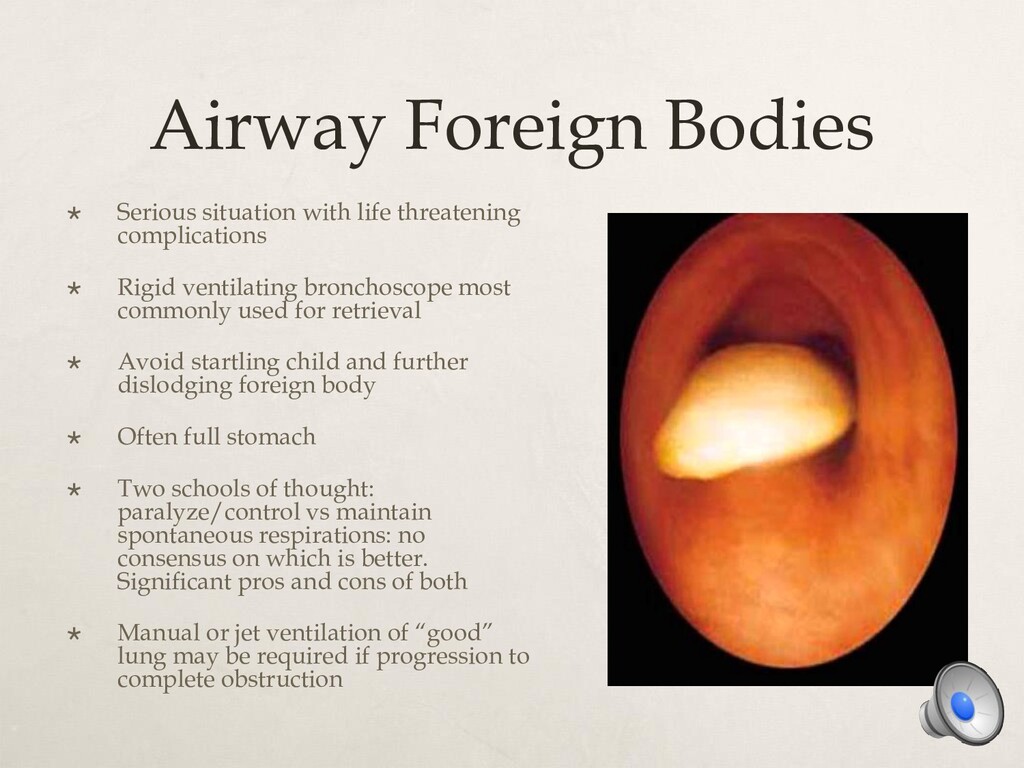
Rigid ventilating bronchoscope most commonly used for retrieval Avoid startling child and further dislodging foreign body Often full stomach Two schools of thought: paralyze/control vs maintain spontaneous respirations: no consensus on which is better. Significant pros and cons of both Manual or jet ventilation of “good” lung may be required if progression to complete obstruction
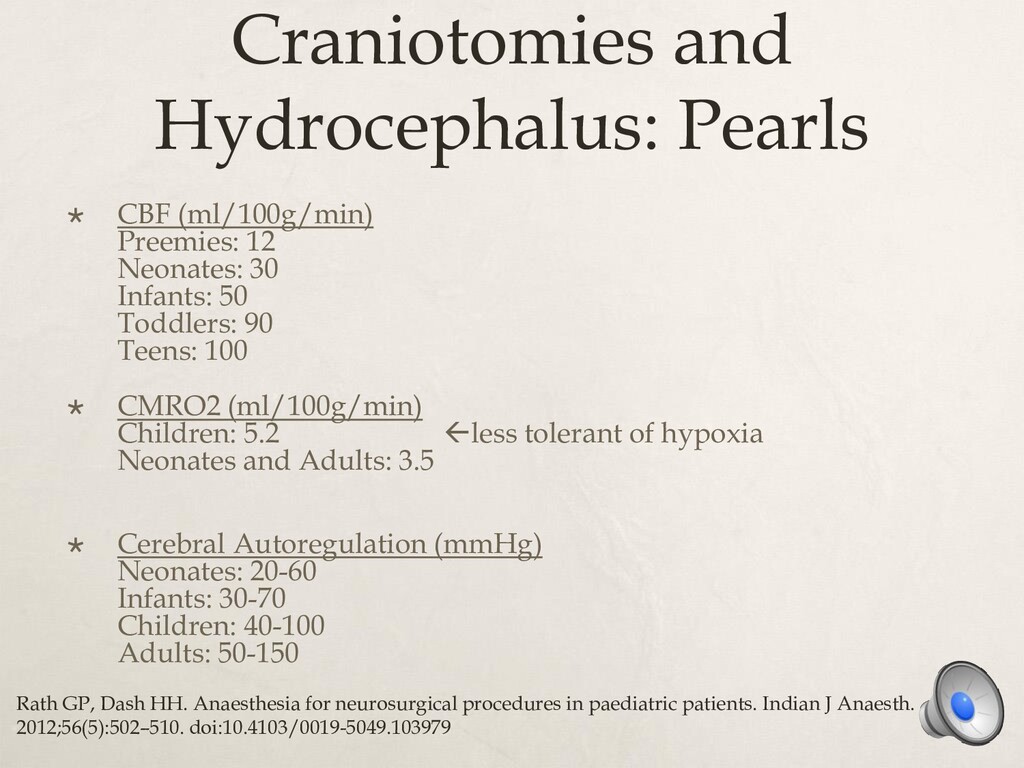
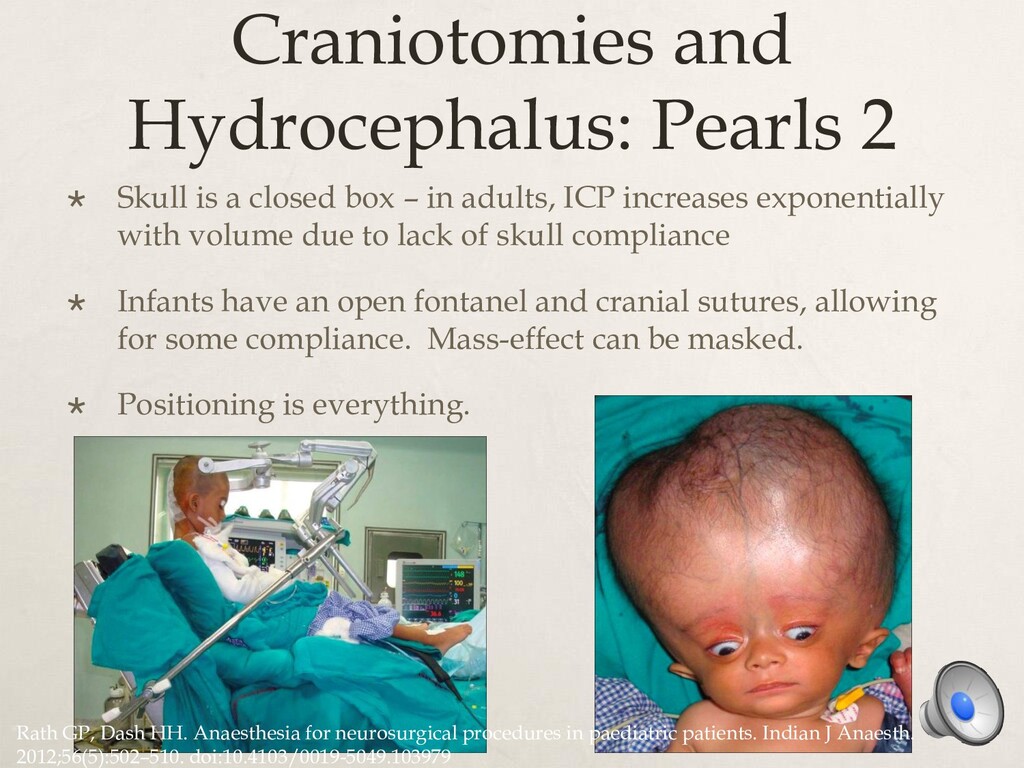
box – in adults, ICP increases exponentially with volume due to lack of skull compliance Infants have an open fontanel and cranial sutures, allowing for some compliance. Mass-effect can be masked. Positioning is everything. Rath GP, Dash HH. Anaesthesia for neurosurgical procedures in paediatric patients. Indian J Anaesth. 2012;56(5):502–510. doi:10.4103/0019-5049.103979
Sitting position massively increases risk of Venous Air Embolism Flexion or extension of head/neck can cause brainstem compression (Arnold-Chiari malform) or ETT malpositioning Revisions often involve tunneling through existing scar tissue in abdomen, which can make surgeries more complicated or risk vascular or bowel injuries
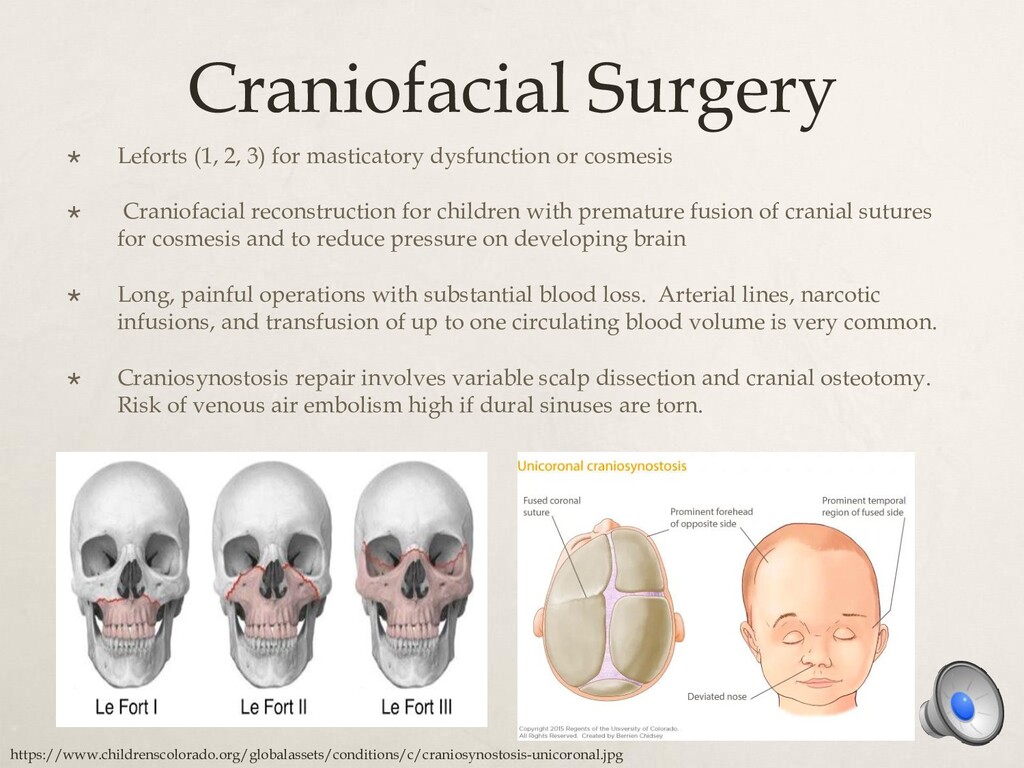
or cosmesis Craniofacial reconstruction for children with premature fusion of cranial sutures for cosmesis and to reduce pressure on developing brain Long, painful operations with substantial blood loss. Arterial lines, narcotic infusions, and transfusion of up to one circulating blood volume is very common. Craniosynostosis repair involves variable scalp dissection and cranial osteotomy. Risk of venous air embolism high if dural sinuses are torn. https://www.childrenscolorado.org/globalassets/conditions/c/craniosynostosis-unicoronal.jpg
but may still be life- threatening due to tracheal, great vessel, or cardiac compression Etiologies: Lymphoma, thymoma, germ cell tumor, metastasis, bronchogenic masses, thyroid masses Preop assessment CRITICAL: evaluate for dyspnea, stridor, syncope, or postural symptom change Induction of GA may be catastrophic if mass shits and compresses vital structures, resulting in failure to ventilate or circulate Maintain spontaneous ventilation in patient’s least symptomatic position, avoid paralytics and positive pressure ventilation.
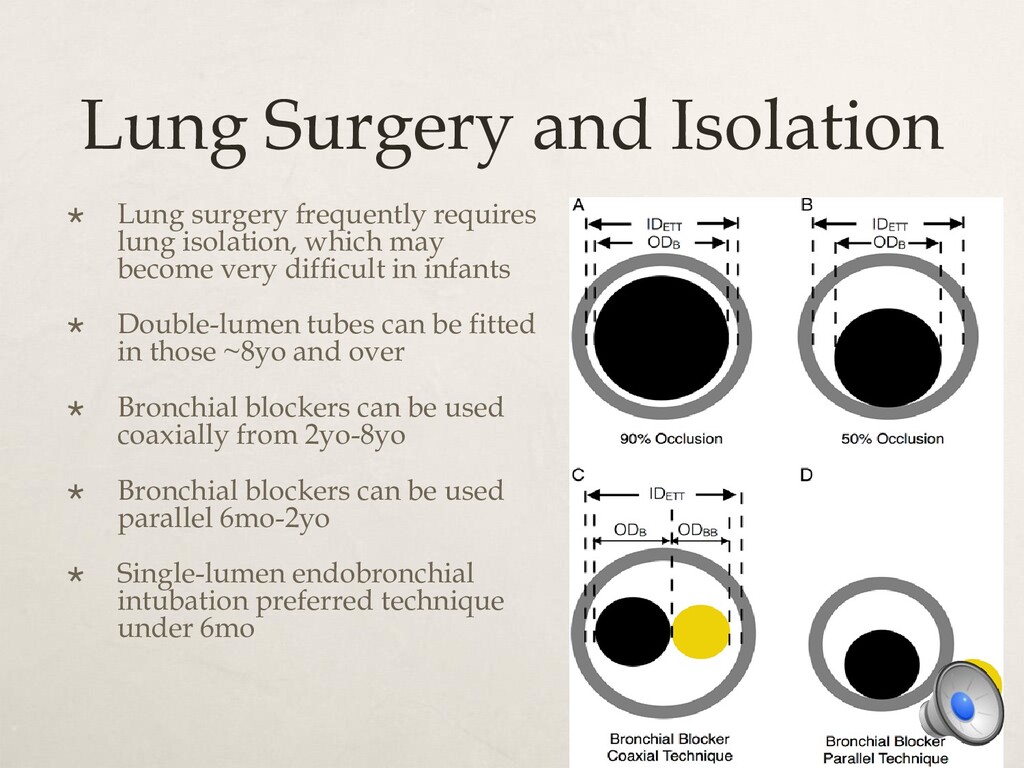
isolation, which may become very difficult in infants Double-lumen tubes can be fitted in those ~8yo and over Bronchial blockers can be used coaxially from 2yo-8yo Bronchial blockers can be used parallel 6mo-2yo Single-lumen endobronchial intubation preferred technique under 6mo
volume reduction and cardiac compression. The Nuss procedure is done for severe cases. Nuss: Minimally invasive surgery wherein 2-3 steel bars are tunneled behind the breastbone and attached to the outer ribs. The ribs and sternum are then raised and stabilized. Intensely painful. Not atypical to need preop multimodal analgesia, substantial intraoperative narcotics, then PCA postop. Complications: great vessel, cardiac, or pulmonary injury. Pericardial or pleural effusion. Pneumothorax.
open significantly increases postop pain. Consent all laparoscopic procedure patients for a regional anesthetic, no matter the age. All truncal nerve blocks performed in adults can be performed in children. Care, however, must be taken in calculating amount of local anesthetic delivered. Thoracic, lumbar, and caudal catheters possible. Caudal catheters can be threaded to any vertebral level.
entire kidney is removed along with tumor. Chemotherapy and sometimes radiation follow. Often open, require epidural. 85-90% cure rate. Ureteral reimplantation performed for vesicoureteral reflex. Sometimes done robotically. Caudal usually performed. Neuroblastoma: generally develop in adrenal glands, but can start or spread to chest, spine, or abdomen. Treatment usually surgical unless origin is in spinal cord
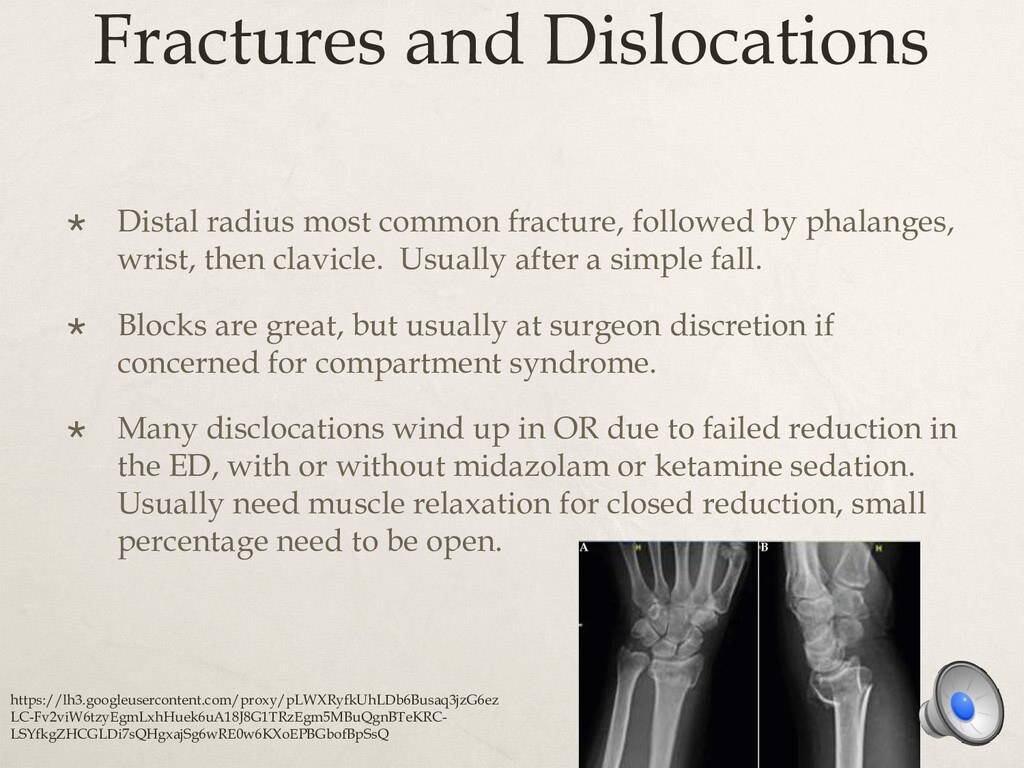
by phalanges, wrist, then clavicle. Usually after a simple fall. Blocks are great, but usually at surgeon discretion if concerned for compartment syndrome. Many disclocations wind up in OR due to failed reduction in the ED, with or without midazolam or ketamine sedation. Usually need muscle relaxation for closed reduction, small percentage need to be open. https://lh3.googleusercontent.com/proxy/pLWXRyfkUhLDb6Busaq3jzG6ez LC-Fv2viW6tzyEgmLxhHuek6uA18J8G1TRzEgm5MBuQgnBTeKRC- LSYfkgZHCGLDi7sQHgxajSg6wRE0w6KXoEPBGbofBpSsQ
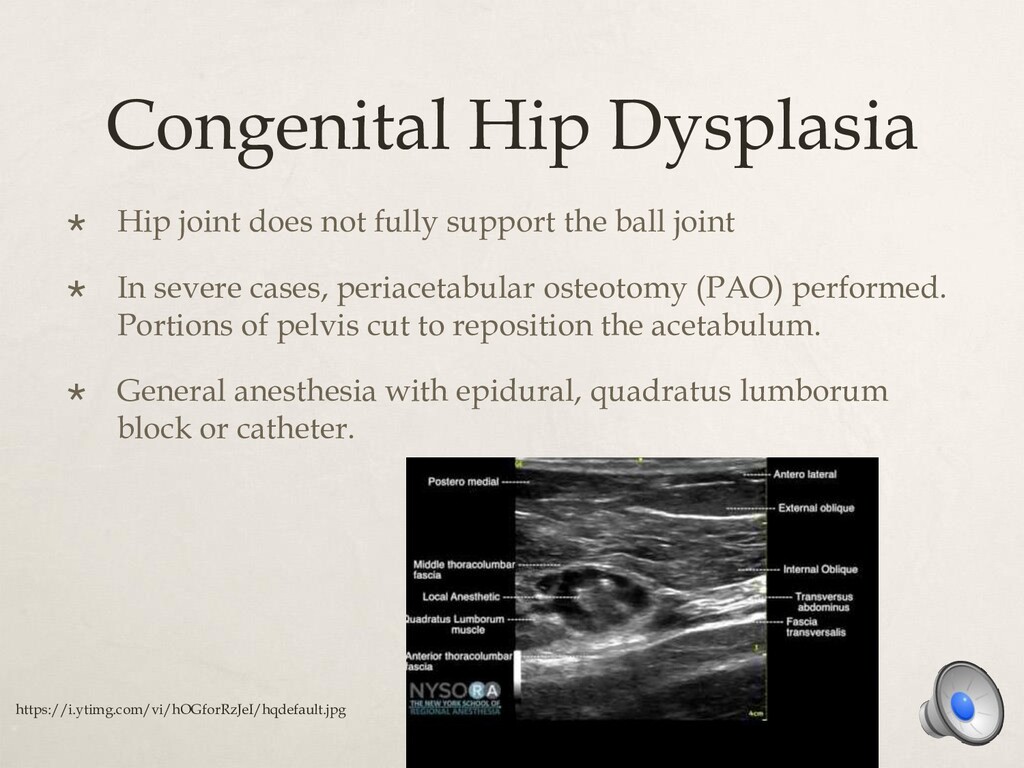
the ball joint In severe cases, periacetabular osteotomy (PAO) performed. Portions of pelvis cut to reposition the acetabulum. General anesthesia with epidural, quadratus lumborum block or catheter. https://i.ytimg.com/vi/hOGforRzJeI/hqdefault.jpg
can cause thoracic insufficiency, impaired lung development, and consequently pulmonary hypertension Surgical options: posterior spinal fusion (most common) and vertical expandable prosthetic rib Long, painful procedures with potential for blood loss, hemodynamic instability, positioning injury, pneumothorax Postoperative vision loss uncommon but devastating Anesthetic: General, prone positioning, arterial line and large bore access, maintenance with TIVA due to neuromonitoring. Multimodal analgesia with IT morphine/PO gabapentin, etc becoming more common
Relatively straightforward – beware oculocardiac reflex and high incidence of PO(N)V Oculocardiac reflex aka trigeminovagal reflex – decrease in HR by 20% or more after globe pressure or extraocular traction. Can even cause cardiac arrest. Decreases with age. Pathway: stretch receptors->ciliary nerves->ciliary ganglion->V1 nerve->Gasserian ganglion->trigeminal nucleus->CNS->Vagus nerve->myocardium->SA node Retro and peribulbar block can decrease OCR occurrence
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}