Presented at the OSEHRA Summit 2014, this talk focused on:
* OSEHRA is major business opportunity for ISVs and systems integrators
* Open source software and associated business models can satisfy most needs.
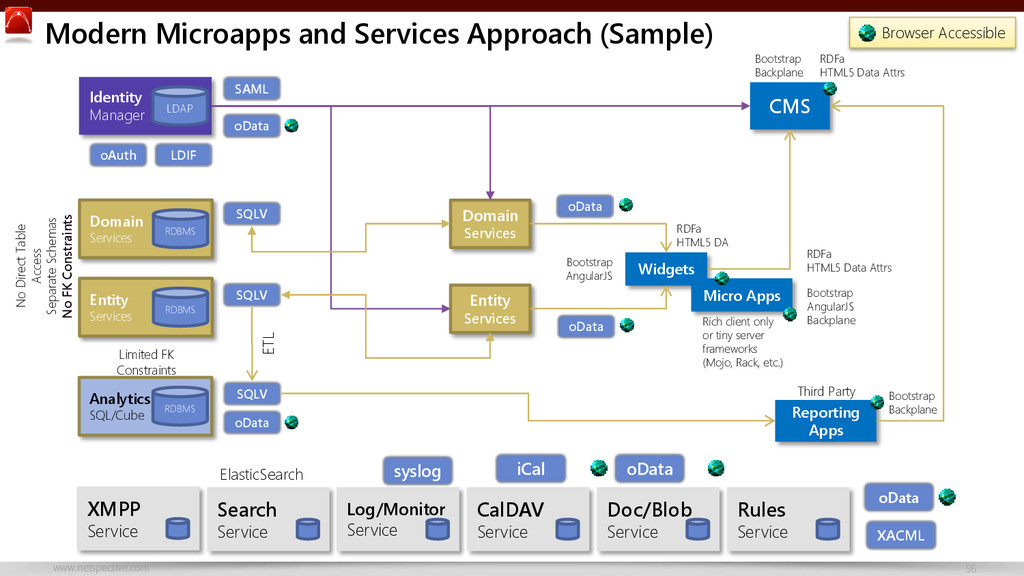
* There’s nothing special about health IT data that justifies complex, expensive, or special technology.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Thank You Visit http://www.netspective.com http://www.healthcareguy.com E-mail [email protected] Follow @ShahidNShah Call](https://files.speakerdeck.com/presentations/04a5b35015a7013267740a3cf862c9b8/slide_58.jpg){kind=link}