the following statements is MOST likely true? A) The use of epinephrine has NOT been shown to be effective as a marker of intravascular injection B) LAST is common in lower extremity peripheral nerve blocks (5% incidence) C) The use of ultrasound guidance rather than nerve stimulation, alone, reduces the incidence of LAST by 65% D) Cardiac arrest as a result of LAST should be treated with epinephrine 1 mg doses of epinephrine during ACLS
nerve blocks Has been shown to be reduced when ultrasound is used rather than nerve stimulation alone Epinephrine is useful as an intravascular injection marker Epinephrine dosing should be less than the dosing in regular ACLS protocols Treatment is with Intralipid (20% lipid emulsion) Dose is 1.5 mL/kg over one minute Subsequent infusion at 15 mL/kg/hour
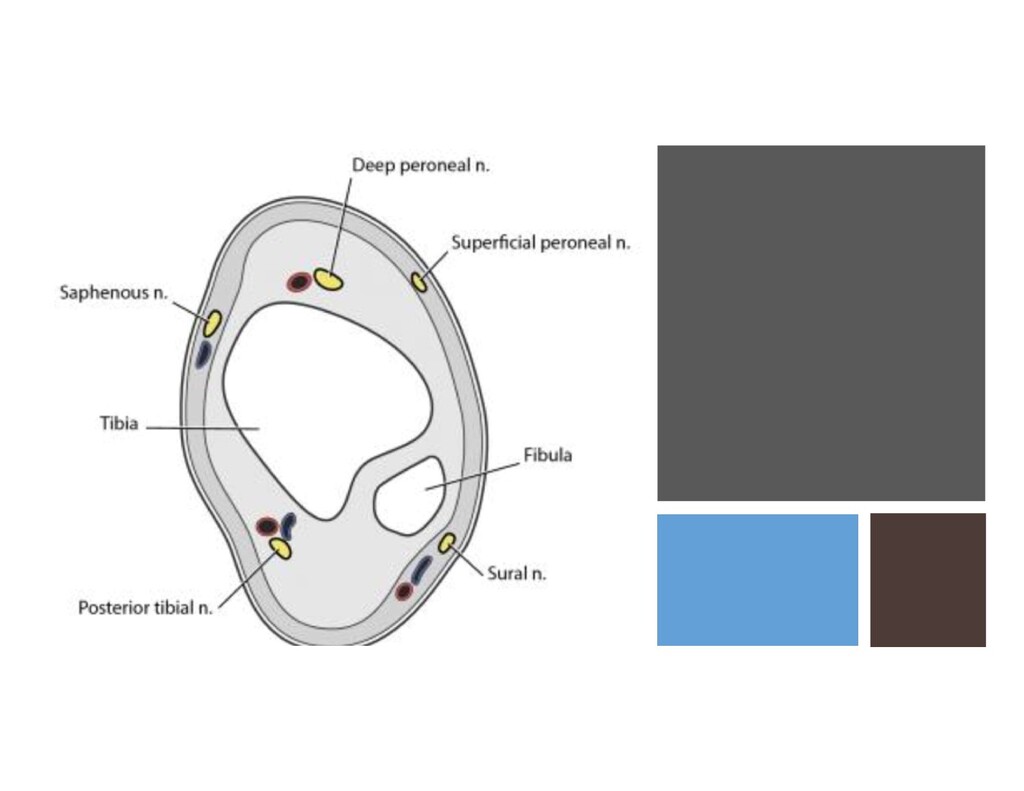
blood vessel used as a landmark for the block? A) Deep Peroneal Nerve / Dorsalis Pedis Artery B) Tibial Nerve / Great Saphenous Vein C) Superficial Peroneal Nerve / Posterior Tibial Artery D) Sural Nerve / Anterior Tibial Artery
and suffers a comminuted left femur fracture. He goes in for ORIF of the femur. A few minutes after induction there is a minimal drop in EtCO2, he is tachycardic (120 bpm) hypotensive (80 mmHg) and is SpO2 92%. What is the next best step in management? A) Place patient in head down, left lateral decubitus position B) Administer TXA C) Obtain emergent TEE D) Release tourniquet
PE ABG is essentially useless (will show hypoxemia + respiratory alkalosis in awake patient due to hyperventilation) S1Q3T3 in <20% of cases Sudden drop in EtCO2 represents dead space TEE = right heart strain if large enough Fat Embolism Major criteria = respiratory insufficiency, cerebral involvement, petechial rash Minor criteria = tachycardia, fever, jaundice, retinal change, renal change Labs = Microglobulinemia (REQUIRED) anemia, thrombocytopenia
central catheter (PICC) which of the following is most correct regarding potential vein choices? • A) The saphenous vein is avoided in children who are not ambulatory • B) The median nerve can be injured when the brachial vein is cannulated • C) The basilic vein is more prone to vasospasm than the cephalic vein • D) The subclavian vein can be used without risk of dramatic complication
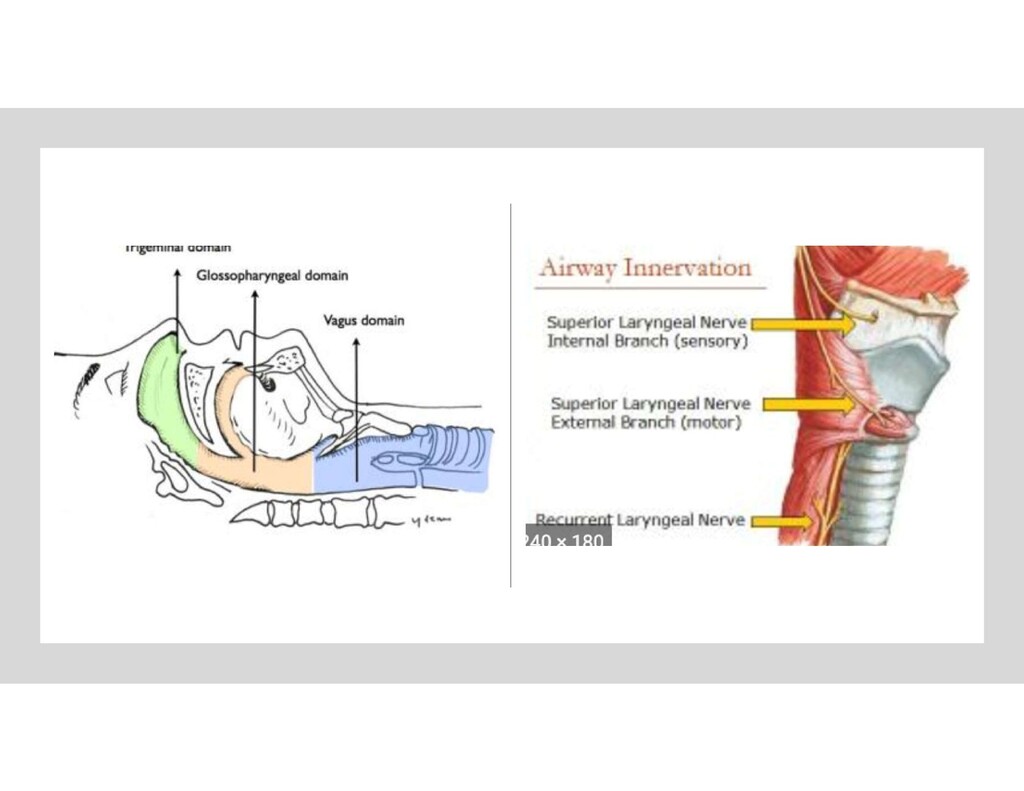
of the airway with its nervous innervation? • A) oropharynx to epiglottis – glossopharyngeal nerve • B) anterior 2/3 of the tongue – glossopharyngeal nerve • C) Epiglottis to vocal cords – recurrent laryngeal nerve • D) Nasopharynx – facial nerve
but NOT diazepam? • A) peripheral vasodilation • B) reversal by flumazenil • C) Facilitation of GABA binding by allosteric modulation • D) Chemical structure change to lipophilic at physiologic pH
contributes to its rapid onset of action Flumazenil is a competitive antagonist for all benzodiazepines All benzodiazepines work through allosteric modulation of GABA (enhance the action of GABA binding Both can cause some degree of peripheral vasodilation
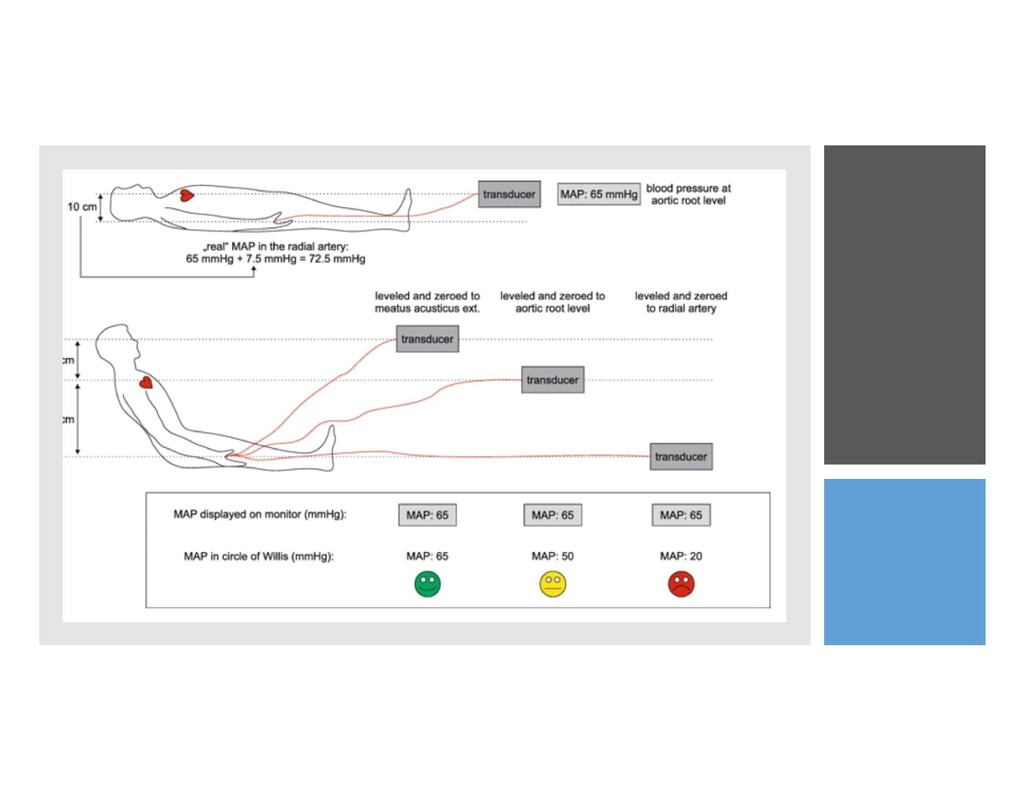
set-up of an arterial line? • A) The system should be leveled 5 cm posterior to the sternum • B) Leveling and zeroing the transducer are the same procedure • C) A transducer leveled 10 cm higher than the appropriate target position will overestimate the pressure by 7.4 mmHg • D) A transducer should be leveled by opening the system to air
is more ACIDEMIC than mother (B becomes BH+) Charged molecule cannot pass back into mother Becomes “trapped” in placenta Chlorprocaine is rapidly hydrolyzed and very little agent crosses the placenta
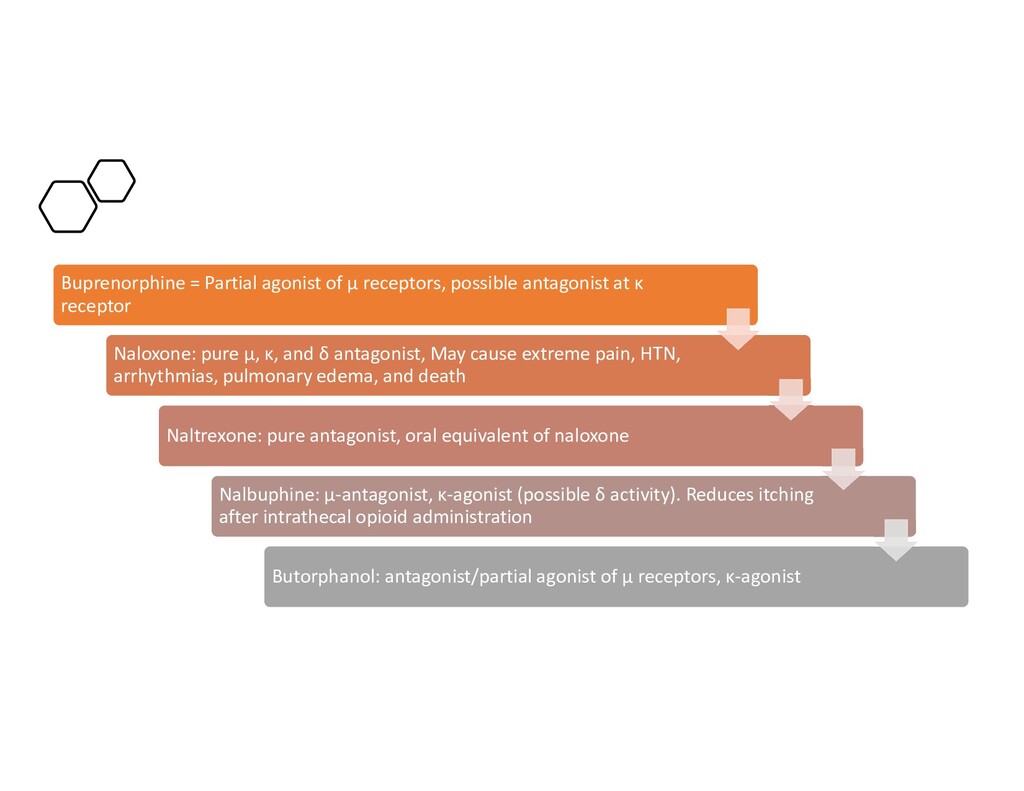
κ receptor Naloxone: pure μ, κ, and δ antagonist, May cause extreme pain, HTN, arrhythmias, pulmonary edema, and death Naltrexone: pure antagonist, oral equivalent of naloxone Nalbuphine: μ-antagonist, κ-agonist (possible δ activity). Reduces itching after intrathecal opioid administration Butorphanol: antagonist/partial agonist of μ receptors, κ-agonist
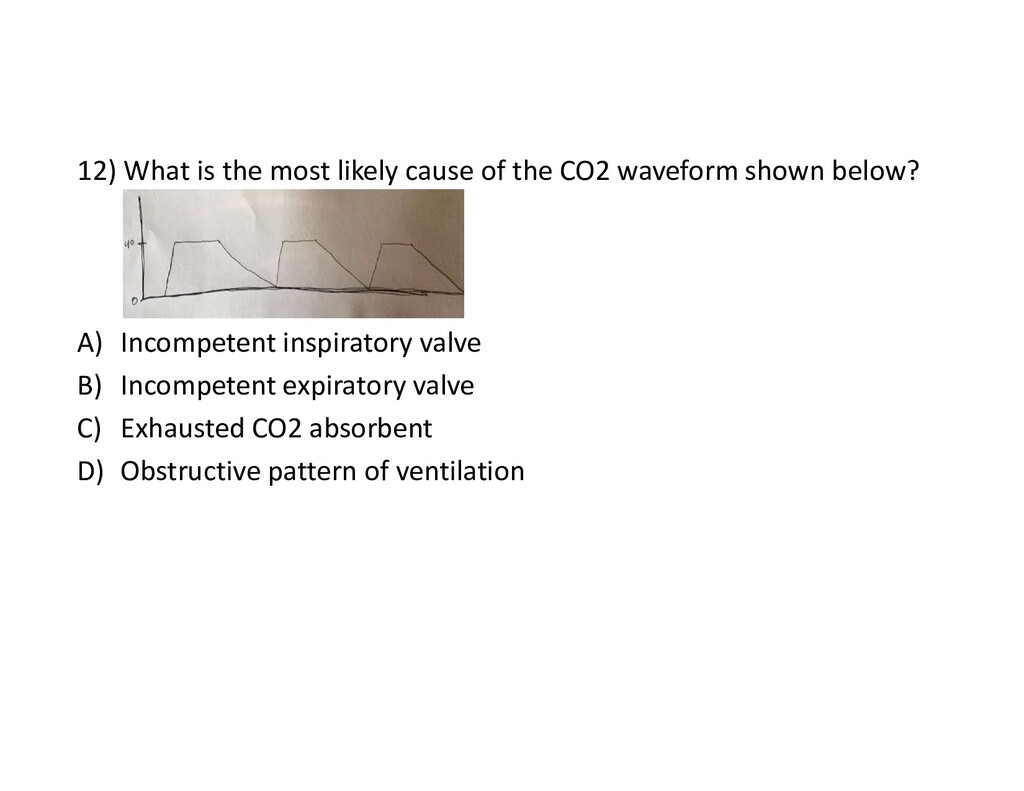
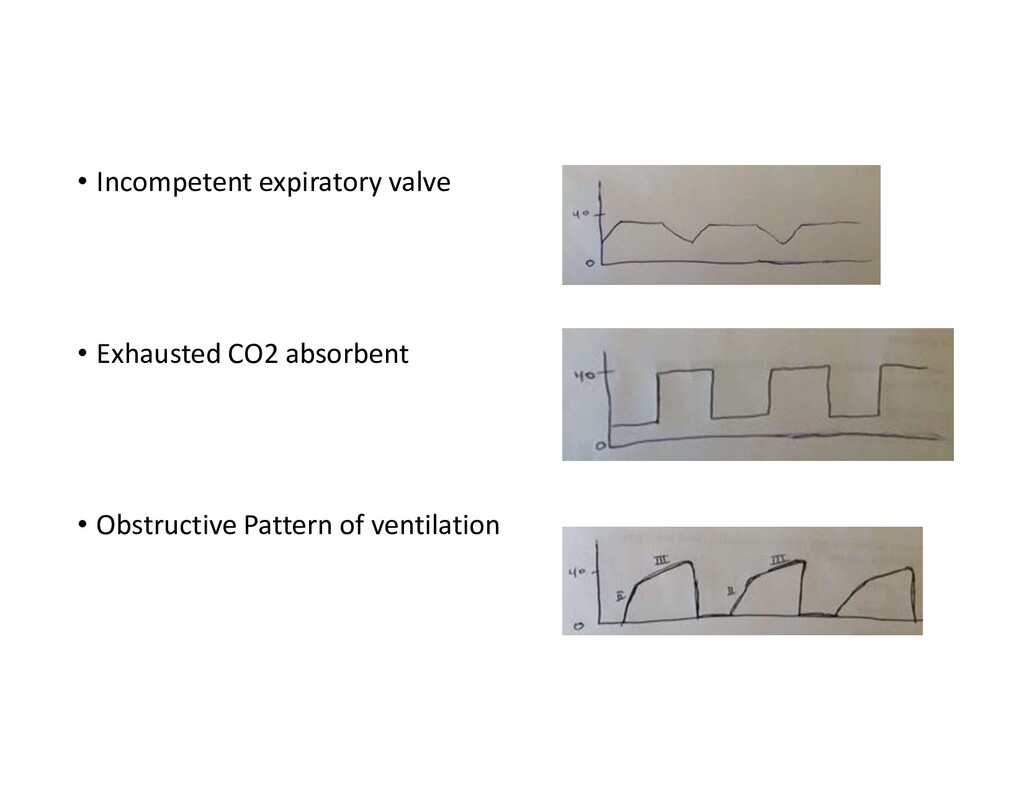
waveform shown below? A) Incompetent inspiratory valve B) Incompetent expiratory valve C) Exhausted CO2 absorbent D) Obstructive pattern of ventilation
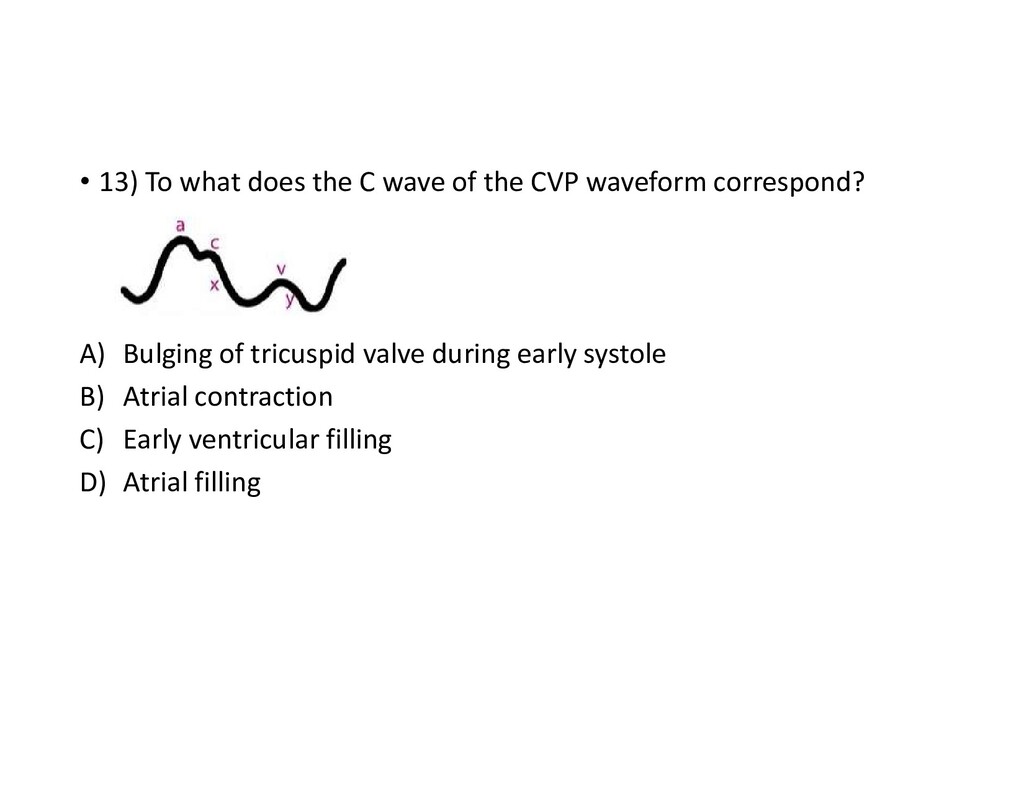
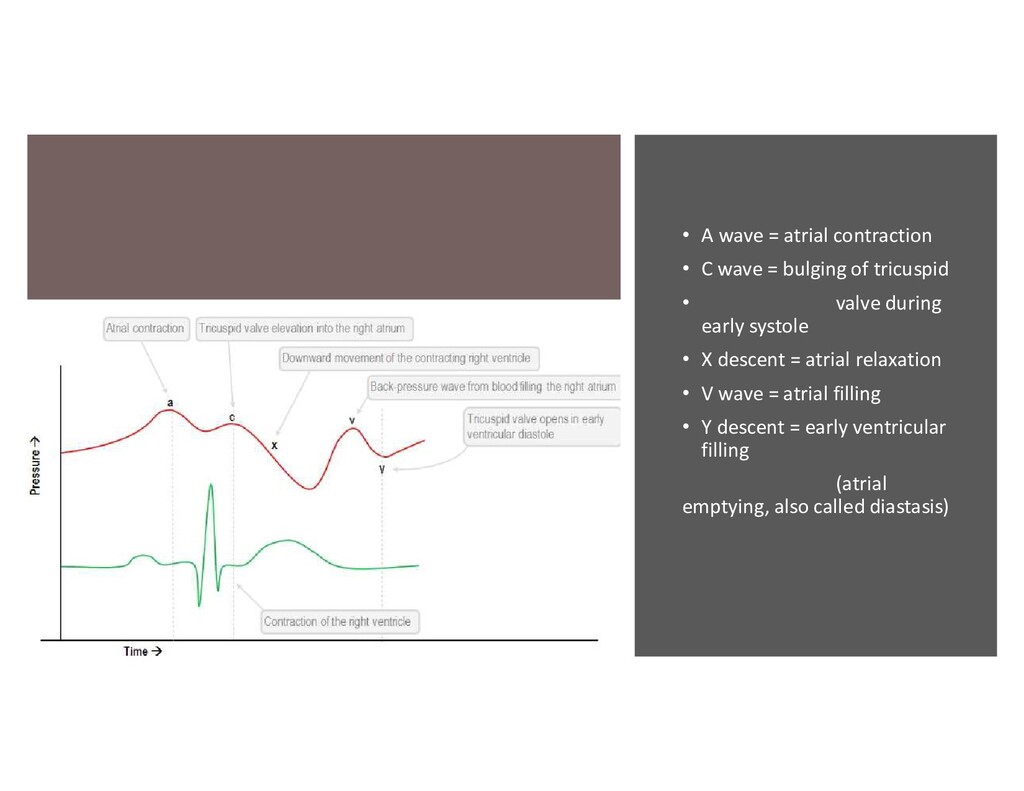
bulging of tricuspid • valve during early systole • X descent = atrial relaxation • V wave = atrial filling • Y descent = early ventricular filling (atrial emptying, also called diastasis)
is having microlaryngeal surgery with CO2 laser. He is under general endotracheal anesthesia with sevoflurane for maintenance. As the surgery begins the ENT surgeon notifies you that a fire has ignited in the airway. What is the first action that should be taken in the situation? A) saline should be poured down the endotracheal tube B) Discontinue volatile agent and nitrous oxide started for maintenance of anesthesia C) activate the OR fire alarm D) extubate the patient and stop all fresh gas flows
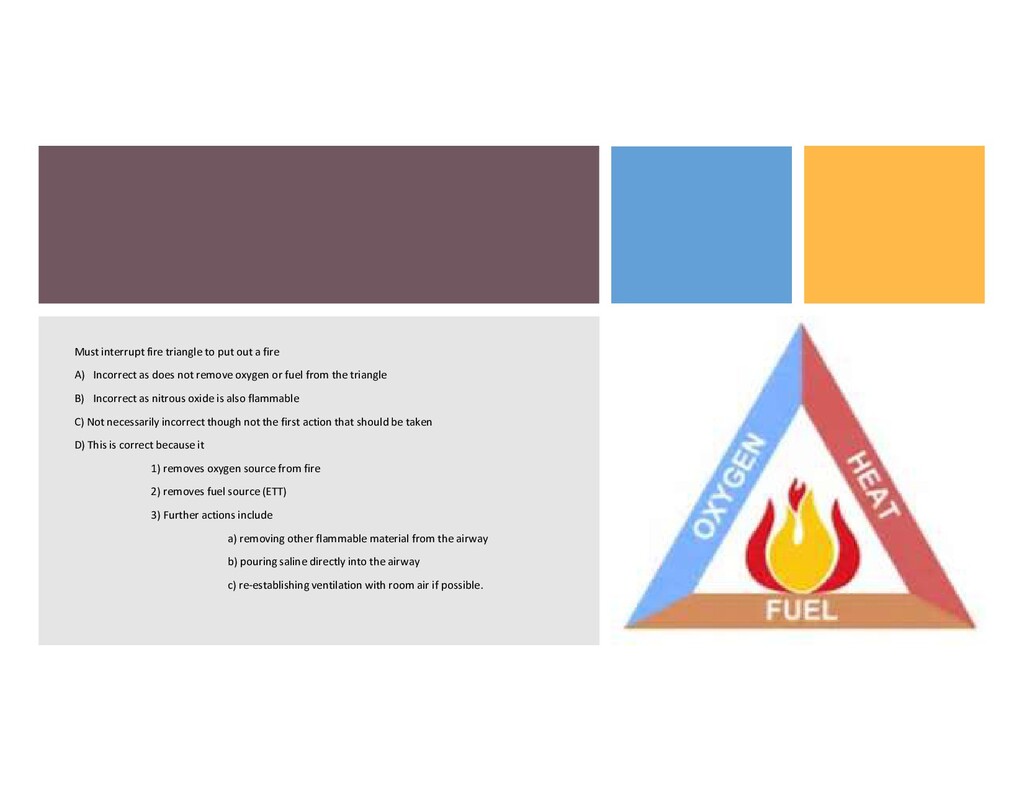
Incorrect as does not remove oxygen or fuel from the triangle B) Incorrect as nitrous oxide is also flammable C) Not necessarily incorrect though not the first action that should be taken D) This is correct because it 1) removes oxygen source from fire 2) removes fuel source (ETT) 3) Further actions include a) removing other flammable material from the airway b) pouring saline directly into the airway c) re-establishing ventilation with room air if possible.
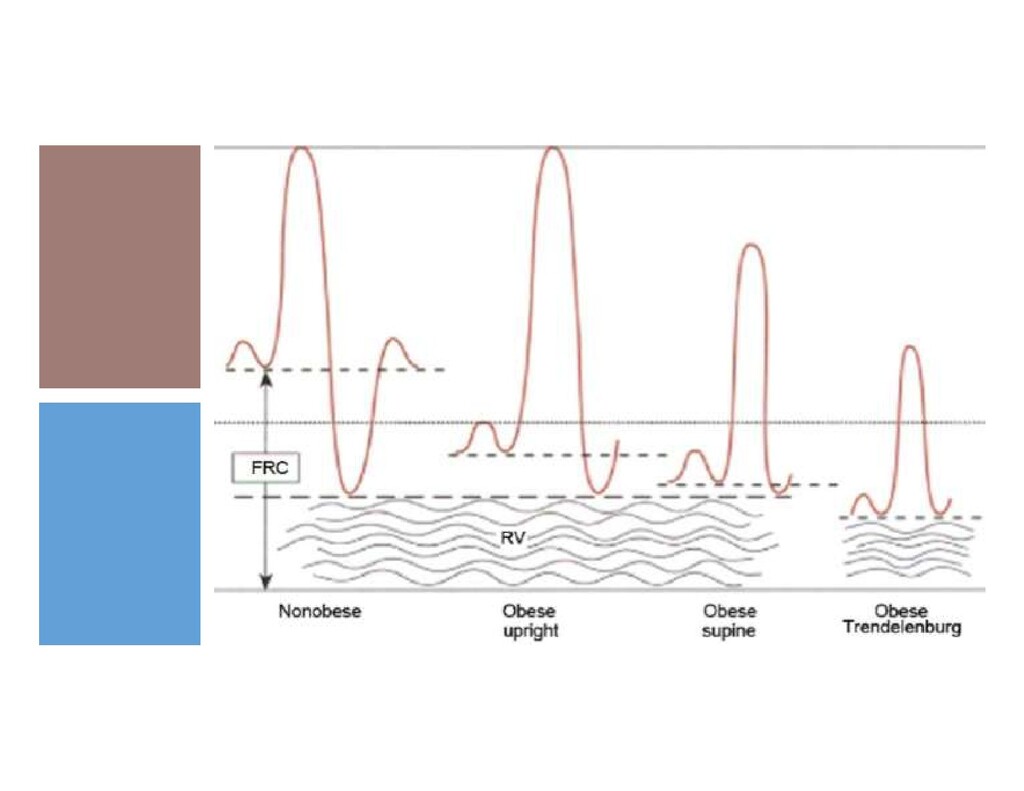
laparoscopic gastric sleeve procedure. How will the respiratory mechanics of this patient differ from the respiratory mechanics of a patient of ideal body weight? A) FRC is decreased due to decreased residual volume B) FRC is decreased due to decreased expiratory reserve volume C) Closing capacity is decreased D) Obstructive ventilation pattern is seen
and charge characteristics is MOST likely to be filtered in the glomerulus (renal corpuscle)? A) Large, negative B) Large, positive C) Small, negative D) Small, positive
pass from blood through the glomerular barrier into the glomerulus. Small molecules are more able to pass the barrier as are molecules that are positively charged. The following figure illustrates this.
The more significant the diastolic dysfunction, the more reliant the heart is on the atrial kick for filling. • Mitral regurgitation = not dependent on atrial kick as large proportion of blood returns to atrium and fills passively • Mitral stenosis = hemodynamic collapse can be seen due to fixed obstruction and decreased filling, atrial kick cannot necessarily overcome the fixed obstruction
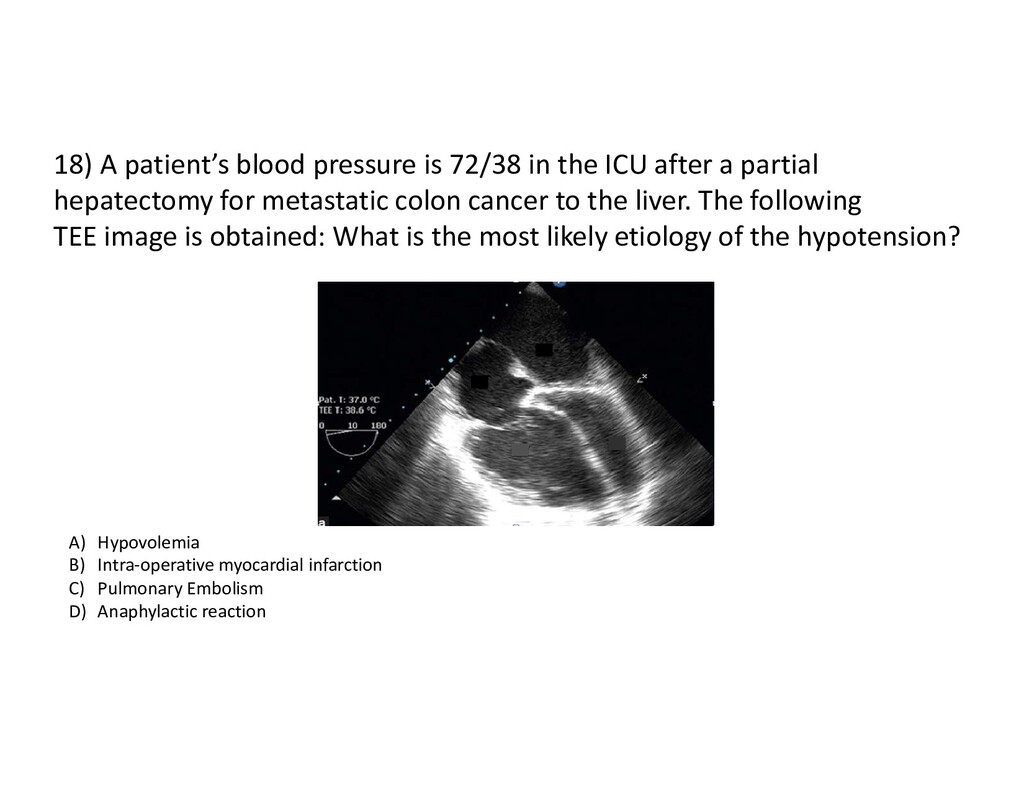
after a partial hepatectomy for metastatic colon cancer to the liver. The following TEE image is obtained: What is the most likely etiology of the hypotension? A) Hypovolemia B) Intra-operative myocardial infarction C) Pulmonary Embolism D) Anaphylactic reaction
ventricle is dilated and the left ventricle is underfilled This represents increased right sided (pulmonary) pressures most consistent with pulmonary embolism
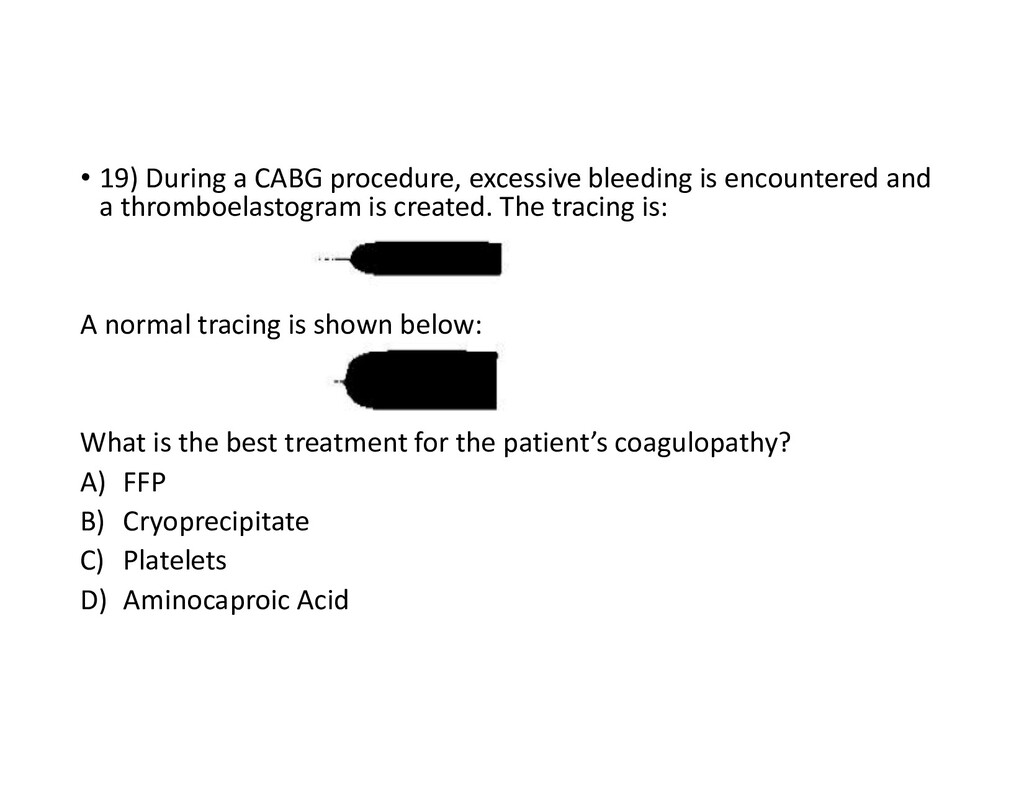
and a thromboelastogram is created. The tracing is: A normal tracing is shown below: What is the best treatment for the patient’s coagulopathy? A) FFP B) Cryoprecipitate C) Platelets D) Aminocaproic Acid
pin and torsion wire mechanism applied while the cuvette oscillates and the blood clots. A recording of the signal from the torsion wire is generated and a graphical representation created • R = reaction time • 0 to the beginning of clot formation • Measures intrinsic and extrinsic clotting pathways • Long R time is generally treated with factors (FFP) • K = coagulation time • 2mm amplitude to 20 mm amplitude • Relies on fibrinogen • Slow = treatment with cryoprecipitate • Similar to angle
at the highest point • Indicates clot strength • Treatment for low MA with platelets • Clot lysis (LY30) • The amount of clot that has been broken down at 30 minutes • Generally more than 3% indicates treatment • Antifibrinolytic such as Aminocaproic acid or TXA
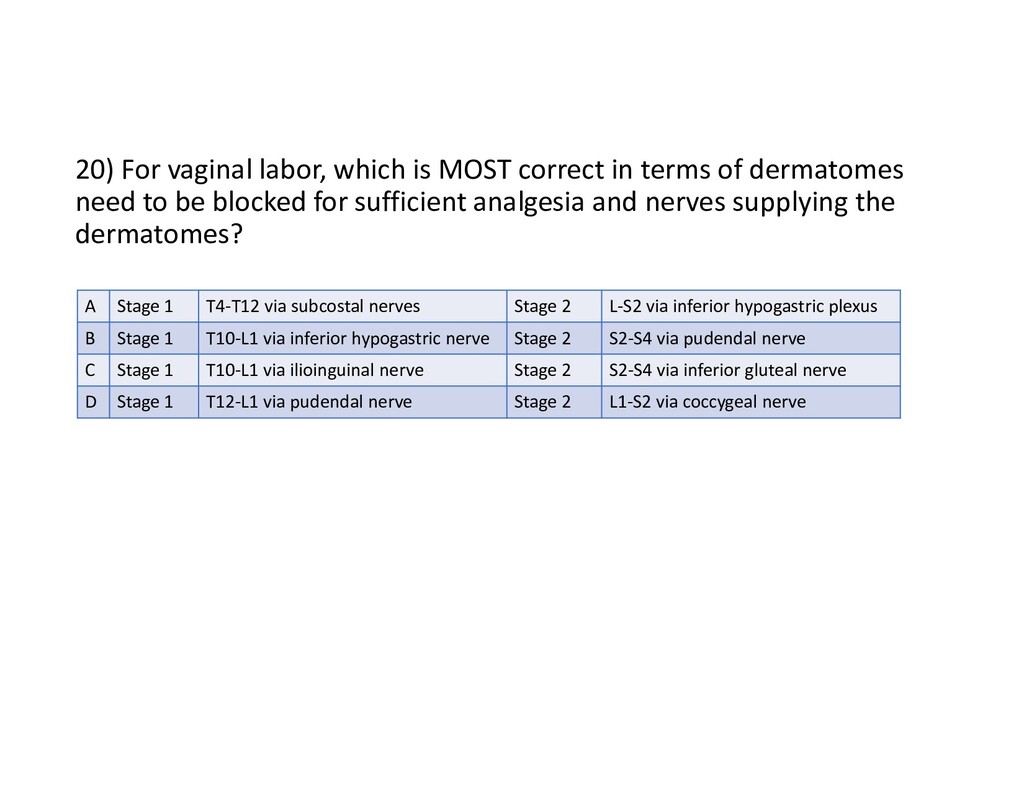
of dermatomes need to be blocked for sufficient analgesia and nerves supplying the dermatomes? A Stage 1 T4-T12 via subcostal nerves Stage 2 L-S2 via inferior hypogastric plexus B Stage 1 T10-L1 via inferior hypogastric nerve Stage 2 S2-S4 via pudendal nerve C Stage 1 T10-L1 via ilioinguinal nerve Stage 2 S2-S4 via inferior gluteal nerve D Stage 1 T12-L1 via pudendal nerve Stage 2 L1-S2 via coccygeal nerve
inferior hypogastric plexus on the way to the sympathetic chain) that originate from the T10-L1 segments of the spinal cord (referred to the back as well as abdominal wall) First Stage: • Pain for the second stage is transmitted via the pudendal nerve (S2-4) Second Stage:
aortic aneurysm undergoes uneventful aneurysm repair. He returns to the ICU on norepinephrine and epinephrine infusions. Over the next hour, his vasopressin requirements increase. His chest tube output has slowed significantly and he has received multiple fluid boluses. You suspect cardiac tamponade. A CVP tracing with which of the following findings would best support this diagnosis? A) An attenuated x descent and y descent B) An attenuated x descent with exaggerated y descent C) An exaggerated x descent and y descent D) An exaggerated x descent with attenuated y descent
y descent • X-descent represents atrial relaxation during ventricular systole. At this time pericardial pressure becomes a little negative (ventricle contracts so space in the pericardium increases relative to what it was before) which momentarily lessens the tamponade • Since the pericardial pressure is relatively negative than what it was before, more blood is drawn into the ventricle than it otherwise would have been and a large x-wave occurs • Y-descent represents early ventricular filling which is obliterated by the tamponade
with anesthetic levels up to T5. Which of the following nerves should be blocked for a transurethral resection of a lateral wall bladder tumor? • A) no further blocks are necessary • B) femoral block • C) sciatic block • D) obturator nerve block
from L3 and L4 with minor input from L2 • Selective obturator block can help to prevent obturator nerve spasm as it courses near the bladder • Block of this nerve can help prevent adductor muscle spasm which may lead to bladder wall perforation, vessel laceration, incomplete tumor resection or hematomas
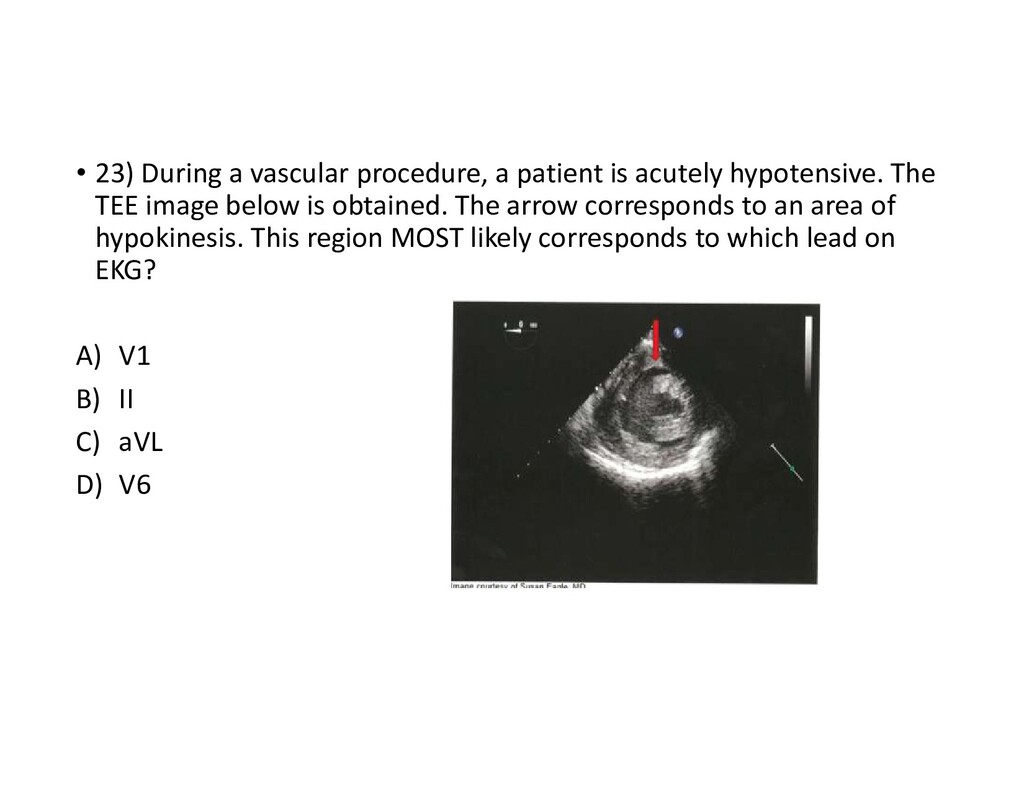
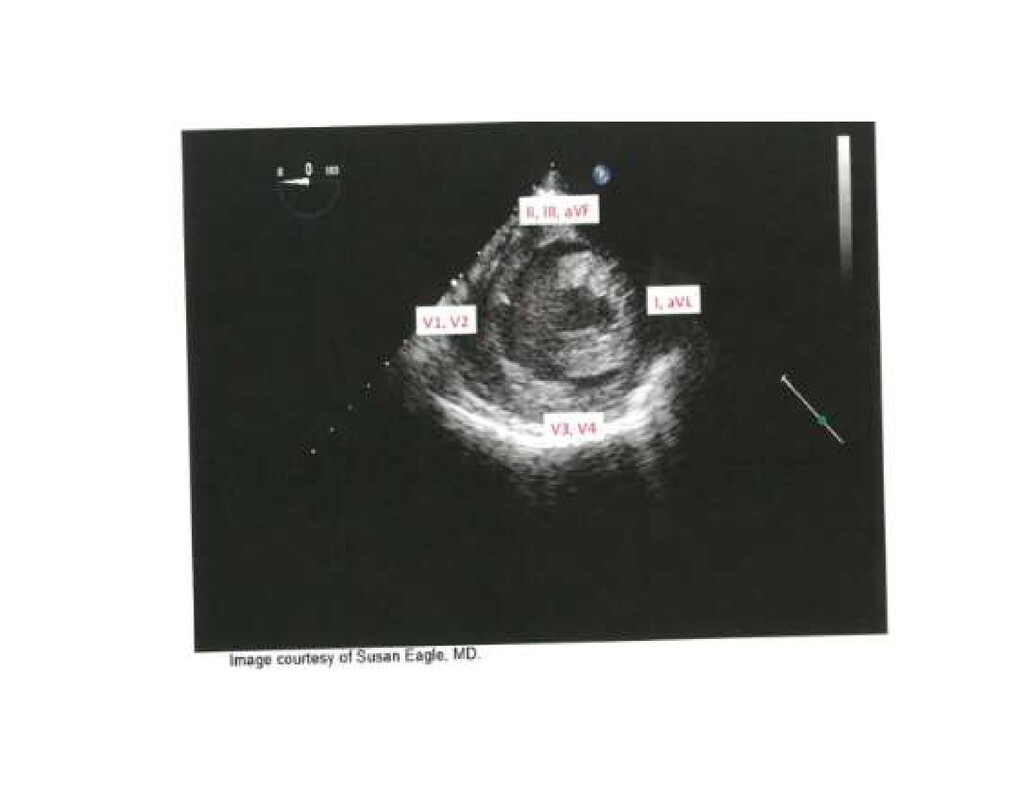
hypotensive. The TEE image below is obtained. The arrow corresponds to an area of hypokinesis. This region MOST likely corresponds to which lead on EKG? A) V1 B) II C) aVL D) V6
contractility and tachycardia. This leads to a high cardiac output scenario. This combination can lead to myocardia ischemia if left untreated. • Supraventricular dysrhythmias can occur in up to 15% of people with hyperthyroidism and this can increase up to 40% with increasing age • Pericardial effusion is most common in hypothyroidism and rare in hyperthyroidism
during a motorcycle accident. Which of the following manifestations is LEAST likely following a cervical spine injury? A) Left ventricular dysfunction B) Bradycardia C) Hypertension D) Pulmonary edema
trauma which leads to • LV dysfunction (or Takotsubo cardiomyopathy) • Bradycardia • Pulmonary edema • LV dysfunction • Neurogenic causes • Loss of sympathetic stimulation below the level of the injury can result in decreased peripheral vascular resistance and hypotension (Spinal Shock)
to be seen in an infant also with congenital tracheoesophageal fistula? A) Limb defects B) Cardiac abnormalities C) Anal atresia D) Renal abnormalities
fistula • Renal anomalies • Limb anomalies Of the associated congenital anomalies, the most common is grouped into the VACTERL association • 35% also have cardiac abnormalities • 25% have GI abnormalites (including anal atresia) • 10% renal • 10% vertebral • 10% limb In infants with TEF:
the anterior pituitary • Multisystem disorder resulting in • DM 2 • Macroglossia • Hypertrichosis • Arthritis • Hypertension • Hypertriglyceridemia • Uncontrolled HTN can lead to hypertrophy, increased cardiac mass and fibrosis leading diastolic heart failure • Cervical spine instability is not associated with acromegaly.
likely remain the same in a patient with ALS? A) Forced vital capacity (FVC) B) Forced expiratory volume in 1 sec. (FEV1) C) The ratio of FEV1/FVC D) Total Lung Capacity (TLC)
lower motor neurons. Pulmonary function testing follows a restrictive pattern • Decreased • Forced vital capacity FEV1 is decreased • Total lung capacity is decreased • Inspiratory and expiratory mouth pressure is decreased (bulbar weakness) • No Change • FEV1/FVC • Sleep disordered breathing is common
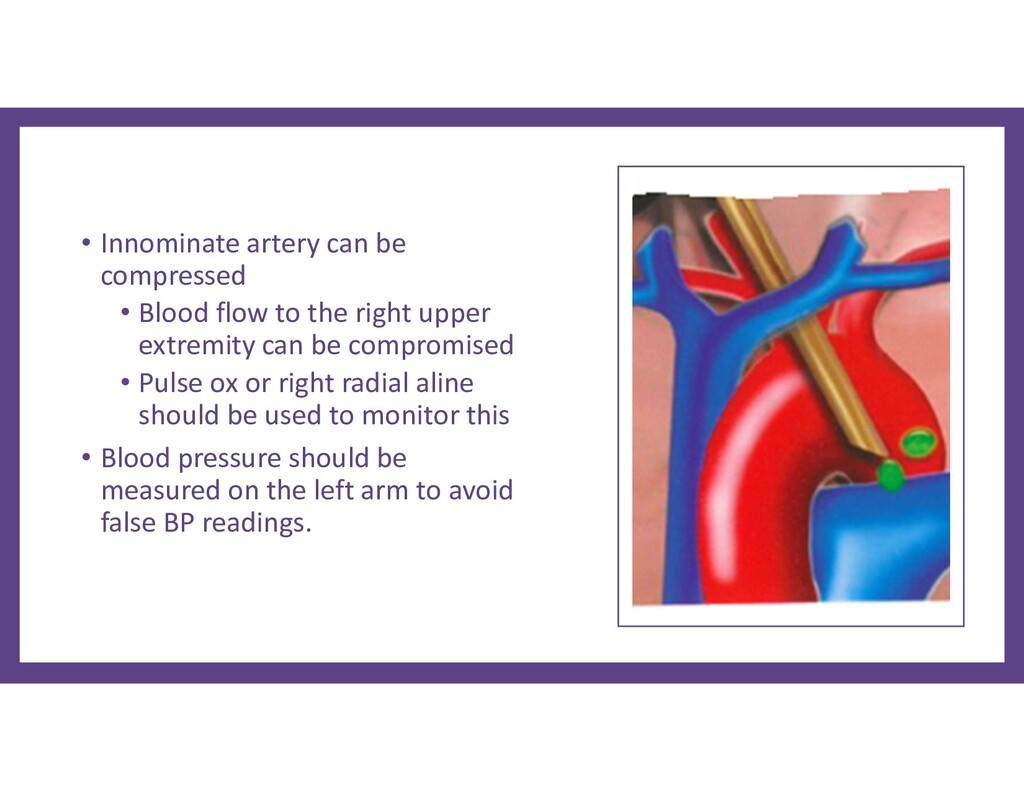
the right upper extremity can be compromised • Pulse ox or right radial aline should be used to monitor this • Blood pressure should be measured on the left arm to avoid false BP readings.
resection of a small frontal tumor is MOST likely to result in transient: A) Increase in intracranial pressure B) Decrease in central venous pressure C) Increase in sodium concentration D) Decrease in serum osmolality
an osmolality of 1098 mOsm at doses up to 1 g/kg. It reduces brain swelling and decreases brain volume, enabling the neurosurgeon to obtain better exposure without excessive retractor pressure. Administration should take place 30 minutes prior to dural opening, and a brisk response in urine output should be noted. • The large osmotic load from a standard dose of mannitol results in • a mild increase in serum osmolality • a transient increase in central venous pressure (CVP) (Figure 1) • a transient increase in intracranial pressure (ICP), possibly due to vasodilation of cerebral vessels in response to the increased osmolality (Figure 2) • no change or a mild decrease in serum sodium and bicarbonate due to osmotic expansion of the extracellular volume.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}