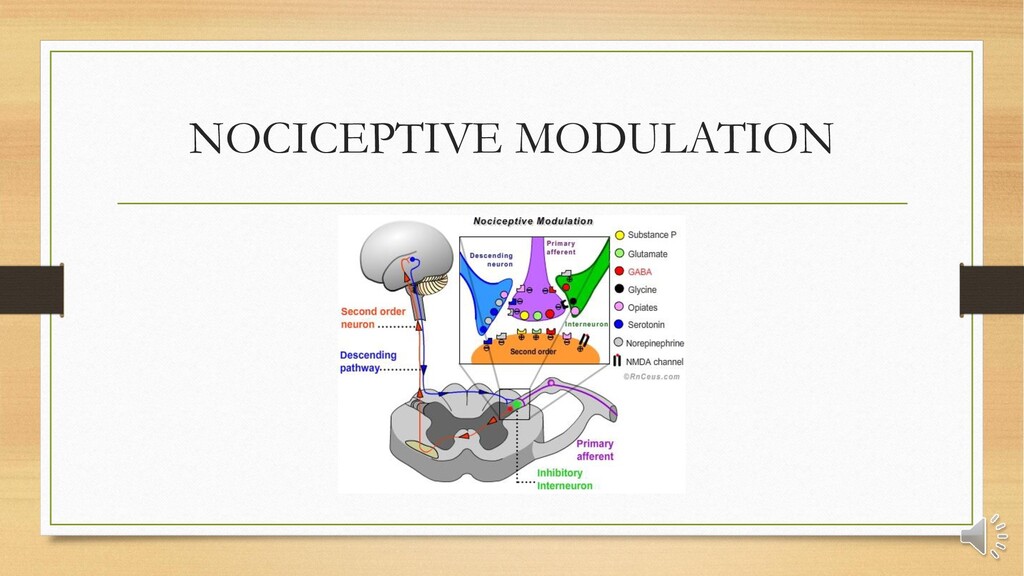
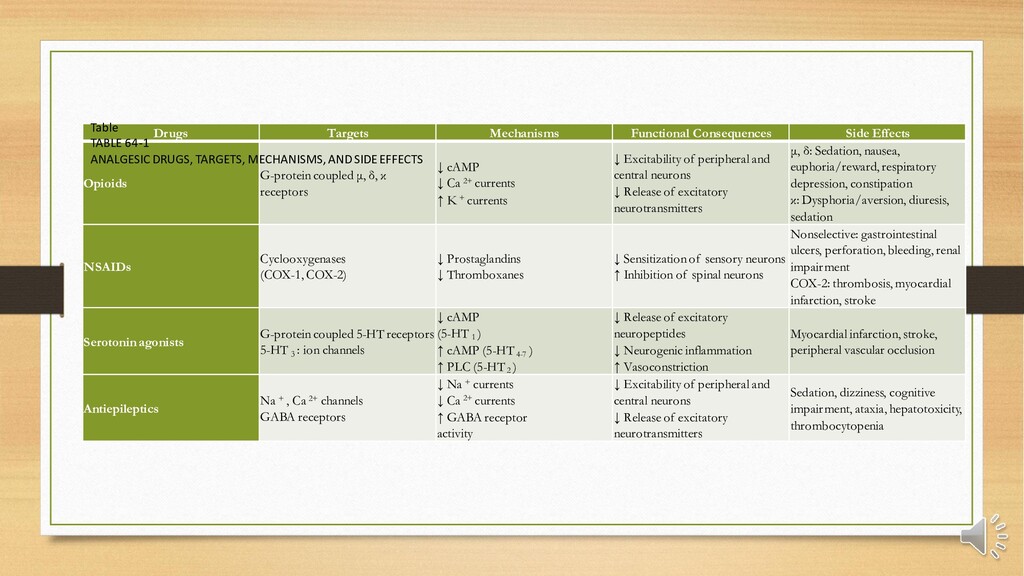
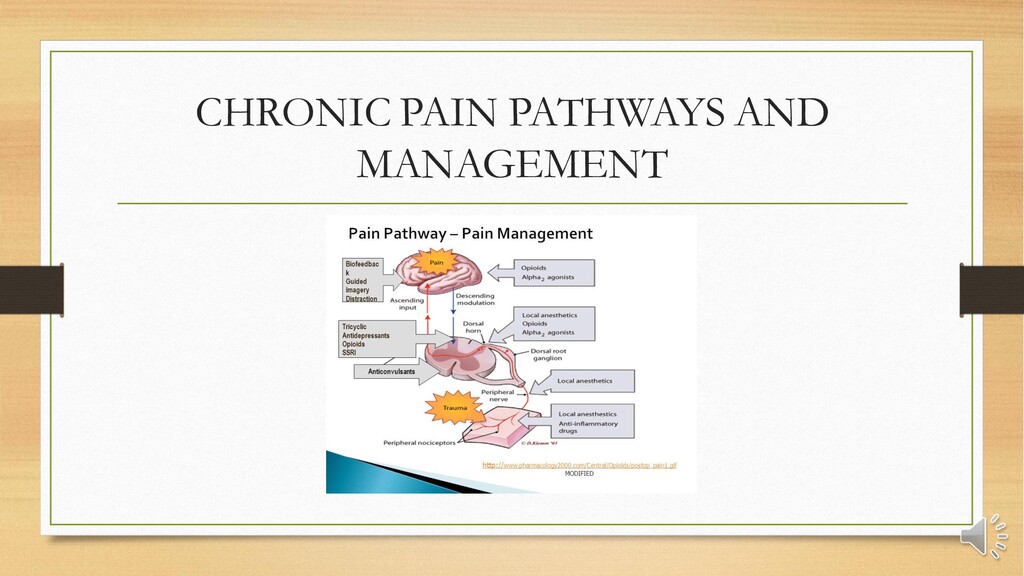
and ion channels, is altered by persistent pain. • Because of the large number of sources and manifestation of chronic pain, classification must include cancer-related, neuropathic, inflammatory, arthritis, and musculoskeletal pain • Interdisciplinary management of chronic pain must include specialists in psychology, physical therapy, occupational therapy, neurology, and anesthesiology. • Drugs used for chronic pain are multiple and include opioids, nonsteroidal anti- inflammatory drugs and antipyretic analgesics, serotonin receptor ligands, antiepileptic's, antidepressants, topical analgesics (e.g., nonsteroidal anti-inflammatory drugs, capsaicin, local anesthetics, opioids), and adjuvants such as local anesthetics, α 2 -agonists, baclofen, botulinum toxin, antiemetics, novel drugs such as cannabinoids, and ion channel blockers. • Interventional management of chronic pain includes the use of diagnostic blocks, therapeutic blocks, continuous catheter techniques (peripheral, epidural, intrathecal), and stimulation techniques such as acupuncture, transcutaneous electrical nerve stimulation, and spinal cord stimulation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}