President, Capital Facilities & Engineering Beth Israel Deaconess Medical Center Wendy Writer Gettleman Vice President, Facilities Management & Real Estate Dana-Farber Cancer Institute John Messervy, AIA Director of Capital & Facilities Planning Partners HealthCare William R. Seed Staff Vice President, Design & Construction Department Universal Health Services MODERATOR Daniel R. Quinn Executive Vice President, Development & Consulting Services Colliers International
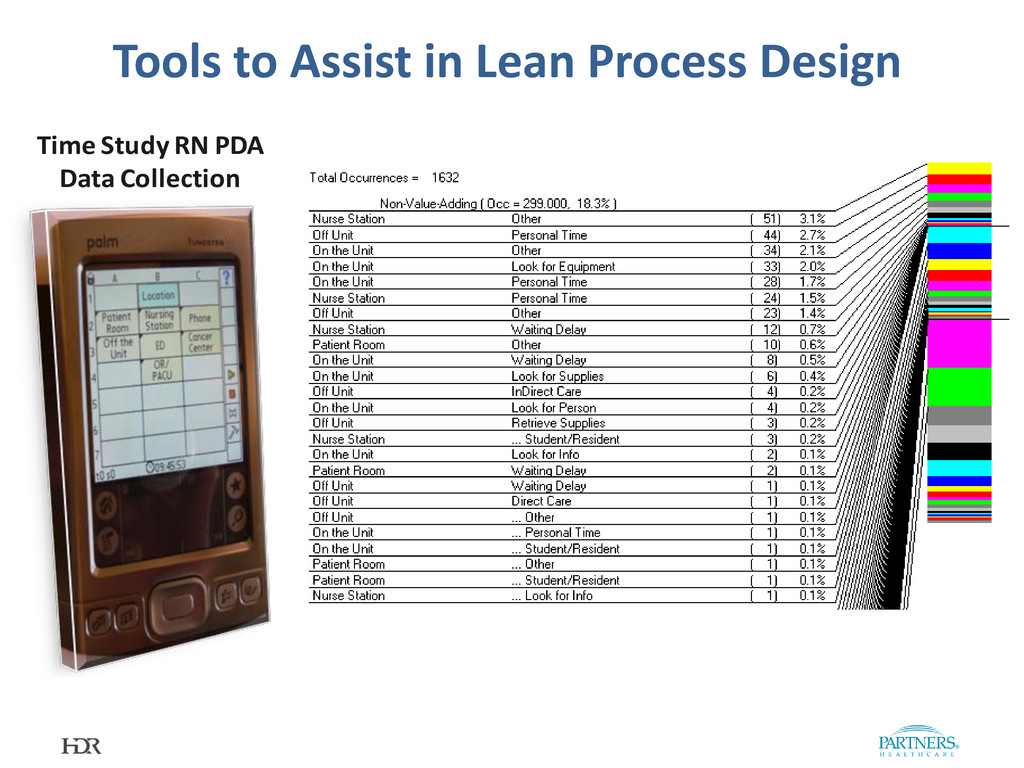
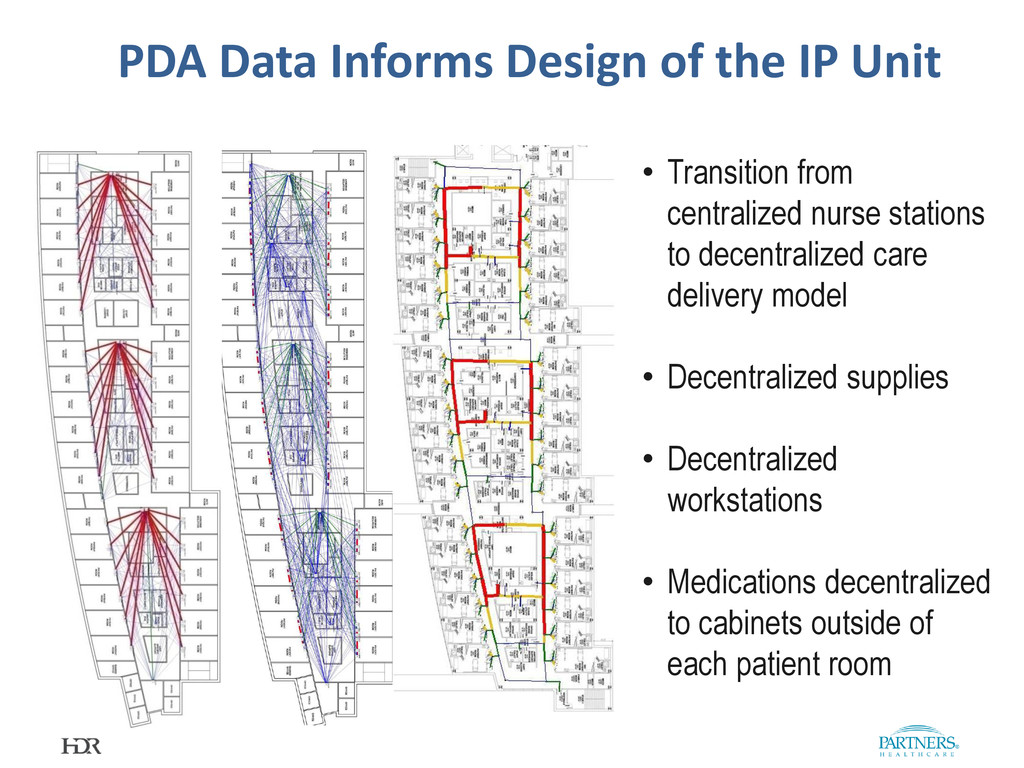
model • Decentralized supplies • Decentralized workstations • Medications decentralized to cabinets outside of each patient room PDA Data Informs Design of the IP Unit
Isolation 5 beds + 1 Isolation 5 beds + 1 Isolation Design Impact on Care Delivery & Functionality 12 Bed Pod 12 Bed Pod 12 Bed Pod 36 beds grouped in 3 clusters of 12 based on hospitalist and nursing staffing models New Lobby below Public Elevators Patient Elevators
agents, etc. • Early and ongoing involvement of key stakeholders • Value engineering, constructability and operability reviews • Design software used to increased construction efficiencies and maintain quality control • Progressive contracting practices • Many more What Does Lean Expertise Bring to Design and Construction that Cannot be Gained by Improved Project Delivery Techniques such as:
Center – expert as part of architectural team • Western Cancer Center – separate contract with the owner, coordinating with other team members and stakeholders Different Placement of Lean Expertise on Design and Construction
walks of current space • Value stream map of current workflows • Work Breakdown Structure • Map IS flow process and document management Sample Lean Exercise: Pharmacy
Arranged full-sized equipment models on full-scale floor layouts • Each team’s layout was video taped and reviewed by all participants • Each team did 3 layouts in sequence followed by group discussions • Consensus reached on equipment layout Sample Lean Exercise: Pharmacy
Involvement of front-line staff • Structuring the input of front-line staff through standard tools and techniques • Understanding and improving the workflow prior to hardened design concepts • Obtaining input from the customer Enhanced Benefits of Lean
Finding Lean experts comfortable in working in the engineering/construction environment with its emphasis on cost and schedule • Finding architectural firms which have integrated operations experts/industrial engineers into their practice • Assisting front-line employees to conceptualize new workflows in new spaces, rather than improving workflows in existing environments Challenges
staff, for patients, families and staff. It all started with our design principles: 1. Promote personalized, multidisciplinary, safe, respectful, compassionate cancer care for patients and families in a healing environment 2. Stimulate translation of research into the care of patients 3. Optimize flexibility and utility of space 4. Streamline the flow of patients and materials, minimize wait and treatment times 5. Foster productivity and collaboration of staff 6. Create a new front entrance and presence
inform design process > 30 design committees & user groups > 300 participants in planning & design process including: Defined decision makers & roles • user groups and committees informed • 2020 group packaged clinical decisions • Steering committee provided recommendations • Leadership Triad made timely decisions • More than 25 MDs • More than 25 RNs • More than 30 patient and family members • More than 250 DF/BWCC employees
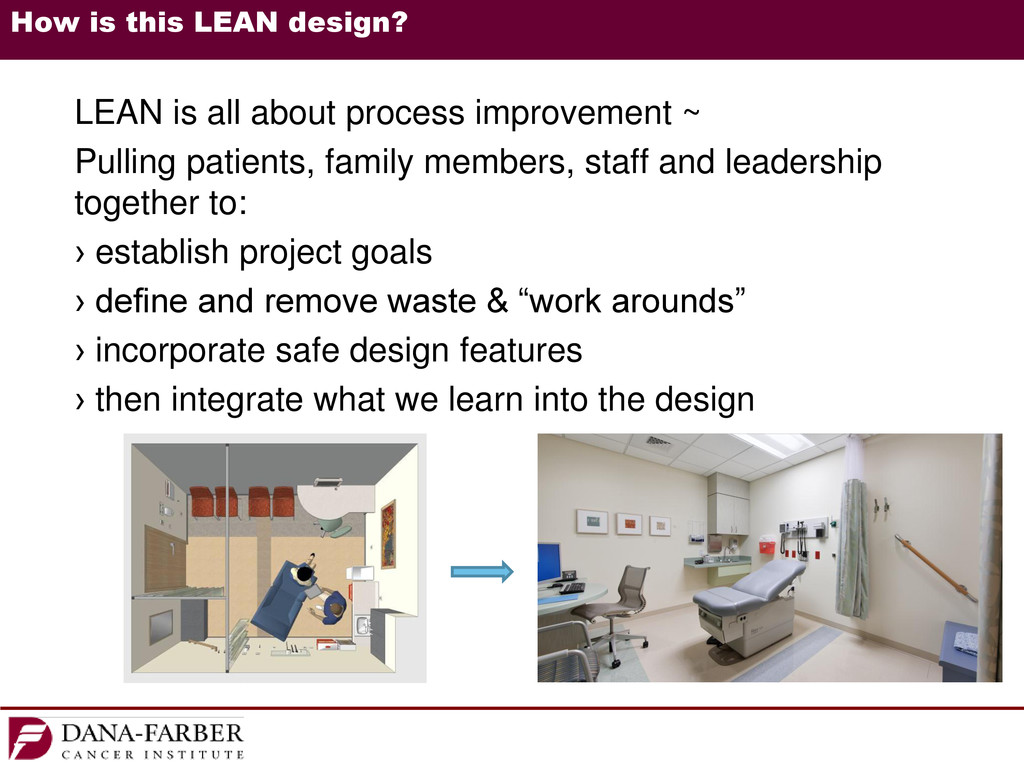
improvement ~ Pulling patients, family members, staff and leadership together to: › establish project goals › define and remove waste & “work arounds” › incorporate safe design features › then integrate what we learn into the design
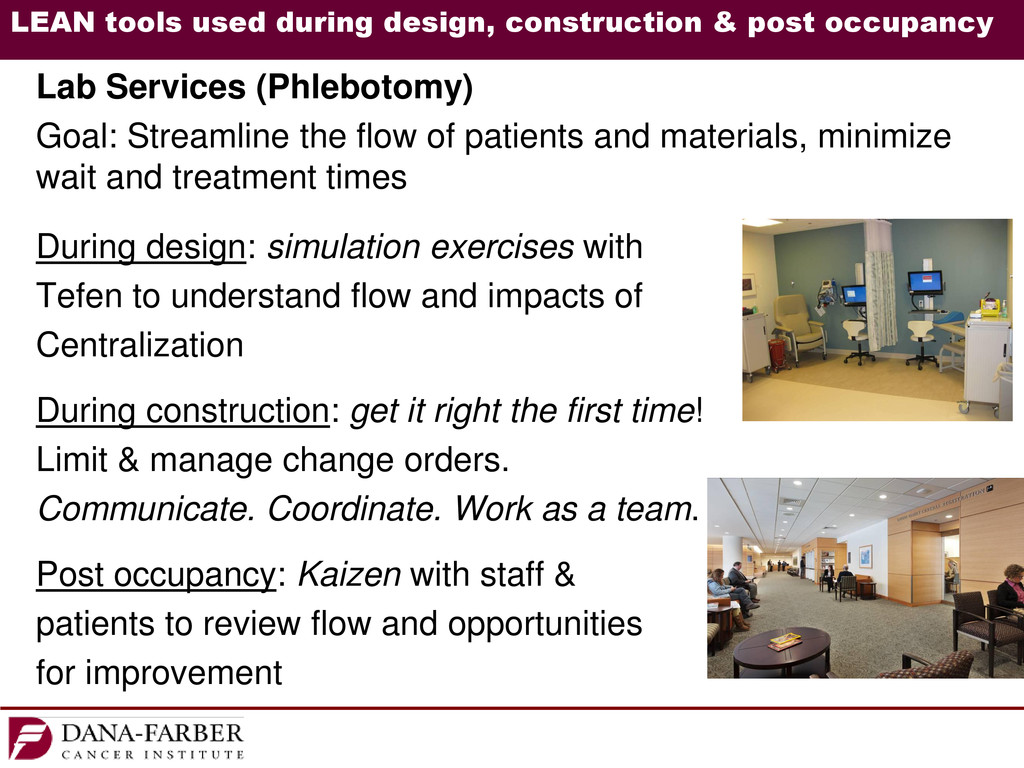
Services (Phlebotomy) Goal: Streamline the flow of patients and materials, minimize wait and treatment times During design: simulation exercises with Tefen to understand flow and impacts of Centralization During construction: get it right the first time! Limit & manage change orders. Communicate. Coordinate. Work as a team. Post occupancy: Kaizen with staff & patients to review flow and opportunities for improvement
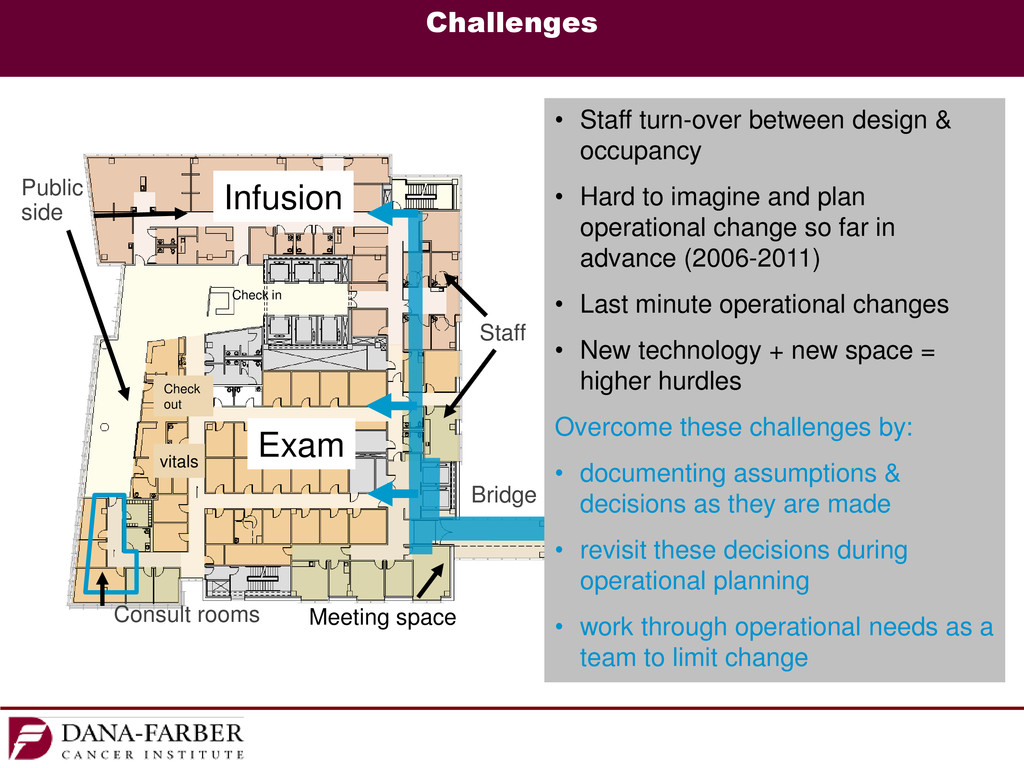
out Check in Challenges • Staff turn-over between design & occupancy • Hard to imagine and plan operational change so far in advance (2006-2011) • Last minute operational changes • New technology + new space = higher hurdles Overcome these challenges by: • documenting assumptions & decisions as they are made • revisit these decisions during operational planning • work through operational needs as a team to limit change Meeting space
• Press Ganey scores in the 90s - higher than ever! • Association of General Contractors (AGC) National Build America Award for “New: Construction Management” & AGC Build New England Honor Award • Boston Society of Architects (BSA) Healthcare Facilities Design Award 2013 • Construction Management Association of America (CMAA), New England Chapter, Project Achievement Award for New Building Construction over $200M • American Council of Engineering Companies of Massachusetts (ACEC/MA) Silver Engineering Excellence Award • Deep Foundations Institute National First Runner-up for the Outstanding Project Award • Modern Healthcare Design, Design Citation Award • International Interior Design Association New England (IIDA) – Healthcare Project Award • LEED Gold certification
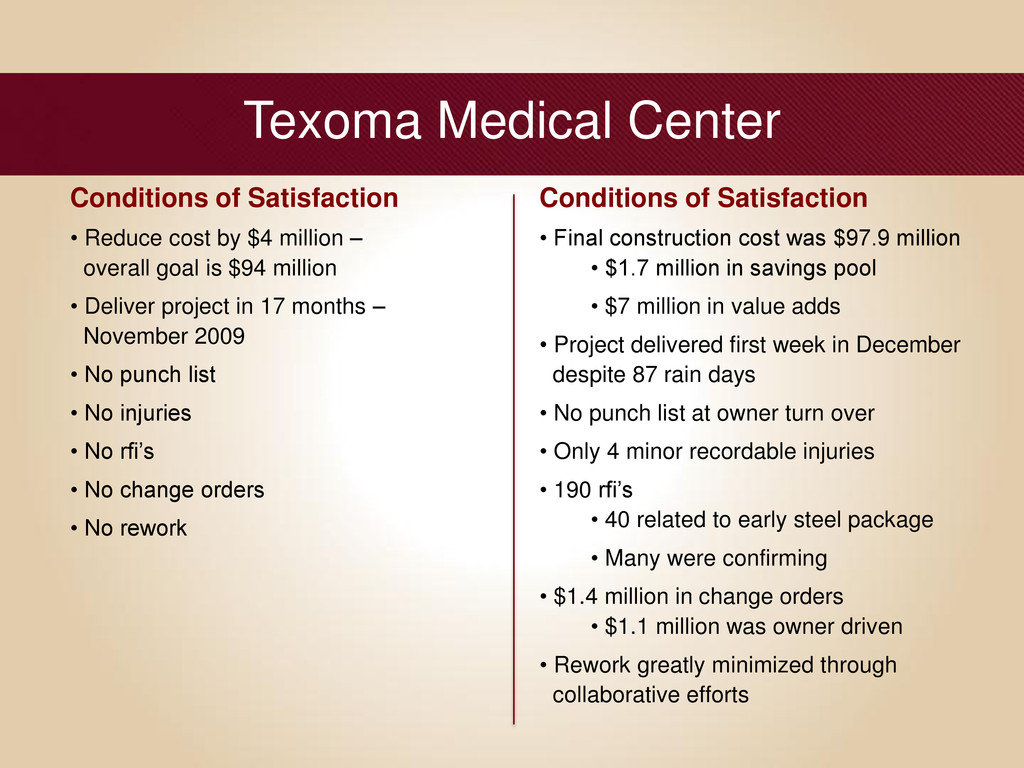
$4 million – overall goal is $94 million • Deliver project in 17 months – November 2009 • No punch list • No injuries • No rfi’s • No change orders • No rework Conditions of Satisfaction • Final construction cost was $97.9 million • $1.7 million in savings pool • $7 million in value adds • Project delivered first week in December despite 87 rain days • No punch list at owner turn over • Only 4 minor recordable injuries • 190 rfi’s • 40 related to early steel package • Many were confirming • $1.4 million in change orders • $1.1 million was owner driven • Rework greatly minimized through collaborative efforts
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}